

Difficult airway management in the emergency department.
Difficult airway management in the emergency department.
Difficult airway management in the emergency department.

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
32 S. L. Orebaugh<br />
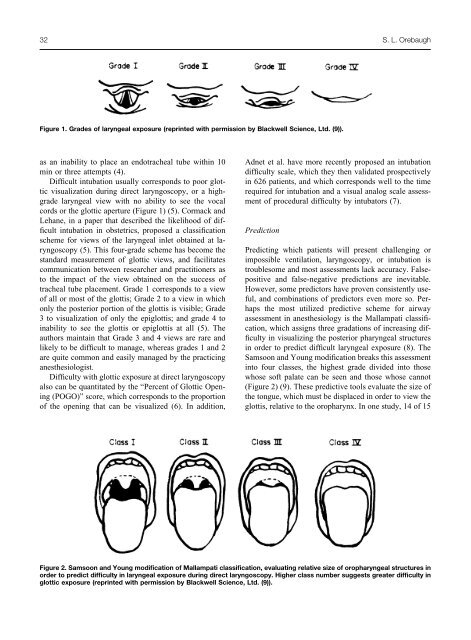
Figure 1. Grades of laryngeal exposure (repr<strong>in</strong>ted with permission by Blackwell Science, Ltd. (9)).<br />
as an <strong>in</strong>ability to place an endotracheal tube with<strong>in</strong> 10<br />
m<strong>in</strong> or three attempts (4).<br />
<strong>Difficult</strong> <strong>in</strong>tubation usually corresponds to poor glottic<br />
visualization dur<strong>in</strong>g direct laryngoscopy, or a highgrade<br />
laryngeal view with no ability to see <strong>the</strong> vocal<br />
cords or <strong>the</strong> glottic aperture (Figure 1) (5). Cormack and<br />
Lehane, <strong>in</strong> a paper that described <strong>the</strong> likelihood of difficult<br />
<strong>in</strong>tubation <strong>in</strong> obstetrics, proposed a classification<br />
scheme for views of <strong>the</strong> laryngeal <strong>in</strong>let obta<strong>in</strong>ed at laryngoscopy<br />
(5). This four-grade scheme has become <strong>the</strong><br />
standard measurement of glottic views, and facilitates<br />
communication between researcher and practitioners as<br />
to <strong>the</strong> impact of <strong>the</strong> view obta<strong>in</strong>ed on <strong>the</strong> success of<br />
tracheal tube placement. Grade 1 corresponds to a view<br />
of all or most of <strong>the</strong> glottis; Grade 2 to a view <strong>in</strong> which<br />
only <strong>the</strong> posterior portion of <strong>the</strong> glottis is visible; Grade<br />
3 to visualization of only <strong>the</strong> epiglottis; and grade 4 to<br />
<strong>in</strong>ability to see <strong>the</strong> glottis or epiglottis at all (5). The<br />
authors ma<strong>in</strong>ta<strong>in</strong> that Grade 3 and 4 views are rare and<br />
likely to be difficult to manage, whereas grades 1 and 2<br />
are quite common and easily managed by <strong>the</strong> practic<strong>in</strong>g<br />
anes<strong>the</strong>siologist.<br />
<strong>Difficult</strong>y with glottic exposure at direct laryngoscopy<br />
also can be quantitated by <strong>the</strong> “Percent of Glottic Open<strong>in</strong>g<br />
(POGO)” score, which corresponds to <strong>the</strong> proportion<br />
of <strong>the</strong> open<strong>in</strong>g that can be visualized (6). In addition,<br />
Adnet et al. have more recently proposed an <strong>in</strong>tubation<br />
difficulty scale, which <strong>the</strong>y <strong>the</strong>n validated prospectively<br />
<strong>in</strong> 626 patients, and which corresponds well to <strong>the</strong> time<br />
required for <strong>in</strong>tubation and a visual analog scale assessment<br />
of procedural difficulty by <strong>in</strong>tubators (7).<br />
Prediction<br />
Predict<strong>in</strong>g which patients will present challeng<strong>in</strong>g or<br />
impossible ventilation, laryngoscopy, or <strong>in</strong>tubation is<br />
troublesome and most assessments lack accuracy. Falsepositive<br />
and false-negative predictions are <strong>in</strong>evitable.<br />
However, some predictors have proven consistently useful,<br />
and comb<strong>in</strong>ations of predictors even more so. Perhaps<br />
<strong>the</strong> most utilized predictive scheme for <strong>airway</strong><br />
assessment <strong>in</strong> anes<strong>the</strong>siology is <strong>the</strong> Mallampati classification,<br />
which assigns three gradations of <strong>in</strong>creas<strong>in</strong>g difficulty<br />
<strong>in</strong> visualiz<strong>in</strong>g <strong>the</strong> posterior pharyngeal structures<br />
<strong>in</strong> order to predict difficult laryngeal exposure (8). The<br />
Samsoon and Young modification breaks this assessment<br />
<strong>in</strong>to four classes, <strong>the</strong> highest grade divided <strong>in</strong>to those<br />
whose soft palate can be seen and those whose cannot<br />
(Figure 2) (9). These predictive tools evaluate <strong>the</strong> size of<br />
<strong>the</strong> tongue, which must be displaced <strong>in</strong> order to view <strong>the</strong><br />
glottis, relative to <strong>the</strong> oropharynx. In one study, 14 of 15<br />
Figure 2. Samsoon and Young modification of Mallampati classification, evaluat<strong>in</strong>g relative size of oropharyngeal structures <strong>in</strong><br />
order to predict difficulty <strong>in</strong> laryngeal exposure dur<strong>in</strong>g direct laryngoscopy. Higher class number suggests greater difficulty <strong>in</strong><br />
glottic exposure (repr<strong>in</strong>ted with permission by Blackwell Science, Ltd. (9)).