Oregon Balance of State HIV/AIDS Housing & Services Systems ...
Oregon Balance of State HIV/AIDS Housing & Services Systems ...
Oregon Balance of State HIV/AIDS Housing & Services Systems ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Oregon</strong> <strong>Balance</strong> <strong>of</strong> <strong>State</strong><br />
<strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> & <strong>Services</strong><br />
<strong>Systems</strong> Integration Plan<br />
August 2008
The research, development, and publication <strong>of</strong> this plan was funded in part by the <strong>Housing</strong><br />
Opportunities for Persons with <strong>AIDS</strong> (HOPWA) National Technical Assistance Program in partnership<br />
with the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development's Office <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong>. The<br />
substance and findings <strong>of</strong> the work are dedicated to the public. The author and publisher are solely<br />
responsible for the accuracy <strong>of</strong> the statements and interpretations contained in this publication. Such<br />
interpretations do not necessarily reflect the views <strong>of</strong> the Government.<br />
Prepared for:<br />
<strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, <strong>HIV</strong> Care and Treatment<br />
<strong>Oregon</strong> <strong>Housing</strong> Opportunities in Partnership (OHOP)<br />
800 NE <strong>Oregon</strong> St., Suite 1105<br />
Portland, OR 97232<br />
Ryan Deibert<br />
OHOP Program Coordinator<br />
(971) 673-0145<br />
ryan.j.deibert@state.or.us<br />
Prepared in collaboration with:<br />
U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development<br />
Portland, <strong>Oregon</strong> Field Office<br />
400 S.W. Sixth Avenue, Suite 700<br />
Portland, OR 97204<br />
Doug Carlson<br />
CPD Field Office Director<br />
(971)222-2612<br />
doug_carlson@hud.gov<br />
Prepared by:<br />
Building Changes<br />
2014 East Madison, Suite 200<br />
Seattle, Washington 98122<br />
(206) 322-9444<br />
www.BuildingChanges.org<br />
Info@BuildingChanges.org
<strong>Oregon</strong> <strong>Balance</strong> <strong>of</strong> <strong>State</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong><br />
Integration Plan Steering Committee Members<br />
Sherri Alston<br />
Eastern <strong>Oregon</strong> Center for Independent Living<br />
Elizabeth Anguiano<br />
<strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Addictions &<br />
Mental Health<br />
Ann Brown<br />
<strong>Oregon</strong> <strong>Housing</strong> and Community <strong>Services</strong><br />
Carla Cary<br />
Mid-Willamette Valley Community Action Agency<br />
Vince Chiotti<br />
<strong>Oregon</strong> <strong>Housing</strong> and Community <strong>Services</strong><br />
John Delco<br />
Community Member<br />
Nancy Donovan<br />
U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development<br />
Joy Hirl<br />
Formerly <strong>of</strong> U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban<br />
Development<br />
<strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong><br />
Vic Fox<br />
Program Manager,<br />
<strong>HIV</strong> Care and<br />
Treatment<br />
Renee Yandell<br />
<strong>Housing</strong> Coordinator, OHOP<br />
Ryan Deibert<br />
Program Coordinator,<br />
<strong>Oregon</strong> <strong>Housing</strong><br />
Opportunities in<br />
Partnership (OHOP)<br />
Kristin Kane<br />
Cascade <strong>AIDS</strong> Project<br />
Dawn Martin<br />
Portland Bureau <strong>of</strong> <strong>Housing</strong> and Community<br />
Development<br />
Pegge McGuire<br />
<strong>Oregon</strong> <strong>Housing</strong> and Community <strong>Services</strong><br />
Wayne Miya<br />
Our House <strong>of</strong> Portland<br />
Scott Rich<br />
U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development<br />
Stan Stradley<br />
<strong>Housing</strong> Authority <strong>of</strong> the County <strong>of</strong> Umatilla<br />
Richie Weinman<br />
City <strong>of</strong> Eugene<br />
Annick Benson<br />
Support <strong>Services</strong><br />
Manager, <strong>HIV</strong> Care<br />
and Treatment<br />
Program<br />
Building Changes / <strong>AIDS</strong> <strong>Housing</strong> <strong>of</strong> Washington<br />
Katherine Cortes<br />
Community Planner<br />
Rachel Moorhead<br />
Training and Publications<br />
Coordinator<br />
Charlie Corrigan<br />
Community Planner<br />
Jessica Pemble<br />
Administrative Assistant<br />
Denise Fry<br />
<strong>Housing</strong> Coordinator,<br />
OHOP<br />
Mark Putnam<br />
Manager <strong>of</strong> Community<br />
Initiatives
Key Stakeholders<br />
ACCESS, Inc.<br />
Edward Angeletti<br />
Cindy Dyer<br />
Ellen Gray<br />
<strong>Housing</strong> and Community <strong>Services</strong> Agency (HACSA)<br />
<strong>of</strong> Lane County<br />
Larry Abel<br />
Craig Satein<br />
<strong>Housing</strong> Authority <strong>of</strong> Jackson County<br />
Cara Carter<br />
Scott Foster<br />
Christie Van Aken<br />
Jackson County Health and Human <strong>Services</strong><br />
Billie Arnold<br />
Mark Ornd<strong>of</strong>f<br />
Al Solovich<br />
Lane County Human <strong>Services</strong> Commission<br />
Pearle Wolfe<br />
Lincoln County Board <strong>of</strong> Commissioners<br />
Bill Hall<br />
Neighbor Impact<br />
Corky Senecal<br />
<strong>Oregon</strong> Department <strong>of</strong> Corrections<br />
Ginger Martin<br />
<strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Addictions<br />
and Mental Health<br />
Vicki Skryha<br />
<strong>Oregon</strong> <strong>Housing</strong> Opportunities in Partnership<br />
(OHOP) Program<br />
Jakki Calhoun<br />
Portland Bureau <strong>of</strong> <strong>Housing</strong> and Community<br />
Development<br />
Heather Lyons<br />
Salem <strong>Housing</strong> Authority<br />
Jerry Cr<strong>of</strong>t<br />
Esther Reinecke<br />
ShelterCare<br />
Erin Bonner<br />
Chris Steele<br />
St. Vincent de Paul Lane County<br />
Anne Williams<br />
U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban<br />
Development<br />
Doug Carlson
Table <strong>of</strong> Contents<br />
Executive Summary....................................................................................................................... i<br />
Overview <strong>of</strong> the <strong>Systems</strong> Integration Assessment and Planning Process .................................. ii<br />
Critical Issues and Recommendations .......................................................................................iii<br />
Context <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> in <strong>Oregon</strong> <strong>Balance</strong> <strong>of</strong> <strong>State</strong> ..................................................... 1<br />
<strong>Oregon</strong> <strong>Housing</strong> and Opportunities in Partnership (OHOP) Program ....................................... 1<br />
Demographics and Epidemiology............................................................................................... 4<br />
Poverty, <strong>Housing</strong>, and Homelessness in <strong>Oregon</strong>...................................................................... 10<br />
Integration <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Services</strong> and <strong>Housing</strong> with Existing <strong>Systems</strong>................................ 17<br />
Outreach Strategies ................................................................................................................... 17<br />
Health Care (including <strong>HIV</strong> Care)............................................................................................ 19<br />
Affordable <strong>Housing</strong> Resources................................................................................................. 21<br />
Homeless <strong>Services</strong> and Prevention ........................................................................................... 29<br />
Addictions and Mental Health <strong>Services</strong>.................................................................................... 31<br />
Human <strong>Services</strong> and Public Assistance .................................................................................... 33<br />
Employment.............................................................................................................................. 34<br />
Criminal Justice ........................................................................................................................ 35<br />
Critical Issues .............................................................................................................................. 41<br />
Outreach and Partnership Development ................................................................................... 41<br />
Integration with <strong>Housing</strong> and Service <strong>Systems</strong> ........................................................................ 42<br />
Recommendations....................................................................................................................... 49<br />
Outreach and Partnership Development ................................................................................... 49<br />
Integration with <strong>Housing</strong> and Service <strong>Systems</strong> ........................................................................ 51<br />
APPENDICES<br />
Appendix 1: Affordable <strong>Housing</strong> Resource Guide ................................................................ A-1<br />
Appendix 2: Stakeholder Survey Results ............................................................................. A-35<br />
Appendix 3: <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> Options ............................................................................ A-41<br />
Appendix 4: Federal and <strong>State</strong> Financing Sources for Affordable <strong>Housing</strong>..................... A-49<br />
Appendix 5: Glossary <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong>- and <strong>Housing</strong>-Related Terms ................................... A-57
Table <strong>of</strong> Figures and Tables<br />
Figure 1: OHOP Service Regions in the <strong>Balance</strong> <strong>of</strong> <strong>State</strong>.............................................................. ii<br />
Table 1: Summary <strong>of</strong> OHOP Grants............................................................................................... 3<br />
Table 2: Total Population (2006) and Number <strong>of</strong> People Living with <strong>HIV</strong>/<strong>AIDS</strong> (2007) for<br />
Counties in the <strong>Balance</strong> <strong>of</strong> <strong>State</strong> ............................................................................................. 7<br />
Table 3: Demographics for the <strong>State</strong> <strong>of</strong> <strong>Oregon</strong> (as <strong>of</strong> July 2006) and for People Living<br />
with <strong>HIV</strong> and <strong>AIDS</strong> in <strong>Oregon</strong> (as <strong>of</strong> March 2007) ............................................................... 9<br />
Table 4: People Living with <strong>HIV</strong> and <strong>AIDS</strong> as <strong>of</strong> March 2007 in <strong>Oregon</strong> by Exposure<br />
Category................................................................................................................................ 10<br />
Table 5: 2006-2008 Fair Market Rents for One-Bedroom Unit for <strong>Oregon</strong> Counties in<br />
<strong>Balance</strong> <strong>of</strong> <strong>State</strong> .................................................................................................................... 14<br />
Table 6: CDBG and HOME Allocations for <strong>Oregon</strong> <strong>Balance</strong> <strong>of</strong> <strong>State</strong>, Fiscal Year 2007 ........... 24<br />
Table 7: Public <strong>Housing</strong> and Section 8 Resources for <strong>Oregon</strong> <strong>Housing</strong> Authorities ................... 26<br />
Table 8: Continuum <strong>of</strong> Care Funding Allocations for Fiscal Year 2006...................................... 30
Executive Summary—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan i<br />
Executive Summary<br />
This Executive Summary includes a statement <strong>of</strong> the purpose behind this systems integration plan,<br />
an overview <strong>of</strong> the needs assessment and planning process, key findings, and critical issues that<br />
were identified and recommendations that were developed by the Steering Committee.<br />
Many people living with <strong>HIV</strong>/<strong>AIDS</strong>, at some point during their illness, find themselves in need <strong>of</strong><br />
housing assistance and support services. Stable housing promotes improved health, sobriety or<br />
decreased use <strong>of</strong> alcohol and illegal drugs, and, for some, a return to paid employment and<br />
productive social activities. As the number <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong> continues to grow in<br />
both urban and rural areas throughout the United <strong>State</strong>s, stakeholders must find new ways to<br />
address their needs to promote the health and well-being <strong>of</strong> these individuals and their families.<br />
Increasingly, maximizing the resources available to people who need them requires partnering<br />
across mainstream housing and human services systems to ensure continuity <strong>of</strong> care, program<br />
efficiency, and that there is “no wrong door” to assistance for clients at risk.<br />
In order to improve the ability <strong>of</strong> the <strong>State</strong> <strong>of</strong> <strong>Oregon</strong> to establish and sustain such partnerships, the<br />
U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development (HUD) funded the development <strong>of</strong> the <strong>Oregon</strong><br />
<strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan in August 2007. The plan was facilitated<br />
by Building Changes (formerly <strong>AIDS</strong> <strong>Housing</strong> <strong>of</strong> Washington), a national <strong>HIV</strong>/<strong>AIDS</strong> housing<br />
technical assistance provider based in Seattle. Building Changes worked closely with the <strong>Oregon</strong><br />
Department <strong>of</strong> Human <strong>Services</strong>, the grantee for HUD’s <strong>Housing</strong> Opportunities for Persons with<br />
<strong>AIDS</strong> (HOPWA) program for <strong>Oregon</strong> <strong>State</strong> outside <strong>of</strong> the five-county Portland metropolitan area.<br />
This area is referred to as the <strong>Oregon</strong> “balance <strong>of</strong> state.”<br />
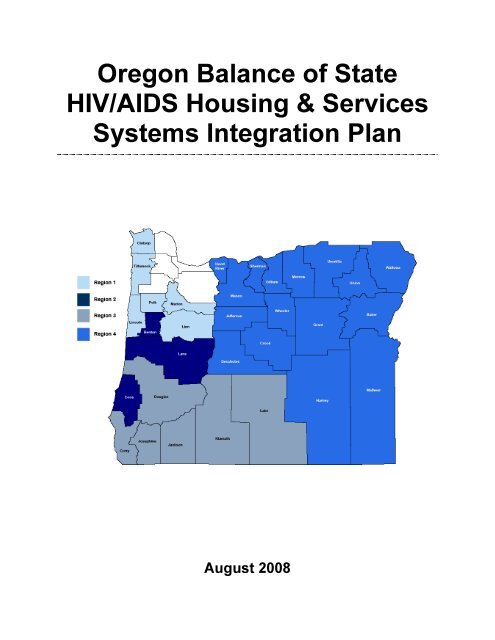
The <strong>Oregon</strong> <strong>Housing</strong> Opportunities in Partnership (OHOP) program has been administered by the<br />
<strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Public Health, <strong>HIV</strong>/STD/TB Section, <strong>HIV</strong> Care and<br />
Treatment program (<strong>HIV</strong> Care and Treatment) since 2002. The four OHOP <strong>Housing</strong> Coordinators<br />
serve four regions <strong>of</strong> the balance <strong>of</strong> state.<br />
Figure 1 on the following page shows a map <strong>of</strong> the four OHOP service regions.
ii Executive Summary—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Figure 1:<br />
OHOP Service Regions in the <strong>Balance</strong> <strong>of</strong> <strong>State</strong><br />
In addition to the formula funds that the <strong>State</strong> receives based on the number <strong>of</strong> residents living with<br />
<strong>HIV</strong>/<strong>AIDS</strong>, <strong>HIV</strong> Care and Treatment concurrently administers competitive HOPWA funding<br />
awarded by HUD in previous funding cycles, including two HOPWA Special Projects <strong>of</strong> National<br />
Significance (SPNS) addressing formerly incarcerated people and people with co-occurring mental<br />
illness, respectively. HOPWA fund administration is further described in the first chapter <strong>of</strong> the<br />
main report, “Context <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> in <strong>Oregon</strong> <strong>Balance</strong> <strong>of</strong> <strong>State</strong>.” Since 2002, OHOP has<br />
provided services to nearly 400 unduplicated people living with <strong>HIV</strong>/<strong>AIDS</strong>. OHOP currently<br />
maintains a wait list <strong>of</strong> about 50 eligible clients.<br />
Overview <strong>of</strong> the <strong>Systems</strong> Integration Assessment and Planning Process<br />
The <strong>HIV</strong>/<strong>AIDS</strong> housing and services systems integration assessment (conducted between fall 2007<br />
and spring 2008) provided an opportunity for more than 60 community members to give input,<br />
discuss, and identify critical issues and strategies for enhancing and integrating <strong>HIV</strong>/<strong>AIDS</strong> housing<br />
and services across the <strong>Oregon</strong> balance <strong>of</strong> state. The process was guided by a Steering Committee<br />
that included a broad cross-section <strong>of</strong> representatives <strong>of</strong> <strong>State</strong> and city agencies, nonpr<strong>of</strong>it service<br />
providers, housing authorities, community action agencies, and a person living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
Stakeholders from each <strong>of</strong> the four OHOP regions participated in the process, through interviews, a<br />
survey, and/or Steering Committee membership.
Executive Summary—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan iii<br />
The <strong>Systems</strong> Integration Plan includes a summary <strong>of</strong> the OHOP program as a regional <strong>HIV</strong>/<strong>AIDS</strong><br />
resource; research on demographic patterns, <strong>HIV</strong>/<strong>AIDS</strong> epidemiology, economic factors, housing<br />
and homelessness among people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong>’s balance <strong>of</strong> state; and<br />
descriptions <strong>of</strong> key features <strong>of</strong> an array <strong>of</strong> interrelated housing and service systems across <strong>Oregon</strong>.<br />
Among the key findings <strong>of</strong> this research is the great need for housing for people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong>. Forty percent <strong>of</strong> <strong>Oregon</strong>ians with <strong>HIV</strong> need housing assistance, and a survey <strong>of</strong> <strong>Oregon</strong><br />
service agency representatives cited the lack <strong>of</strong> affordable housing as the number-one barrier to<br />
stability for <strong>Oregon</strong>ians living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
For greater detail on the findings <strong>of</strong> each aspect <strong>of</strong> the research, please see the “Context <strong>of</strong><br />
<strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong>” and “Integration <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Services</strong> and <strong>Housing</strong> with Existing <strong>Systems</strong>”<br />
sections <strong>of</strong> the Plan. Based on these findings, the Steering Committee identified critical issues and<br />
developed recommendations to improve the ability <strong>of</strong> these systems to cooperatively meet the<br />
housing and services needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong>.<br />
Critical Issues and Recommendations<br />
The <strong>Oregon</strong> <strong>HIV</strong> <strong>Housing</strong> and Service <strong>Systems</strong> Integration Plan Steering Committee met twice in<br />
Salem, <strong>Oregon</strong>, and also by telephone conference, to review findings from the assessment <strong>of</strong><br />
<strong>HIV</strong>/<strong>AIDS</strong> resources and systems integration conducted by Building Changes. Based on these<br />
findings, the Committee identified critical issues in systems integration that pose challenges to<br />
meeting the housing and related needs <strong>of</strong> people living with <strong>HIV</strong> and <strong>AIDS</strong> in the state <strong>of</strong> <strong>Oregon</strong><br />
(outside <strong>of</strong> the Portland metropolitan area). The Committee then sought to develop strategic<br />
recommendations that addressed the critical issues.<br />
Among the critical issues, the Committee identified both general issues related to the outreach and<br />
partnership strategies <strong>of</strong> the OHOP program, and issues specific to the various housing and service<br />
systems which should be involved in an integrated <strong>HIV</strong> housing and service plan for <strong>Oregon</strong><br />
residents. One or more recommendations were developed to correspond to each type <strong>of</strong> issue and<br />
system. For greater detail on each <strong>of</strong> these issues and recommendations, please read the “Critical<br />
Issues” and “Recommendations and Strategies” section <strong>of</strong> the complete Plan.<br />
Critical Issues<br />
Outreach and Partnership Development<br />
1. Limited Awareness <strong>of</strong> Resources Dedicated to People Living with <strong>HIV</strong>/<strong>AIDS</strong><br />
Many potential housing and services partners lack awareness or accurate knowledge <strong>of</strong> existing<br />
resources dedicated to, or which can be used to serve, people living with <strong>HIV</strong>/<strong>AIDS</strong>, and that lack<br />
<strong>of</strong> awareness may limit partnerships.<br />
2. Confidentiality Concerns<br />
The need to maintain client confidentiality restricts the ways that OHOP housing coordinators and<br />
other organizations and individuals can publicize their activities and resources.<br />
3. Limited Staff Capacity and Knowledge
iv Executive Summary—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
OHOP and <strong>HIV</strong> Care and Treatment staff may lack familiarity with aspects <strong>of</strong> partner systems,<br />
including affordable housing, and have limited resources and time to conduct marketing and<br />
outreach to potential partners and planning bodies.<br />
Recommendations<br />
• Develop simple, discreet material to publicize OHOP and related services and opportunities, and<br />
disseminate widely.<br />
• Present to current and potential partners, including faith-based and community-based grass roots<br />
organizations with information tailored to their interests.<br />
• Engage provider agency staff, clients, and other regional participants in publicizing the need,<br />
opportunity, and benefits <strong>of</strong> investing in housing and services for people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
• Offer trainings and create forums for sharing best practices to build OHOP and partner staff<br />
capacity.<br />
Individualized <strong>Housing</strong> and Service System Approaches<br />
Affordable <strong>Housing</strong> Resources<br />
4. Prioritizing Participation among Many Planning and Implementation Processes<br />
Mechanisms for community input are frequently built in to affordable housing planning processes,<br />
but it can be difficult for OHOP staff and partners to track the time-limited windows to provide such<br />
input, as well as to prioritize in which meetings and processes their participation will be most<br />
effective and conducive to cooperative ventures.<br />
5. Maximizing Access to New Resources for Special Populations<br />
Steering Committee members noted that affordable housing funders and developers are asked to<br />
prioritize or include a variety <strong>of</strong> special population definitions and set-asides in their projects or<br />
guidelines. Affordable housing resources are limited across the balance <strong>of</strong> state, resulting in strong<br />
competition for funding opportunities.<br />
6. Understanding Affordable <strong>Housing</strong> System Missions and Cultures<br />
Stakeholders in the affordable housing “system” have interests and goals that vary from entity to<br />
entity and may not be clear to OHOP stakeholders or consistent with goals <strong>of</strong> expanding access to<br />
housing by people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
Recommendations<br />
• Participate consistently in the statewide Consolidated Plan, Continuum <strong>of</strong> Care, and other<br />
planning processes.<br />
• Prioritize strategically between building on existing relationships or seeking new partnerships<br />
with affordable housing developers and providers, neighborhood associations, and faith-based<br />
organizations.<br />
• Seek housing development opportunities in which relatively modest <strong>HIV</strong>/<strong>AIDS</strong>-specific<br />
resources can leverage significant investment from other sources.
Executive Summary—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan v<br />
Homeless <strong>Services</strong><br />
7. Lack <strong>of</strong> Shared Data and Coordinated Planning Between <strong>HIV</strong>/<strong>AIDS</strong> and Homeless<br />
<strong>Systems</strong><br />
Limited data is available on the overlap between the challenges <strong>of</strong> homelessness and <strong>HIV</strong>/<strong>AIDS</strong>,<br />
and information systems are not well integrated on the client or systems levels. As a result, clients<br />
risk falling through the cracks and not receiving referrals for needed services.<br />
8. Incomplete Integration <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> Issues into Continua <strong>of</strong> Care<br />
Steering Committee members identified the need for more meaningful inclusion <strong>of</strong> the needs <strong>of</strong><br />
people living with <strong>HIV</strong>/<strong>AIDS</strong> in Continuum <strong>of</strong> Care planning, including through participation by<br />
<strong>HIV</strong>/<strong>AIDS</strong> system stakeholders in Continuum meetings, and the pursuit <strong>of</strong> additional Shelter Plus<br />
Care projects across the state.<br />
Recommendations<br />
• Focus attention on improving coordination with planning, data, and other elements <strong>of</strong> homeless<br />
systems.<br />
• Promote Shelter Plus Care and other bonus projects through agreements to streamline or share<br />
sponsor administrative costs.<br />
• Conduct outreach and seek partnerships with landlords and property managers.<br />
Addictions and Mental Health<br />
9. Addictions and Mental Health <strong>Services</strong> Gap<br />
The Steering Committee saw a significant gap in services for addictions and mental health services<br />
among people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong>’s balance <strong>of</strong> state.<br />
10. Limited Access by People Living with <strong>HIV</strong>/<strong>AIDS</strong> to Mainstream Behavioral Health<br />
<strong>Services</strong><br />
Steering Committee members noted that limited statewide development funds to serve people with<br />
behavioral health issues and unmet housing needs have not to date supported developments wholly<br />
or partially dedicated to people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
Recommendations<br />
• Partner with substance abuse and mental health service providers to spotlight need and seek<br />
expanded support for these services.<br />
• Build relationships with behavioral health crisis providers.<br />
Human <strong>Services</strong> and Public Assistance<br />
11. Loss and Scarcity <strong>of</strong> Funding for Human <strong>Services</strong><br />
The budgets <strong>of</strong> local agencies that provide the bulk <strong>of</strong> human services in <strong>Oregon</strong> have been hard-hit<br />
(especially in smaller, more rural counties) by the loss <strong>of</strong> timber revenues and other challenges. The<br />
number <strong>of</strong> promising “one-stop” centers in which multiple agencies coordinate their services has<br />
dwindled.
vi Executive Summary—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
12. Family Support Needs<br />
A substantial number <strong>of</strong> family households impacted by <strong>HIV</strong>/<strong>AIDS</strong>, which have diverse and unique<br />
needs as compared to individuals, require housing and services support. While HOPWA funds can<br />
be used to serve households as well as individuals, various program activities (discussed further in<br />
Appendix 3: <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> Options) may be more or less appropriate for family groups.<br />
Recommendation<br />
• Prioritize education and outreach to local DHS <strong>of</strong>fices and community action agencies around<br />
<strong>HIV</strong>/<strong>AIDS</strong> and client issues, and support coordinated service delivery models.<br />
Criminal Justice<br />
13. Lack <strong>of</strong> <strong>Housing</strong> Options<br />
Offenders living with <strong>HIV</strong>/<strong>AIDS</strong> are screened out <strong>of</strong> public and private housing by background<br />
checks, and can find it difficult to transition to mainstream housing assistance programs such as<br />
Section 8, even if they are successfully housed with OHOP assistance.<br />
14. Multiple Risk Factors<br />
The inter-related risk factors that are commonly found among <strong>of</strong>fenders translate into high service<br />
needs – and gaps in receiving services – when prisoners return to the community.<br />
Recommendation<br />
• Pursue partnerships with local and state criminal justice agencies and stakeholders, including<br />
grass roots community- and faith-based organizations, and seek federal and other resources to<br />
serve people with incarceration histories.<br />
Primary Care, Hospitals and Assisted Living<br />
15. Lack <strong>of</strong> Research and Resources for People Living with <strong>HIV</strong>/<strong>AIDS</strong><br />
Steering Committee members identified a need for more assisted living and long-term care options<br />
(including in-home assistance) for both <strong>HIV</strong>-positive people living longer, and those suffering from<br />
chronic diseases like diabetes which provider observation suggests emerge earlier and more<br />
frequently among people with <strong>HIV</strong> than in the general population.<br />
16. Additional <strong>Housing</strong> Challenges<br />
Holding housing units and maintaining housing assistance as people cycle in and out <strong>of</strong> assisted<br />
living situations can be difficult, and can require modifications to facility or agency rules and incur<br />
additional administrative costs. The difficulty <strong>of</strong> placing clients in assisted living is broader than the<br />
<strong>HIV</strong>/<strong>AIDS</strong> population and is a challenge statewide.<br />
Recommendations<br />
• Consider that clients may need periodic or long-term care in assisted living situations while<br />
setting OHOP policies and allocating resources.<br />
• Conduct outreach about emerging primary care and assisted living needs <strong>of</strong> people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong>, including to providers <strong>of</strong> these services.
Executive Summary—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan vii<br />
Employment<br />
17. Limited Coordination among Employment, Service, and <strong>Housing</strong> <strong>Systems</strong><br />
The level <strong>of</strong> coordination between OHOP and its partners and employment services providers in the<br />
balance <strong>of</strong> state falls short <strong>of</strong> meeting the level <strong>of</strong> need for employment assistance among people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
Recommendation<br />
• Collaborate with workforce systems to provide employment supports and training for people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong>.
Section 1: Summary <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong><br />
<strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong><br />
Integration
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 1<br />
Context <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> in <strong>Oregon</strong> <strong>Balance</strong> <strong>of</strong><br />
<strong>State</strong><br />
This section provides an overview <strong>of</strong> the OHOP program and describes the overall context for<br />
<strong>HIV</strong>/<strong>AIDS</strong> housing and services in the balance <strong>of</strong> state.<br />
<strong>Oregon</strong> <strong>Housing</strong> and Opportunities in Partnership (OHOP) Program<br />
Many people living with <strong>HIV</strong>/<strong>AIDS</strong> find themselves in need <strong>of</strong> housing assistance and support<br />
services at some point during their illness. As many as 60 percent <strong>of</strong> all persons living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> report a lifetime experience <strong>of</strong> homelessness or housing instability. 1 Stable housing<br />
promotes improved health, sobriety or decreased use <strong>of</strong> alcohol and illegal drugs, and, for some<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong>, a return to paid employment and productive social activities.<br />
The federal <strong>Housing</strong> Opportunities for Persons with <strong>AIDS</strong> (HOPWA) program provides funding,<br />
distributed by both formula and competition, dedicated to the housing needs <strong>of</strong> people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> and their families. In <strong>Oregon</strong>, HOPWA funds are allocated separately to the Portland<br />
Eligible Metropolitan Area (EMA)—Clackamas, Columbia, Multnomah, Washington, and Yamhill<br />
Counties in <strong>Oregon</strong>, and Clark County, Washington—and the rest <strong>of</strong> the state <strong>of</strong> <strong>Oregon</strong> (referred to<br />
as the “balance <strong>of</strong> state”). These two regions (metro Portland and the balance <strong>of</strong> state) each receive a<br />
portion <strong>of</strong> HOPWA formula funding and may compete for additional funding against other<br />
metropolitan and statewide regions defined by HUD.<br />
The <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Public Health, <strong>HIV</strong>/STD/TB Section, <strong>HIV</strong> Care and<br />
Treatment program (<strong>HIV</strong> Care and Treatment) has provided HOPWA-funded housing services in the<br />
balance <strong>of</strong> state through the <strong>Oregon</strong> <strong>Housing</strong> Opportunities in Partnership (OHOP) program since<br />
2002. The four OHOP <strong>Housing</strong> Coordinators serve four defined regions <strong>of</strong> the balance <strong>of</strong> state.<br />
Figure 1 on the following page shows a map <strong>of</strong> the four OHOP service regions.<br />
1 Aidala, A., Columbia University. Homelessness, <strong>Housing</strong> Instability and <strong>Housing</strong> Problems among Persons Living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
Paper presented at the <strong>Housing</strong> and <strong>HIV</strong>/<strong>AIDS</strong> Research Summit, June, 2005. Available online:<br />
http://www.nationalaidshousing.org/toolkit/sound_investment.pdf (Accessed: February 21, 2008).
2 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Figure 1:<br />
OHOP Service Regions in the <strong>Balance</strong> <strong>of</strong> <strong>State</strong><br />
<strong>Housing</strong> Coordinators provide an array <strong>of</strong> HOPWA eligible housing services for people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> with incomes below 80 percent <strong>of</strong> Area Median Income (AMI), including Tenant-Based<br />
Rental Assistance (TBRA), Short-Term Rental, Mortgage, and Utilities (STRMU) assistance, and<br />
housing information and referrals. (A discussion <strong>of</strong> eligible activities defined by the HOPWA<br />
program, and complementary activities that may be funded by other sources, is in Appendix 3:<br />
<strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> Options.) Since 2002, OHOP has provided services to nearly 400 unduplicated<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong>. OHOP currently maintains a wait list <strong>of</strong> about 50 eligible clients.<br />
HOPWA formula funds are distributed to two types <strong>of</strong> grantees: eligible metropolitan areas (EMAs)<br />
with populations <strong>of</strong> more than 500,000 and at least 1,500 cumulative <strong>AIDS</strong> cases, and states with<br />
more than 1,500 cumulative <strong>AIDS</strong> cases for areas outside <strong>of</strong> EMAs. In addition to these formula<br />
funds, HOPWA competitive program funds are awarded to model projects or programs based on<br />
their strategies, effectiveness, and ability to be replicated. Although OHOP was initially funded<br />
through a competitive grant, the state <strong>of</strong> <strong>Oregon</strong> became eligible for HOPWA formula funding in<br />
2006 in recognition <strong>of</strong> the growing epidemic outside the Portland area. This formula funding<br />
replaces OHOP’s competitive grant, which expires in July 2008.<br />
<strong>Oregon</strong> has been awarded two competitive HOPWA Special Projects <strong>of</strong> National Significance<br />
(SPNS) that are administered concurrently with the state’s formula funds. In 2006, HUD awarded<br />
funding for a SPNS project focused on formerly incarcerated people living with <strong>HIV</strong>/<strong>AIDS</strong>. The
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 3<br />
<strong>Oregon</strong> <strong>State</strong>wide Supportive Community Re-entry (OSSCR) project is a statewide initiative that is<br />
administered in areas outside <strong>of</strong> the Portland metropolitan area by OHOP (within the Portland area,<br />
OSSCR is administered by Cascade <strong>AIDS</strong> Project). Clients are referred by <strong>Oregon</strong> Department <strong>of</strong><br />
Corrections and local criminal justice agencies, and work closely with OHOP <strong>Housing</strong> Coordinators<br />
and <strong>HIV</strong> Care and Treatment Case Managers to develop housing plans that are integrated with other<br />
supportive service and community corrections plans. The OSSCR program includes TBRA funding<br />
for about 55 clients per year, including 20 in the Portland EMA, and 35 throughout the rest <strong>of</strong><br />
<strong>Oregon</strong>.<br />
In 2007, <strong>Oregon</strong> was again successful in receiving a SPNS award for the new <strong>Oregon</strong> <strong>Housing</strong> and<br />
Behavioral Health Initiative (OHBHI), which will serve people living with <strong>HIV</strong>/<strong>AIDS</strong> along the<br />
Interstate 5 corridor who have co-occurring mental illness. Outside <strong>of</strong> the Portland EMA, OHOP<br />
<strong>Housing</strong> Coordinators will provide housing services and Cascadia Behavioral Health will provide<br />
coordinated mental health and addictions services. (Inside the Portland EMA, these services will be<br />
provided by Cascade <strong>AIDS</strong> Project.) The OHBHI program includes TBRA funding for about 35<br />
clients per year, including 24 in the balance <strong>of</strong> state and about 11 in the Portland EMA.<br />
Table 1 summarizes the four current HOPWA grants that comprise the OHOP program. Annual<br />
budgets and TBRA goals are approximate and may vary as grants carry over between years.<br />
Formula HOPWA Grant<br />
Table 1:<br />
Summary <strong>of</strong> OHOP Grants<br />
Grant Grant Period<br />
Competitive (Prior to Formula<br />
Grantee Status)<br />
OSSCR SPNS<br />
OHBHI SPNS<br />
Every Calendar<br />
Year<br />
July 2005 to June<br />
2008<br />
January 2006 to<br />
December 2008<br />
January 2008 to<br />
December 2010<br />
Annual BoS<br />
Budget<br />
Annual BoS<br />
TBRA Goals<br />
$307,490 26<br />
$442,968 40<br />
$277,658 35<br />
$166,267 24<br />
Source: Information provided by <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, <strong>HIV</strong> Treatment and Care Program.<br />
Note: No totals are provided as budget periods differ, and TBRA goals may not be cumulative.<br />
HOPWA program strategy is guided in part by the participation <strong>of</strong> grantees in their local<br />
Consolidated Plans and in Continuum <strong>of</strong> Care planning, as well as by HOPWA program goals and<br />
rules; these processes are discussed further in “Integration <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Services</strong> and <strong>Housing</strong> with<br />
Existing <strong>Systems</strong>,” beginning on page 21 (Consolidated Plan) and page 29 (Continuum <strong>of</strong> Care).<br />
The Steering Committee guiding this Plan felt that including comparative information from nearby<br />
regions could help <strong>Oregon</strong> to contextualize various potential program approaches and set<br />
benchmarks to measure success; such information is therefore included here and throughout this<br />
section <strong>of</strong> the Plan. The Portland EMA contains more than three-quarters <strong>of</strong> the people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong>, and received $943,000 (more than three times the formula funding for the<br />
state <strong>of</strong> <strong>Oregon</strong>) in HOPWA formula funding in 2007.
4 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Formula funds were distributed similarly in <strong>Oregon</strong>’s neighbor to the north: the Seattle EMA<br />
received $1.6 million in HOPWA formula funds in 2007. 2 In addition, the state <strong>of</strong> Washington<br />
received slightly more than a third <strong>of</strong> that amount, or $622,000, to address people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> throughout the balance <strong>of</strong> state. 3<br />
The OHOP program has been particularly successful in securing competitive HOPWA funding in<br />
recent years. Neighboring jurisdictions have also received competitive grants. Our House <strong>of</strong><br />
Portland, in the Portland EMA, received a three-year, $1.04 million HOPWA competitive grant for<br />
housing placement, TBRA, and supportive services such as acute care. The Washington balance <strong>of</strong><br />
state received a three-year, $1.15 million HOPWA competitive grant serving eastern Washington. 4<br />
In 2006, a DHS evaluation <strong>of</strong> the OHOP program found that nine out <strong>of</strong> ten clients reported<br />
satisfaction with their current housing, and 89 percent said their housing situation had improved<br />
since having a <strong>Housing</strong> Coordinator. The evaluation stated that landlords were also satisfied with<br />
the program’s performance and were generally willing to accept additional OHOP clients. 5<br />
The evaluation indentified two main challenges for the OHOP program. The extended housing<br />
authority wait lists for Section 8 <strong>Housing</strong> Choice Vouchers limited the ability <strong>of</strong> the OHOP program<br />
to transition clients to mainstream housing resources and serve more eligible people on the OHOP<br />
wait list. A second challenge was serving clients with multiple barriers, such as mental illness,<br />
substance use, or felony histories. Following the evaluation, <strong>Oregon</strong> has sought to address the<br />
challenges <strong>of</strong> serving clients with multiple barriers by designing two new competitive SPNS<br />
programs and conducting this systems integration assessment.<br />
Demographics and Epidemiology<br />
Population<br />
Understanding the needs and challenges facing people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong> requires<br />
some contextual information surrounding conditions and factors affecting life in <strong>Oregon</strong> as a whole.<br />
The total population <strong>of</strong> <strong>Oregon</strong> was 3,700,758 in 2006. The population <strong>of</strong> the balance <strong>of</strong> state—<br />
outside the Portland Eligible Metropolitan Area (EMA) that includes Clackamas, Columbia,<br />
Multnomah, Washington, and Yamhill Counties—was 1,986,964 in 2006, or 54 percent <strong>of</strong> <strong>Oregon</strong>’s<br />
2 Washington and <strong>Oregon</strong> each have two HOPWA formula grantees, including and EMSA and balance <strong>of</strong> state, and have similar<br />
general population and <strong>HIV</strong> demographics. At the request <strong>of</strong> the Steering Committee, we have provided comparison data for<br />
Washington state and city <strong>of</strong> Seattle throughout this section <strong>of</strong> the plan, to highlight the similarities and differences between these<br />
neighboring states.<br />
3 U.S. <strong>Housing</strong> and Urban Development. Available online: http://www.hud.gov/<strong>of</strong>fices/cpd/aidshousing/local/wa/index.cfm and<br />
http://www.hud.gov/<strong>of</strong>fices/cpd/about/budget/budget08/index.cfm (Accessed: February 7, 2008).<br />
4 U.S. <strong>Housing</strong> and Urban Development. Available online: http://www.hud.gov/<strong>of</strong>fices/cpd/aidshousing/index.cfm and<br />
http://www.hud.gov/local/ga/news/pr2007-10-10.cfm (Accessed: January 17, 2008).<br />
5 <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Program Design and Evaluation <strong>Services</strong>. <strong>Oregon</strong> <strong>Housing</strong> Opportunities in Partnership:<br />
Summary <strong>of</strong> Project Evaluation Design and Findings. Available online: http://www.oregon.gov/DHS/ph/hiv/services/housing.shtml<br />
(Accessed: November 30, 2007).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 5<br />
total population. 6 For comparison, neighboring Washington <strong>State</strong> (outside the Seattle EMA)<br />
included about 3.8 million people, or 60 percent <strong>of</strong> the state’s total population. 7<br />
Across the balance <strong>of</strong> the state <strong>of</strong> <strong>Oregon</strong>, population trends vary between areas <strong>of</strong> high growth and<br />
limited or negative population growth. Deschutes County, which grew the fastest between 1990 and<br />
2000, continues to lead <strong>Oregon</strong> counties in population growth. From 2000 to 2006, the population<br />
<strong>of</strong> Deschutes increased by 29 percent, fueled by the city <strong>of</strong> Bend, which grew by 35 percent.<br />
Neighboring Crook County grew by 20 percent. Other fast growing counties included Polk (17<br />
percent), Marion (9 percent), and Jackson Counties (9 percent).<br />
Ten counties in eastern <strong>Oregon</strong> have lost population since 2000, including Baker, Gilliam, Grant,<br />
Harney, Malheur, Sherman, Union, Wallowa, Wasco, and Wheeler Counties. These counties are<br />
largely rural and account for just three percent <strong>of</strong> <strong>Oregon</strong>’s total population.<br />
In 2006, the majority <strong>of</strong> the population (87 percent) <strong>of</strong> the state <strong>of</strong> <strong>Oregon</strong> was White. Asians were<br />
three percent <strong>of</strong> the population and two percent was Black/African American. In the balance <strong>of</strong><br />
state, 89 percent <strong>of</strong> the population was White, two percent was Asian, and less than one percent was<br />
Black/African American. Both statewide and in the balance <strong>of</strong> state, the 2006 population was 10<br />
percent Hispanic, regardless <strong>of</strong> race (meaning that a person could be counted as White as well as<br />
Hispanic, for example). 8<br />
6 U.S. Census. 2006 American Community Survey estimates. Available online: http://factfinder.census.gov/ (Accessed: November<br />
26, 2007).<br />
7 Washington <strong>State</strong> Office <strong>of</strong> Financial Management, Washington <strong>State</strong> Population Estimates. Available online:<br />
http://www.<strong>of</strong>m.wa.gov/pop/april1/default.asp (Accessed: January 10, 2008).<br />
8 U.S. Census. 2006 American Community Survey estimates. Available online: http://factfinder.census.gov/ (Accessed: November<br />
26, 2007).
6 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Epidemiology <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong><br />
As <strong>of</strong> March 31, 2007, there were 4,777 people reported living with <strong>HIV</strong>/<strong>AIDS</strong> in the state <strong>of</strong><br />
<strong>Oregon</strong>, including 1,291 in the balance <strong>of</strong> state, or 27 percent <strong>of</strong> the state total. 9 By comparison,<br />
with an overall population nearly twice as large, neighboring Washington reported 9,774 people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong> as <strong>of</strong> June 2000. In Washington, 30 percent <strong>of</strong> the people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> were diagnosed in the balance <strong>of</strong> state, a distribution similar to that between Portland<br />
and the balance <strong>of</strong> <strong>Oregon</strong>. 10<br />
These totals are based on data collected through <strong>HIV</strong>/<strong>AIDS</strong> surveillance data, and do not include<br />
people who do not know that they have <strong>HIV</strong>/<strong>AIDS</strong> nor people who are aware but have not been<br />
reported yet. <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong> (DHS) estimates that the actual prevalence <strong>of</strong><br />
<strong>HIV</strong>/<strong>AIDS</strong> is approximately 48 percent higher, 11 or about 7,077 people statewide and 1,911 in the<br />
balance <strong>of</strong> state.<br />
The <strong>AIDS</strong> case rate in <strong>Oregon</strong> was 34 th among states (excluding the District <strong>of</strong> Columbia) in 2005,<br />
at 6.0 per 100,000. The state <strong>of</strong> Washington, by comparison, ranked 28 th . 12<br />
People living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong> are dispersed throughout the balance <strong>of</strong> state. Nearly every<br />
county reported at least one person living with <strong>HIV</strong>/<strong>AIDS</strong> in 2007, with 21 counties reporting at<br />
least eight people, and 11 counties reporting at least 30 people. Marion, Lane, and Jackson<br />
Counties, the three largest in population in the balance <strong>of</strong> state, have the largest concentrations <strong>of</strong><br />
people living with <strong>HIV</strong>/<strong>AIDS</strong>. 13 More than 90 percent <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong> reside<br />
within 25 miles <strong>of</strong> I-5. 14<br />
Table 2 on the following page shows the population and number <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong><br />
by county in the balance <strong>of</strong> state.<br />
9 <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, <strong>HIV</strong> Data and Analysis. Available online:<br />
http://www.oregon.gov/DHS/ph/hiv/data/index.shtml (Accessed: November 26, 2007).<br />
10 Washington <strong>State</strong>/Seattle-King County <strong>HIV</strong>/<strong>AIDS</strong> Epidemiology Report, First Half 2007. Available online:<br />
http://www.metrokc.gov/health/apu/epi/1st-half-2007.pdf (Accessed: January 10, 2008).<br />
11 <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, <strong>HIV</strong> Care and Treatment Program, 2007 HOPWA NOFA Proposal for the <strong>Oregon</strong><br />
<strong>Housing</strong> and Behavioral Health Initiative (OHBHI).<br />
12 The <strong>AIDS</strong> case rate is calculated by dividing the number <strong>of</strong> <strong>AIDS</strong> cases reported during the 12 months <strong>of</strong> the most recent year for<br />
which data are available by the population in that same year, multiplied by 100,000. “<strong>HIV</strong>/<strong>AIDS</strong> Surveillance Report: Cases <strong>of</strong> <strong>HIV</strong><br />
Infection and <strong>AIDS</strong> in the United <strong>State</strong>s, 2005,” National Center for <strong>HIV</strong>, STD and TB Prevention, Centers for Disease Control and<br />
Prevention, Department <strong>of</strong> Health and Human <strong>Services</strong>, 2006. As cited on the Kaiser Family Foundation <strong>State</strong> Health Facts website.<br />
Available online: http://www.statehealthfacts.org/comparemaptable.jsp?ind=513&cat=11&yr=1&typ=1&sort=n&o=d (Accessed:<br />
January 15, 2008).<br />
13 <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, <strong>HIV</strong> Data and Analysis. Available online:<br />
http://www.oregon.gov/DHS/ph/hiv/data/index.shtml (Accessed: November 26, 2007).<br />
14 <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, <strong>HIV</strong> Care and Treatment Program, 2007 HOPWA NOFA Proposal for the <strong>Oregon</strong><br />
<strong>Housing</strong> and Behavioral Health Initiative (OHBHI).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 7<br />
Table 2:<br />
Total Population (2006) and Number <strong>of</strong> People Living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> (2007) for Counties in the <strong>Balance</strong> <strong>of</strong> <strong>State</strong><br />
County Population<br />
Number <strong>of</strong><br />
PLWHA<br />
Percentage<br />
<strong>of</strong> BoS Total<br />
Baker County 16,243 *
8 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
People living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong> have a broad diversity <strong>of</strong> backgrounds. Similar to<br />
neighboring Washington <strong>State</strong> and nationwide, people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong> include<br />
men and women <strong>of</strong> all ages. As treatments and medications for <strong>HIV</strong>/<strong>AIDS</strong> improve, people with<br />
<strong>HIV</strong>/<strong>AIDS</strong> are living longer, and in 2007, 30 percent <strong>of</strong> <strong>Oregon</strong>ians with <strong>HIV</strong>/<strong>AIDS</strong> were over 50<br />
years old. 15<br />
<strong>HIV</strong>/<strong>AIDS</strong> also impacts diverse households. People living with <strong>HIV</strong>/<strong>AIDS</strong> include single men and<br />
women, as well as adults living in households with children and other adults. In the balance <strong>of</strong> state,<br />
some regions serve a high percentage <strong>of</strong> adults living with their families, particularly in the Eugene<br />
area.<br />
The prevalence <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> is disproportionately high for Blacks/African Americans nationwide,<br />
and this trend holds true in <strong>Oregon</strong>. While Blacks/African Americans comprise less than two<br />
percent <strong>of</strong> the state population, they account for seven percent <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong>. In<br />
recent years, Blacks/African Americans have six times the rate <strong>of</strong> new diagnoses compared to<br />
Whites in <strong>Oregon</strong>, 16 which reflects the national statistic that Blacks/African Americans face the<br />
highest rates <strong>of</strong> new <strong>AIDS</strong> cases per capita (more than four times that <strong>of</strong> the general population, and<br />
more than 10 times that <strong>of</strong> Whites). 17<br />
Tables 3 and 4 on the following pages summarize demographics and risk factors for people living<br />
with <strong>HIV</strong>/<strong>AIDS</strong> in the state <strong>of</strong> <strong>Oregon</strong> as <strong>of</strong> March 31, 2007.<br />
15 <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, <strong>HIV</strong> Data and Analysis. Available online:<br />
http://www.oregon.gov/DHS/ph/hiv/data/index.shtml (Accessed: November 26, 2007).<br />
16 <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, <strong>HIV</strong> Data and Analysis, Epidemiological Pr<strong>of</strong>ile, 2005. Available online:<br />
http://www.oregon.gov/DHS/ph/hiv/data/EpiPr<strong>of</strong>ile.shtml (Accessed: November 27, 2007).<br />
17 2005 National Health Care Disparities Report, Centers for Disease Control and Prevention, 2005. Appendix D, Table 52: New<br />
<strong>AIDS</strong> cases per 100,000 population 13 and over: Race/Ethnicity. Available online:<br />
http://www.ahrq.gov/qual/nhdr05/quality/effectiveness/hiv/T52.htm (Accessed: June 20, 2008).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 9<br />
Demographics<br />
Race/Ethnicity<br />
White, not<br />
Hispanic<br />
Black/African<br />
American, not<br />
Hispanic<br />
Table 3:<br />
Demographics for <strong>State</strong> <strong>of</strong> <strong>Oregon</strong> (as <strong>of</strong> July 2006)<br />
and for People Living with <strong>HIV</strong> and <strong>AIDS</strong> in <strong>Oregon</strong> (as <strong>of</strong> March 2007)<br />
<strong>State</strong> <strong>of</strong><br />
OR<br />
People Living with<br />
<strong>HIV</strong><br />
People Living<br />
with <strong>AIDS</strong><br />
People Living with<br />
<strong>HIV</strong> and <strong>AIDS</strong><br />
Percent Number Percent Number Percent Number Percent<br />
81% 1,522 81% 2,320 80% 3,842 80%<br />
2% 139 7% 194 7% 333 7%<br />
Hispanic 10% 167 9% 304 10% 471 10%<br />
Asian/Pacific<br />
Islander<br />
American<br />
Indian/Alaska<br />
Native<br />
4% 15 1% 50 2% 65 1%<br />
1% 19 1% 33 1% 52 1%<br />
Multi-Race 2% * * * * * *<br />
Unknown 0% * * * * * *<br />
Gender<br />
Total 100% 1,872 100% 2,905 100% 4,777 100%<br />
Male 50% 1,587 85% 2,600 90% 4,187 88%<br />
Female 50% 285 15% 305 10% 590 12%<br />
Age<br />
Total 100% 1,872 100% 2,905 100% 4,777 100%<br />
Under 19 26% 34 2% 9
10 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Table 4:<br />
People Living with <strong>HIV</strong> and <strong>AIDS</strong> as <strong>of</strong> March 2007 in <strong>Oregon</strong> by Exposure Category<br />
Demographics<br />
Exposure Category<br />
Men who have Sex with<br />
Men (MSM)<br />
People Living with<br />
<strong>HIV</strong><br />
People Living with<br />
<strong>AIDS</strong><br />
People Living with<br />
<strong>HIV</strong> and <strong>AIDS</strong><br />
Number Percent Number Percent Number Percent<br />
1,168 62% 1,778 61% 2,946 62%<br />
Injection Drug Use (IDU) 176 9% 349 12% 525 11%<br />
MSM/IDU 144 8% 249 9% 403 8%<br />
Heterosexual 195 10% 283 10% 478 10%<br />
Other/Hemophilia/Blood<br />
Transfusion<br />
Pediatric – Mother with/at<br />
risk for <strong>HIV</strong><br />
10
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 11<br />
Homelessness Advisory Council (EHAC), the poverty rate in rural counties exceeded the rate in<br />
urban counties, and the unemployment rate was higher in rural (6.6 percent) than in urban counties<br />
(5.1 percent). 23<br />
Average incomes are also generally lower in rural counties than in urban areas. According to HUD,<br />
the Median Family Income (MFI) for <strong>Oregon</strong> was $55,700 in 2007. The MFI was $59,400 in<br />
metropolitan areas, and $45,600 in nonmetropolitan areas. MFI varied by county, from a low <strong>of</strong><br />
$39,000 in Wheeler County to $67,400 in Benton County. 24<br />
Many counties in rural <strong>Oregon</strong>, already struggling with low incomes and higher rates <strong>of</strong><br />
unemployment, are facing budgetary pressures that severely limit the funds available for local<br />
housing and services. The loss <strong>of</strong> federal timber replacement revenues in 2007—called O & C<br />
Revenues for federal land previously owned by <strong>Oregon</strong> and California Railroad—has caused<br />
financial crises in several counties. For example, more than two-thirds <strong>of</strong> the county general funds<br />
<strong>of</strong> Josephine and Douglas Counties relied on O & C Revenues. 25<br />
Health Insurance in <strong>Oregon</strong><br />
In 2006, a total <strong>of</strong> 576,000 <strong>Oregon</strong>ians lacked health insurance, about 16 percent <strong>of</strong> the state<br />
population, 26 compared to nine percent for neighboring Washington. 27 Stakeholders across the state<br />
cited the restricted eligibility for the <strong>Oregon</strong> Health Plan (OHP), the state health insurance program,<br />
and the lack <strong>of</strong> funding options to serve people who don’t qualify, as a major impediment to<br />
providing adequate medical care and supportive services (including supportive housing) to lowincome<br />
<strong>Oregon</strong> residents.<br />
During the 1990s, OHP received national praise for its expansion <strong>of</strong> health insurance coverage<br />
among state residents, achieved by creating a two-tiered benefits structure. OHP Plus provided a<br />
full range <strong>of</strong> services to people who would be categorically eligible for Medicaid, such as lowincome<br />
families and pregnant women. OHP Standard extended a limited benefits option to people<br />
who were below the federal poverty line.<br />
In 2002, OHP Standard attempted a further expansion to residents at 185 percent <strong>of</strong> poverty or less,<br />
predicated on cost-sharing and premium policies. The expansion failed, as <strong>Oregon</strong>’s budget crisis<br />
facilitated a severe, ongoing drop in enrollment. 28 The <strong>Oregon</strong> Health Plan Standard program was<br />
forced to take measures which reduced enrollment from 104,000 people in January 2003 to 49,000<br />
in December 2003, and to less than 25,000 in January 2007. 29 DHS recently announced that it will<br />
23<br />
Ending Homelessness Advisory Council (EHAC). Draft 10 Year Plan to End Homelessness, Part 1: Understanding Homelessness<br />
in <strong>Oregon</strong>. Available online: http://www.ehac.oregon.gov (Accessed: November 27, 2007).<br />
24<br />
U.S. <strong>Housing</strong> and Urban Development, Income Limits FY 2007. Available online: http://www.huduser.org/datasets/il.html<br />
(Accessed: November 27, 2007).<br />
25<br />
Dennis Richardson, <strong>Oregon</strong> <strong>State</strong> Representative. March 2007 Newsletter. Available online:<br />
http://www.dennisrichardson.org/lu031607.htm (Accessed: November 29, 2007).<br />
26<br />
<strong>Oregon</strong> Progress Board, Benchmarks Reports. Available online: http://benchmarks.oregon.gov (Accessed: October 15, 2007).<br />
27<br />
Washington <strong>State</strong> Office <strong>of</strong> Financial Management, 2006 Washington <strong>State</strong> Population Survey. Available online:<br />
http://www.<strong>of</strong>m.wa.gov/researchbriefs/brief039.pdf (Accessed: January 10, 2008).<br />
28<br />
Oberlander, Jonathan. “Health Reform Interrupted: The Unraveling Of The <strong>Oregon</strong> Health Plan,” in Health Affairs, December<br />
2006. Available online: http://content.healthaffairs.org/cgi/content/short/hlthaff.26.1.w96v1 (Accessed: November 27, 2007).<br />
29<br />
Ending Homelessness Advisory Council (EHAC). Draft 10 Year Plan to End Homelessness, Part 1: Understanding Homelessness<br />
in <strong>Oregon</strong>. Available online: http://www.ehac.oregon.gov (Accessed: November 27, 2007).
12 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
reopen enrollment for OHP Standard through a lottery beginning in January 2008, although the total<br />
enrollment in OHP Standard will maintain a biennial average <strong>of</strong> 24,000. 30<br />
The <strong>Oregon</strong> <strong>HIV</strong> Care and Treatment Program helps to bridge the insurance gap for people living<br />
with <strong>HIV</strong> in <strong>Oregon</strong> who seek care, using a unique set <strong>of</strong> tools. <strong>Oregon</strong> <strong>HIV</strong> Care and Treatment<br />
uses federal Ryan White formula funding to pay health insurance premiums and co-pays for any<br />
presenting income-eligible clients who are not insured through OHP. The program leverages the<br />
<strong>Oregon</strong> Medical Insurance Pool (OMIP) to provide coverage for <strong>Oregon</strong> residents with qualifying<br />
medical conditions—including <strong>HIV</strong>/<strong>AIDS</strong>—that would otherwise restrict their individual health<br />
insurance coverage through private insurers. 31<br />
With the enactment <strong>of</strong> <strong>Oregon</strong>’s mental health parity law in January 2007, all group health insurers<br />
must cover insured individuals for a broad range <strong>of</strong> behavioral health services, including mental<br />
health and substance abuse treatment, at levels equal to coverage for other medical conditions. 32<br />
This change may improve the availability <strong>of</strong> needed care for <strong>Oregon</strong>ians with <strong>HIV</strong>/<strong>AIDS</strong> and cooccurring<br />
disorders, although the health insurance context described above continues to pose<br />
system-wide challenges.<br />
<strong>Housing</strong> in <strong>Oregon</strong><br />
<strong>Housing</strong> affordability is declining rapidly in <strong>Oregon</strong> for both renters and owners. The 2006-2010<br />
<strong>State</strong> <strong>of</strong> <strong>Oregon</strong> Consolidated Plan reported that 73 percent <strong>of</strong> very low-income households, 60<br />
percent <strong>of</strong> low-income households, and 37 percent <strong>of</strong> moderate-income households in <strong>Oregon</strong> are<br />
cost-burdened. 33 Households are considered cost-burdened if they spend more than 30 percent <strong>of</strong><br />
income on housing and utilities. The <strong>State</strong> <strong>of</strong> Washington Consolidated Plan reported similar<br />
findings: 70 percent <strong>of</strong> very low-income households and 60 percent <strong>of</strong> low-income households were<br />
cost-burdened. 34<br />
Affordable housing is particularly scarce for renters. In 2006, 82 percent <strong>of</strong> <strong>Oregon</strong> households<br />
below the rental median income ($22,669 in 2006) were considered cost-burdened. Forty-six<br />
percent <strong>of</strong> homeowners with incomes below the median for homeowners ($56,164) were costburdened.<br />
35<br />
The state <strong>of</strong> <strong>Oregon</strong> has a relatively low rate <strong>of</strong> homeownership, 64 percent compared to the<br />
national rate <strong>of</strong> 67 percent in 2006. The rate <strong>of</strong> homeownership is higher in the balance <strong>of</strong> state (66<br />
percent) than in the Portland Eligible Metropolitan Area (63 percent).<br />
Homeownership rates in <strong>Oregon</strong> vary substantially by county. The low homeownership rates <strong>of</strong><br />
Benton (55 percent) and Lane Counties (61 percent) are likely influenced by their large college<br />
30<br />
<strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>. “Several thousand <strong>Oregon</strong>ians to be added to <strong>Oregon</strong> Health Plan's Standard benefit<br />
package” (news release), January 7, 2008. Available online: http://www.oregon.gov/DHS/news/2008news/2008-0107.shtml<br />
(Accessed: January 14, 2008).<br />
31<br />
<strong>Oregon</strong> Medical Insurance Pool. Available online: http://www.omip.state.or.us/ (Accessed: November 29, 2007).<br />
32<br />
<strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, <strong>HIV</strong> Care and Treatment Program, 2007 HOPWA NOFA Proposal for the <strong>Oregon</strong><br />
<strong>Housing</strong> and Behavioral Health Initiative (OHBHI).<br />
33<br />
<strong>Oregon</strong> <strong>Housing</strong> and Community <strong>Services</strong>. <strong>State</strong> <strong>of</strong> <strong>Oregon</strong> Consolidated Plan, 2006-2010. Available online:<br />
http://www.oregon.gov/OHCS/HRS_Consolidated_Plan_5yearplan.shtml (Accessed: November 27, 2007).<br />
34<br />
Washington <strong>State</strong> Department <strong>of</strong> Community, Trade and Economic Development <strong>Housing</strong> Division, 2005-2009 Consolidated Plan.<br />
Available online http://cted.wa.gov/site/811/default.aspx (Accessed: January 10, 2008).<br />
35<br />
<strong>Oregon</strong> Progress Board, Benchmarks Reports. Available online: http://benchmarks.oregon.gov (Accessed: October 15, 2007).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 13<br />
campuses. Rental housing is less available in counties with higher homeownership rates, such as<br />
Polk (74 percent), Josephine (72 percent), and Deschutes (70 percent). 36<br />
Amid a national trend toward increasing mortgage default rates, <strong>Oregon</strong> compares favorably to<br />
other states, but is in line with the neighboring state <strong>of</strong> Washington. In 2007, 0.54 percent and 0.57<br />
percent <strong>of</strong> households in <strong>Oregon</strong> and Washington, respectively, entered some stage <strong>of</strong> foreclosure,<br />
compared with 1.03 percent nationwide. 37<br />
Each year, the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development (HUD) establishes Fair Market<br />
Rents (FMRs) to determine payment standards for the Section 8 <strong>Housing</strong> Choice Voucher program,<br />
as well as other HUD programs such as HOME rental assistance. HUD defines FMRs as the 40th<br />
percentile rent, or, the dollar amount below which 40 percent <strong>of</strong> the standard-quality rental housing<br />
units are rented. 38 FMRs are a good indicator <strong>of</strong> the variance in housing costs across counties.<br />
In the balance <strong>of</strong> state, the FMRs for most counties increased by about eight percent from 2006 to<br />
2008. For 2008, Baker County has the lowest FMR ($450) and Deschutes County has the highest<br />
FMR ($614) in the balance <strong>of</strong> state. 39<br />
Table 5 on the following page lists the FMR for one-bedroom apartment rentals in the balance <strong>of</strong><br />
state, by county for the years 2006 through 2008.<br />
36 U.S. Census, 2006 American Community Survey estimates. Available online: http://factfinder.census.gov/ (Accessed: November<br />
27, 2007).<br />
37 Data from RealtyTrac, a private firm that tracks nationwide foreclosure trends. Available online:<br />
http://www.realtytrac.com/ContentManagement/pressrelease.aspx?ChannelID=9&ItemID=3988&accnt=64847 (Accessed: February<br />
19, 2008).<br />
38 U.S. <strong>Housing</strong> and Urban Development, Fair Market Rents. Available online<br />
http://www.huduser.org/datasets/fmr/fmrover_071707R2.doc (Accessed: December 3, 2007).<br />
39 U.S. <strong>Housing</strong> and Urban Development, Fair Market Rents. Available online: http://www.huduser.org/datasets/fmr.html (Accessed:<br />
November 26, 2007).
14 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Table 5:<br />
2006-2008 Fair Market Rents for One-Bedroom Unit for <strong>Oregon</strong><br />
Counties in <strong>Balance</strong> <strong>of</strong> <strong>State</strong><br />
County<br />
2006 FMR<br />
for 1 BR<br />
2007 FMR<br />
for 1 BR<br />
2008 FMR<br />
for 1 BR<br />
Baker $415 $430 $450<br />
Benton (Corvallis MSA) $560 $579 $601<br />
Clatsop $503 $521 $544<br />
Coos $471 $488 $512<br />
Crook $494 $512 $535<br />
Curry $505 $523 $548<br />
Deschutes (Bend MSA) $567 $587 $614<br />
Douglas $453 $468 $491<br />
Gilliam $483 $499 $524<br />
Grant $483 $499 $524<br />
Harney $429 $444 $466<br />
Hood River $514 $532 $556<br />
Jackson (Medford MSA) $540 $560 $581<br />
Jefferson $490 $507 $530<br />
Josephine $510 $528 $552<br />
Klamath $431 $446 $467<br />
Lake $429 $444 $466<br />
Lane (Eugene-Springfield MSA) $561 $581 $600<br />
Lincoln $525 $543 $567<br />
Linn $532 $550 $576<br />
Malheur $445 $461 $484<br />
Marion (Salem MSA) $520 $530 $531<br />
Morrow $483 $499 $524<br />
Polk (Salem MSA) $520 $530 $531<br />
Sherman $483 $499 $524<br />
Tillamook $506 $524 $550<br />
Umatilla $438 $453 $475<br />
Union $427 $442 $462<br />
Wallowa $424 $439 $459<br />
Wasco $475 $492 $516<br />
Wheeler $483 $499 $524<br />
Source: U.S. <strong>Housing</strong> and Urban Development, Fair Market Rents. Available online:<br />
http://www.huduser.org/datasets/fmr.html (Accessed: November 26, 2007).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 15<br />
Homelessness<br />
<strong>Oregon</strong> has one <strong>of</strong> the highest rates <strong>of</strong> homelessness per capita in the nation. <strong>Oregon</strong> <strong>Housing</strong> and<br />
Community <strong>Services</strong> (OHCS) reported that the number <strong>of</strong> <strong>Oregon</strong>ians who were homeless on any<br />
given night increased from 21 per 10,000 residents in 2002, to 31 per 10,000 in 2006. 40 A recent<br />
report estimated the 2007 homeless rate to be 45 per 10,000. 41 In 2006, the state <strong>of</strong> Washington<br />
estimated that 31 per 10,000 residents were homeless on any given night. 42<br />
The worsening statewide situation contrasts with the nationally recognized successes <strong>of</strong> the Portland<br />
10 Year Plan to End Homelessness, enacted in December 2004. During the first two years <strong>of</strong> the<br />
plan’s implementation, 1,039 chronically homeless individuals and 770 homeless families with<br />
children were housed, numbers far above the performance goals initially laid out in the plan. 43<br />
The 2007 <strong>Oregon</strong> one-night shelter count identified 13,020 total homeless people, including 4,655<br />
people who were turned away from shelters. These numbers are point-in-time counts <strong>of</strong> people who<br />
spent the night at a shelter or were turned away on one night in January 2007. One-night counts<br />
typically undercount homeless people in rural areas where shelter facilities are limited.<br />
Some counties in particular lack the facilities to serve homeless people seeking shelter. In 2007,<br />
Deschutes County reported 1,403 homeless people, including 1,179 who were turned away from<br />
shelters. The vast majority <strong>of</strong> those turned away were people in families with children. 44<br />
Most shelters and one-night counts do not keep data on the number <strong>of</strong> homeless people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong>, although homeless people are known to have added risk <strong>of</strong> <strong>HIV</strong> diagnosis. The U.S.<br />
homeless population has an estimated median rate <strong>of</strong> <strong>HIV</strong> prevalence <strong>of</strong> at least three times<br />
higher—three percent versus one percent—than the general population. 45 The 2005 needs<br />
assessment for people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong> echoed the national findings on<br />
homelessness. Twenty-six percent <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong> reported being in unstable<br />
housing situations in the past year, and 15 percent had been homeless in the past two years. 46<br />
Homelessness is especially dangerous for people living with <strong>HIV</strong>/<strong>AIDS</strong>. Effective treatment <strong>of</strong><br />
<strong>HIV</strong>/<strong>AIDS</strong> requires a regular regimen <strong>of</strong> antiretroviral medications, which may be difficult to<br />
administer under conditions <strong>of</strong> homelessness or in emergency shelters. Many people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> may also be more susceptible to life-threatening infections if living on the street or in<br />
unsanitary conditions.<br />
40 <strong>Oregon</strong> Progress Board, Benchmarks Reports. Available online: http://benchmarks.oregon.gov (Accessed: October 15, 2007).<br />
41 Ending Homelessness Advisory Council (EHAC). Draft 10 Year Plan to End Homelessness, Part 1: Understanding Homelessness<br />
in <strong>Oregon</strong>. Available online: http://www.ehac.oregon.gov (Accessed: November 27, 2007).<br />
42 Washington <strong>State</strong> Department <strong>of</strong> Community, Trade and Economic Development <strong>Housing</strong> Division, 2006 Ten Year Plan to End<br />
Homelessness. Available online: http://cted.wa.gov/_CTED/documents/ID_3356_Publications.doc (Accessed: January 10, 2008).<br />
43 City <strong>of</strong> Portland, Bureau <strong>of</strong> <strong>Housing</strong> and Community Development. 2006 Annual Report for the 10 Year Plan to End<br />
Homelessness. Available online: http://www.portlandonline.com/bhcd/index.cfm?c=38062 (Accessed: November 29, 2007).<br />
44 Ending Homelessness Advisory Council (EHAC). Draft 10 Year Plan to End Homelessness, Part 1: Understanding Homelessness<br />
in <strong>Oregon</strong>. Available online: http://www.ehac.oregon.gov (Accessed: November 27, 2007).<br />
45 Higher rates (8.5 to 62 percent) have been found in selected homeless sub-populations. Song, John M.D., M.P.H., M.A.T.,<br />
<strong>HIV</strong>/<strong>AIDS</strong> & Homelessness: Recommendations for Clinical Practice and Public Policy, November 1999, National Health Care for<br />
the Homeless Council, Health Care for the Homeless Clinician’s Network, p. 1. Available online: www.nhchc.org (Accessed:<br />
January 10, 2002).<br />
46 <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Program Design and Evaluation <strong>Services</strong>. We Listened…2005: Survey for People Living<br />
with <strong>HIV</strong> and <strong>AIDS</strong> in <strong>Oregon</strong>. Available online: http://www.oregon.gov/DHS/ph/hiv/services/needs/reports.shtml (Accessed:<br />
November 27, 2007).
16 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Stable housing enables people living with <strong>HIV</strong>/<strong>AIDS</strong> to access and maintain life-saving medical<br />
care and treatments. Compared to those who were in stable housing, homeless people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> experience worse overall physical and mental health, are more likely to be hospitalized<br />
and use emergency rooms, and are less likely to receive medical treatment. Stable housing is<br />
significantly correlated with treatment success. 47<br />
In addition, research indicates housing stability decreases the risk factors that can lead to <strong>HIV</strong><br />
transmission. A 2006 study found that each prevented <strong>HIV</strong> infection saves $303,000 in lifetime<br />
medical costs. 48 Compared to the modest cost <strong>of</strong> providing housing for people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong>, the cost savings from preventing <strong>HIV</strong> transmission are substantial.<br />
In a study released in 2007, researchers compared the costs <strong>of</strong> providing rental assistance, case<br />
management, and related services to the treatment costs associated with new cases <strong>of</strong> <strong>HIV</strong>. The<br />
study found that if just one out <strong>of</strong> every 19 clients receiving housing support avoided <strong>HIV</strong><br />
transmission, the intervention would be cost-saving. The housing intervention would be costeffective<br />
if it prevented one <strong>HIV</strong> transmission for every 64 clients. 49<br />
<strong>Housing</strong> Needs for People Living with <strong>HIV</strong>/<strong>AIDS</strong><br />
<strong>Housing</strong> assistance is an important need for people living with <strong>HIV</strong>/<strong>AIDS</strong> who face a spectrum <strong>of</strong><br />
housing instability, including those who are not currently homeless. Recent research emphasizes<br />
that housing needs, including but not limited to homelessness, are significant barriers to appropriate,<br />
effective <strong>HIV</strong> medical care, and that housing assistance increases access and retention in medical<br />
care and treatment. 50<br />
The most recent needs assessment for people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong> found that forty<br />
percent <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong> reported a need for housing assistance (including both<br />
those who needed and were receiving assistance, and those who needed but were not receiving<br />
assistance), including more than 500 people in the balance <strong>of</strong> state. Sixteen percent <strong>of</strong> needs<br />
assessment survey respondents reported receiving assistance through a Section 8 voucher or public<br />
housing, or an estimated 200 clients in the balance <strong>of</strong> state. A small number <strong>of</strong> respondents<br />
indicated receiving assistance through transitional housing programs or Shelter Plus Care. The<br />
<strong>Oregon</strong> <strong>Housing</strong> Opportunities in Partnership (OHOP) Program serves approximately 100 people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong> in the balance <strong>of</strong> state each year. 51<br />
47<br />
National <strong>AIDS</strong> <strong>Housing</strong> Coalition. <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong>: Improving Health Outcomes. Available online:<br />
http://www.nationalaidshousing.org/toolkit/health_outcomes.pdf (Accessed: December 7, 2007).<br />
48<br />
Schackman, et al, “The Lifetime Cost <strong>of</strong> Current Human Immunodeficiency Virus Care in the United<br />
<strong>State</strong>s”, Medical Care, Vol. 44, No. 11, p. 990, November 2006.<br />
49<br />
Holtgrave, David R., et al. “Cost and Threshold Analysis <strong>of</strong> housing as an <strong>HIV</strong> Prevention Intervention,” in the November 2007<br />
<strong>Housing</strong> and <strong>HIV</strong>/<strong>AIDS</strong> Supplement to <strong>AIDS</strong> and Behavior.<br />
50<br />
Aidala, A., et al. “<strong>Housing</strong> Need, housing Assistance, and Connection to <strong>HIV</strong> Medical Care,” in the November 2007 <strong>Housing</strong> and<br />
<strong>HIV</strong>/<strong>AIDS</strong> Supplement to <strong>AIDS</strong> and Behavior.<br />
51<br />
<strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Program Design and Evaluation <strong>Services</strong>. We Listened…2005: Survey for People Living<br />
with <strong>HIV</strong> and <strong>AIDS</strong> in <strong>Oregon</strong>. Available online: http://www.oregon.gov/DHS/ph/hiv/services/needs/reports.shtml (Accessed:<br />
November 27, 2007).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 17<br />
Integration <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Services</strong> and <strong>Housing</strong> with<br />
Existing <strong>Systems</strong><br />
This section describes how <strong>HIV</strong>/<strong>AIDS</strong> services and housing are currently integrated into other<br />
systems in the balance <strong>of</strong> state and identifies opportunities that exist for further integration with<br />
existing or potential partners.<br />
Meaningful integration with mainstream housing and service providers and the general public is<br />
critical for <strong>Oregon</strong> <strong>Housing</strong> Opportunities in Partnership (OHOP) and other programs and agencies<br />
that serve people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong>. Connections to local service providers and<br />
housing agencies help ensure that OHOP resources are reaching all <strong>of</strong> the diverse communities <strong>of</strong><br />
eligible clients in need, and assure that the needs <strong>of</strong> people with multiple, co-occurring challenges<br />
are recognized and efficiently addressed. In addition, partnership with mainstream housing<br />
organizations (such as affordable housing developers or housing authorities) and participation in<br />
planning processes (such as the Continuum <strong>of</strong> Care or Consolidated Funding Cycle processes) can<br />
lead to the development or dedication <strong>of</strong> new housing resources, targeted either for people with<br />
disabilities in general or specifically for people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
The first part <strong>of</strong> this chapter presents information on general outreach strategies that OHOP and its<br />
partners use or could use to communicate with an array <strong>of</strong> different systems, as well as outlines<br />
some barriers to transparent and effective communication. The second part <strong>of</strong> the chapter provides<br />
context information on some <strong>of</strong> the most relevant systems, including key components <strong>of</strong> the<br />
particular system, the level <strong>of</strong> integration that exists with <strong>HIV</strong>/<strong>AIDS</strong> housing and services, and<br />
challenges within that system. This “map” <strong>of</strong> interlocking systems is intended to help OHOP and its<br />
partners better understand how to employ dedicated <strong>HIV</strong>/<strong>AIDS</strong> resources to complement existing<br />
capacity in these regions, and how to most effectively collaborate with the broader set <strong>of</strong> affordable<br />
housing and services systems to increase and maintain capacity to serve as many <strong>Oregon</strong>ians as<br />
possible. (Critical issues within this context, and specific recommendations for addressing<br />
challenges and meeting need among people living with <strong>HIV</strong>/<strong>AIDS</strong>, are addressed in the subsequent<br />
section (Section 2), beginning on page 40 <strong>of</strong> this plan.)<br />
Information for these sections comes from primary research, interviews with key informants across<br />
the state, and a survey <strong>of</strong> stakeholders. The stakeholders that participated in the survey were divided<br />
between the four OHOP service regions. Half <strong>of</strong> the respondents represent <strong>HIV</strong>/<strong>AIDS</strong> agencies, and<br />
half represent agencies that do not specifically provide services to people with <strong>HIV</strong>/<strong>AIDS</strong>, although<br />
some <strong>of</strong> their clients may have an <strong>HIV</strong> diagnosis. Detailed survey responses are also available in<br />
Appendix 2.<br />
Outreach Strategies<br />
Outreach to a broad spectrum <strong>of</strong> housing and service system stakeholders and others must be the<br />
cornerstone <strong>of</strong> any integration effort. Because the number <strong>of</strong> <strong>Oregon</strong> residents living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> outside <strong>of</strong> the Portland metro area is relatively small and spread out, OHOP and partner<br />
staff must take a proactive role simply to make known the needs <strong>of</strong> this population and the
18 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
resources they have to <strong>of</strong>fer. Yet staff capacity is a serious challenge for dedicated <strong>HIV</strong>/<strong>AIDS</strong><br />
programs and agencies, as staff have limited time to dedicate to outreach activities. When they do<br />
reach out, they may be met with misconceptions or stigma about their clients, or limited willingness<br />
on the part <strong>of</strong> other agencies to engage people perceived to have “their own” resources.<br />
Client confidentiality concerns can also restrict the ways that OHOP and other <strong>HIV</strong>/<strong>AIDS</strong> providers<br />
publicize their activities and resources. For people living with <strong>HIV</strong>/<strong>AIDS</strong>, stigma and<br />
discrimination are factors in finding and maintaining housing, accessing support services, and<br />
seeking medical care. People living with <strong>HIV</strong>/<strong>AIDS</strong> <strong>of</strong>ten struggle to keep their <strong>HIV</strong> status private,<br />
particularly from landlords and neighbors. For this reason, OHOP tends to market its services<br />
quietly and to avoid disclosing to landlords and other providers that HOPWA is the source <strong>of</strong><br />
housing assistance for clients they place, or that clients qualify for assistance via an <strong>HIV</strong> diagnosis.<br />
This challenge has surfaced acutely in Jackson County, where people living with <strong>HIV</strong>/<strong>AIDS</strong> have<br />
been evicted from affordable housing programs, including one dedicated to pregnant women, when<br />
their <strong>HIV</strong> status was revealed.<br />
Partnerships with organizations that serve people with disabilities in general can help to alleviate<br />
confidentiality issues, by providing more general cover for making resources available to people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong>. For example, the Eastern <strong>Oregon</strong> Center for Independent Living (EOCIL)<br />
provides <strong>HIV</strong> case management and services in ten counties in eastern <strong>Oregon</strong> (OHOP Region 4).<br />
Because EOCIL serves individuals with multiple disabilities, its case managers can work with<br />
landlords and other partners without having to reveal the <strong>HIV</strong> status <strong>of</strong> their clients.<br />
Making general materials and information about OHOP services available routinely through<br />
mainstream providers is another way to raise awareness without disclosing clients’ <strong>HIV</strong>/<strong>AIDS</strong><br />
status. In key stakeholder interviews, providers in Eugene and Medford noted the need for simple<br />
marketing tools (such as updated brochures about OHOP, with contact names and phone numbers<br />
that clients can call) that could be disseminated by all types <strong>of</strong> service agencies as part <strong>of</strong> their<br />
general information packets. Another need noted by stakeholders in Jackson County was for<br />
<strong>HIV</strong>/<strong>AIDS</strong> training for mainstream services or housing provider staff.<br />
Some OHOP resources for people living with <strong>HIV</strong>/<strong>AIDS</strong> overlap with programs available to a<br />
wider client base. In Jackson County, for example, ACCESS has a limited pool <strong>of</strong> utility assistance<br />
to distribute among low-income clients, which include some people living with <strong>HIV</strong>/<strong>AIDS</strong> who<br />
could qualify for a greater level <strong>of</strong> utility assistance through OHOP. One solution to optimize the<br />
allocation <strong>of</strong> limited resources may be to include OHOP information on the ACCESS application<br />
form.<br />
In some cases, activities undertaken by the clients themselves can strengthen community<br />
relationships. An example <strong>of</strong> an effective tool for strengthening landlord connections in particular<br />
can be found in Lane County. St. Vincent de Paul <strong>of</strong>fers the Second Chance Renters Program to<br />
individuals who want to demonstrate commitment to good relationships with potential landlords, by<br />
learning both concrete information about tenant responsibilities and landlord expectations, as well<br />
as how to demonstrate consistency, trust, and a desire to succeed.<br />
Outreach can be especially difficult in rural areas which may have relatively few social service<br />
agencies and networks. Rural outreach may require creative partners to leverage limited housing<br />
resources. Faith-based organizations can provide community structure, are frequently mission-
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 19<br />
driven to assist people with limited assets, and may be willing to provide support, services, or even<br />
housing. Another opportunity may be the six USDA Rural Development <strong>of</strong>fices in the balance <strong>of</strong><br />
state, which provide rental assistance to low-income residents in rural areas. However, nationally<br />
this assistance has been greatly reduced in recent years, and these <strong>of</strong>fices in <strong>Oregon</strong> currently assist<br />
with only 700 rental units statewide.<br />
Health Care (including <strong>HIV</strong> Care)<br />
People living with <strong>HIV</strong>/<strong>AIDS</strong> have a range <strong>of</strong> health care needs, including treatment for <strong>HIV</strong><br />
disease itself, treatment for other chronic health conditions, supportive services, and in some cases<br />
care in an assisted living environment. In <strong>Oregon</strong>, the primary responsibility for meeting the health<br />
care needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong> falls to the <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>,<br />
Public Health, <strong>HIV</strong>/STD/TB Section, <strong>HIV</strong> Care and Treatment Program, known in brief as “<strong>HIV</strong><br />
Care and Treatment.” <strong>HIV</strong> Care and Treatment is also the administrator <strong>of</strong> the OHOP program. At<br />
least in part because <strong>of</strong> this structural connection, as well as because all recipients <strong>of</strong> <strong>HIV</strong> housing<br />
assistance are eligible for some health services as a result <strong>of</strong> their <strong>HIV</strong> diagnosis, integration<br />
between these two systems (health care and <strong>HIV</strong>/<strong>AIDS</strong> housing) is particularly extensive and well<br />
developed.<br />
<strong>HIV</strong> Care and Treatment administers <strong>HIV</strong> case management services throughout the <strong>Oregon</strong><br />
balance <strong>of</strong> state and provides an array <strong>of</strong> other types <strong>of</strong> statewide medical assistance, with a<br />
program-wide budget <strong>of</strong> approximately $14 million that includes both federal Ryan White<br />
Comprehensive <strong>AIDS</strong> Resources Emergency (CARE) Act funds and state general and other funds.<br />
Federal Ryan White CARE Act funds are awarded to all states by formula to provide primary<br />
healthcare and support services, including <strong>AIDS</strong> Drug Assistance Programs (ADAPs), which<br />
enhance access to care for people living with <strong>HIV</strong>/<strong>AIDS</strong> and their families. <strong>HIV</strong> Care and<br />
Treatment activities are therefore commonly referred to as “Ryan White” services, although state<br />
and other program funding for <strong>HIV</strong> Care and Treatment roughly equal the federal funding share.<br />
<strong>HIV</strong> Care and Treatment program services are provided in the balance <strong>of</strong> state by a network <strong>of</strong> 19<br />
<strong>AIDS</strong> service providers (15 county health departments, two community-based organizations, and<br />
two independent contractors) with a total <strong>of</strong> 42 <strong>HIV</strong> case managers serving more than 800 people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong> and their families each year. 52 Approximately $1.5 million <strong>of</strong> services are<br />
annually targeted to individuals in the balance <strong>of</strong> state, along with $2.5 to 3 million in ADAP<br />
funding. <strong>Oregon</strong>’s ADAP, known locally as CAREAssist, represents the <strong>HIV</strong> Care and Treatment<br />
Program’s largest program element by expenditure, and roughly 75 percent <strong>of</strong> ADAP funds are<br />
expended in the Portland metropolitan area.<br />
As part <strong>of</strong> its CAREAssist portfolio, <strong>Oregon</strong> <strong>HIV</strong> Care and Treatment is able to provide access to<br />
health insurance (as described in the section on Health Insurance above) for low-income people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong> who are not covered by the <strong>Oregon</strong> Health Plan (OHP). Between<br />
these two programs, any income-eligible <strong>Oregon</strong>ian living with <strong>HIV</strong>/<strong>AIDS</strong> who presents with a<br />
need for health insurance coverage can receive it. <strong>HIV</strong> Care and Treatment administrators estimate<br />
that approximately 20 percent <strong>of</strong> <strong>Oregon</strong>ians living with <strong>HIV</strong>/<strong>AIDS</strong> receive medical service<br />
52 <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, <strong>HIV</strong> Care and Treatment Program, 2007 HOPWA NOFA Proposal for the <strong>Oregon</strong><br />
<strong>Housing</strong> and Behavioral Health Initiative (OHBHI).
20 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
coverage through OHP, but approximately twice that number receive access to medical care through<br />
CAREAssist. 53<br />
OHOP <strong>Housing</strong> Coordinators work closely with <strong>HIV</strong> Case Managers throughout the state. The<br />
close coordination between programs allows OHOP to leverage nearly two dollars <strong>of</strong> other <strong>HIV</strong><br />
Care and Treatment program-funded services for every one dollar <strong>of</strong> HOPWA assistance. It is<br />
important to note that, prior to the introduction <strong>of</strong> the OHOP program, much <strong>of</strong> <strong>Oregon</strong>’s locally<br />
administered <strong>HIV</strong> case management support service funds were spent on housing. Since the<br />
inception <strong>of</strong> the OHOP program, the annual utilization <strong>of</strong> <strong>Oregon</strong> <strong>HIV</strong> case management local<br />
support service dollars for housing services has decreased by more than 50 percent; those funds are<br />
now able to be applied to other essential activities, including health care, oral health services,<br />
medical transportation, and addictions and mental health treatment.<br />
At the planning level, OHOP and <strong>HIV</strong> Care and Treatment administrators collaborate regularly,<br />
including in the development <strong>of</strong> the Ryan White Title II <strong>HIV</strong> Client <strong>Services</strong> Comprehensive Plan<br />
for 2006-2009. Over 70 percent <strong>of</strong> surveyed <strong>AIDS</strong> agencies reported participating in the Ryan<br />
White planning process, including the <strong>Oregon</strong> <strong>HIV</strong> Care Coalition.<br />
People living with <strong>HIV</strong>/<strong>AIDS</strong>, like others throughout <strong>Oregon</strong>, frequently turn to hospitals for their<br />
acute care needs, which can sometimes disrupt their housing stability. The <strong>Oregon</strong> Association <strong>of</strong><br />
Hospitals and Health <strong>Systems</strong> represents the interests <strong>of</strong> hospitals and other facilities across the<br />
state, highlighting key issues for members. 54 A key hospital issue <strong>of</strong> uncompensated care expenses<br />
may be limited in the case <strong>of</strong> people with <strong>HIV</strong>/<strong>AIDS</strong>, because <strong>of</strong> the health insurance assistance that<br />
<strong>HIV</strong> Care and Treatment provides (as described above). However, attention is required to ensure<br />
coordination between the two systems around transitions between inpatient and outpatient care and<br />
treatment for chronic conditions such as diabetes.<br />
Research has not yet measured the incidence, age <strong>of</strong> onset and cause <strong>of</strong> geriatric diseases in longterm<br />
survivors <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong>. 55 But Steering Committee members observed that these types <strong>of</strong><br />
major medical challenges are common among the growing numbers <strong>of</strong> clients they serve who have<br />
been living with the disease for some time. An <strong>HIV</strong>/<strong>AIDS</strong> housing provider in Portland reported<br />
serving an estimated 10 percent <strong>of</strong> clients in assisted living situations; while OHOP has served very<br />
few clients in such situations, the number in need <strong>of</strong> such assistance may increase.<br />
Mainstream assisted living facilities are not typically equipped to provide specialized <strong>HIV</strong> care, and<br />
may resist or encounter challenges in integrating people living with <strong>HIV</strong>/<strong>AIDS</strong> with dissimilar<br />
populations <strong>of</strong> older individuals or other specialized groups, such as people with developmental<br />
disabilities. <strong>State</strong> funding for clients in assisted living facilities is limited for virtually all<br />
populations, not just people living with <strong>HIV</strong>/<strong>AIDS</strong>, and strict admissions criteria can delay clients<br />
entering care.<br />
The network <strong>of</strong> skilled nursing facilities, assisted living and residential care facilities, integrated<br />
health systems, independent senior living communities and licensed in-home care agencies in<br />
53 Email from Ryan Deibert, OHOP Program Coordinator, February 15, 2008.<br />
54 <strong>Oregon</strong> Association <strong>of</strong> Hospitals and Health <strong>Systems</strong> website. Available online: http://www.oahhs.org/ (Accessed: January 14,<br />
2008).<br />
55 Jane Gross, “<strong>AIDS</strong> Patients Face Downside <strong>of</strong> Living Longer,” New York Times, January 6, 2008. Available online:<br />
http://www.nytimes.com/2008/01/06/health/06<strong>HIV</strong>.html?_r=1&hp=&adxnnl=1&oref=slogin&adxnnlx=1199656842-<br />
+Wb7LQvnXDGjucLalOJG/g (Accessed: January 10, 2008).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 21<br />
<strong>Oregon</strong> is represented by the <strong>Oregon</strong> Health Care Association (OHCA), among other associations. 56<br />
OHCA provides training in venues that include an annual fall convention and spring expo.<br />
One alternative approach to long-term hospitalization is to provide services to clients in their own<br />
homes. Funding for these services is limited, yet this approach may be an appropriate option for<br />
some clients. For example, Our House <strong>of</strong> Portland operates a program providing in-home care (such<br />
as nursing, social work, and occupational therapy) to people living with <strong>HIV</strong>/<strong>AIDS</strong> in the Portland<br />
Eligible Metropolitan Area. Because many funding streams do not allow this type <strong>of</strong> service, the<br />
agency must fundraise creatively to support its programs. For more information on this and other<br />
innovative agencies, please see Appendix 1: Affordable <strong>Housing</strong> Resource Guide.<br />
Affordable <strong>Housing</strong> Resources<br />
In the survey <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> service agencies in <strong>Oregon</strong>, the lack <strong>of</strong> affordable housing was the<br />
number-one barrier to stability for people living with <strong>HIV</strong>/<strong>AIDS</strong>, identified by all 16 respondents.<br />
Of all respondents (<strong>HIV</strong>/<strong>AIDS</strong> agencies and non-<strong>HIV</strong>/<strong>AIDS</strong> agencies), 78 percent responded that<br />
creating more housing opportunities for people living with <strong>HIV</strong>/<strong>AIDS</strong> was a high priority for<br />
systems integration in the balance <strong>of</strong> state.<br />
In October 2006, <strong>Oregon</strong> <strong>Housing</strong> and Community <strong>Services</strong> (OHCS) published an inventory <strong>of</strong><br />
housing units that are dedicated as affordable across the state. OHCS reported 54,522 units <strong>of</strong><br />
affordable housing statewide, including 23,881 units in the balance <strong>of</strong> state, or 44 percent <strong>of</strong> the<br />
total. The population <strong>of</strong> the balance <strong>of</strong> state is 54 percent <strong>of</strong> the total <strong>Oregon</strong> population. 57<br />
Developing new affordable housing resources usually requires accessing funding sources from<br />
multiple levels <strong>of</strong> government. The following sections describe the main sources <strong>of</strong> affordable<br />
housing funding in <strong>Oregon</strong> and the planning processes that determine funding priorities. Affordable<br />
housing resources include federal and state program funds allocated through the state Consolidated<br />
Plan and Consolidated Funding Cycle and local Consolidated Plans, Low Income <strong>Housing</strong> Tax<br />
Credits, public housing authority resources, and the network <strong>of</strong> affordable housing developers in<br />
<strong>Oregon</strong>. The Continuum <strong>of</strong> Care planning process is discussed in the following section on homeless<br />
services, as it funds both services and housing targeted at reducing homelessness.<br />
The <strong>Oregon</strong> <strong>State</strong> Consolidated Plan and Consolidated Funding Cycle<br />
Consolidated Plans (Con Plans) are comprehensive planning documents required by the U.S.<br />
Department <strong>of</strong> <strong>Housing</strong> and Urban Development (HUD) for all states, large cities, and urban<br />
counties that receive Community Development Block Grant (CDBG), Emergency Shelter Grants<br />
(ESG), HOME Investment Partnerships Program (HOME), and/or <strong>Housing</strong> Opportunities for<br />
Persons with <strong>AIDS</strong> (HOPWA) funding. Of these, CDBG, HOME, and HOPWA can all support<br />
development activities. This planning process is intended to help local jurisdictions receive public<br />
input, develop a vision for housing and community development, and coordinate their activities.<br />
Con Plans are generally submitted on a five-year cycle, with annual action plans to describe<br />
activities expected in the coming year.<br />
56 <strong>Oregon</strong> Health Care Association website. Available online: http://www.ohca.com/ (Accessed: January 14, 2008).<br />
57 <strong>Oregon</strong> <strong>Housing</strong> and Community <strong>Services</strong>. Low Income <strong>Housing</strong> <strong>State</strong>-wide List. Available online: http://www.ohcs.oregon.gov/<br />
(Accessed: November 28, 2007).
22 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
For the <strong>State</strong> <strong>of</strong> <strong>Oregon</strong> (as opposed to the <strong>Oregon</strong> cities and counties which plan independently),<br />
different state agencies take the lead on different programs which are included in the Consolidated<br />
Plan process. As noted previously, HOPWA is administered by the <strong>HIV</strong> Care and Treatment<br />
Program, within the Department <strong>of</strong> Human <strong>Services</strong> (DHS). The <strong>Oregon</strong> Economic and Community<br />
Development Department (OECDD) administers CDBG funds based on the Con Plan guidelines.<br />
<strong>Oregon</strong> <strong>Housing</strong> and Community <strong>Services</strong> (OHCS) releases HOME and ESG funds through its<br />
Consolidated Funding Cycle (CFC), with funding rounds in the fall and spring. The OHCS CFC<br />
also includes the <strong>Oregon</strong> allocation <strong>of</strong> federal Low Income <strong>Housing</strong> Tax Credit (LIHTC) funding,<br />
the <strong>Oregon</strong> Affordable <strong>Housing</strong> Tax Credit program, the <strong>Housing</strong> Development Grant (Trust Fund)<br />
program, the Low-Income Weatherization program, and the HELP (Financing Adjustment Factor<br />
Savings Fund) program. (LIHTC is also affected by a separate planning process, the Qualified<br />
Allocation Plan, discussed below.) Funding is released through the Spring and Fall funding cycles.<br />
<strong>Housing</strong> and service providers were asked in the stakeholder survey if their agencies participated in<br />
the Con Plan planning processes. Forty-four percent <strong>of</strong> agencies that did not specifically serve<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong> reported participating in their Con Plan planning process, compared<br />
to just seven percent <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> agencies. Of all respondents, 64 percent did not know how well<br />
their Con Plan included the housing and services needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
The needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong> have not historically been well represented in the Con<br />
Plan planning processes. However, there are opportunities to increase recognition <strong>of</strong> the needs <strong>of</strong><br />
people living with <strong>HIV</strong>/<strong>AIDS</strong> in these planning processes. For the past several years, the state Con<br />
Plan has identified people living with <strong>HIV</strong>/<strong>AIDS</strong> as a high priority among special needs<br />
populations. In 2007, the OHOP Program Coordinator participated in the development <strong>of</strong> the<br />
Annual Action Plan for the state Con Plan, and provided information on the housing needs for<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
The CFC guidelines set aside 30 percent <strong>of</strong> funding for targeted populations and OHCS priorities.<br />
In 2007, the CFC guidelines targeted special needs populations, which were defined as “farm<br />
workers, developmentally disabled, chronically mentally ill, chronically homeless (including single<br />
persons under the HUD definition <strong>of</strong> chronically homeless, and homeless families), and ex<strong>of</strong>fenders.”<br />
The Spring 2008 CFC scaled back the populations targeted by the 30 percent set aside.<br />
For this round, the set asides will include:<br />
• <strong>Housing</strong> for developmentally disabled populations;<br />
• <strong>Housing</strong> for the homeless, utilizing <strong>Housing</strong> PLUS resources; and<br />
• Preservation <strong>of</strong> existing affordable housing units.<br />
The CFC also has a performance target that 50 percent <strong>of</strong> funded units serve special needs<br />
populations. OHCS has not met this target since 2002, so there may be an opportunity to more<br />
aggressively target housing for people with disabilities, including <strong>HIV</strong>/<strong>AIDS</strong>, in the next CFC<br />
round. 58<br />
One <strong>of</strong> the important programs funded through the CFC is the HOME tenant-based assistance<br />
(TBA) voucher program, which can be a valuable tool for assisting clients to gain access to housing<br />
and develop self-sufficiency. Several Community Action Programs in <strong>Oregon</strong> operate the TBA<br />
58 <strong>Oregon</strong> <strong>Housing</strong> and Community <strong>Services</strong>. 2006-2007 Consolidated Funding Cycle Guidelines. Available online:<br />
www.oregon.gov/OHCS/HRS_CFC_Overview.shtml (Accessed: November 28, 2007).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 23<br />
programs, which have been used extensively in <strong>Oregon</strong> since the inception <strong>of</strong> the HOME<br />
program. 59 HOME TBA is designed to be transitional, with the housing subsidy expiring after 24<br />
months, during which time the tenant works toward a personal self-sufficiency plan.<br />
While HOME TBA administrators can include program preferences for people with <strong>HIV</strong>/<strong>AIDS</strong> or<br />
other special needs, in order to maintain successful self-sufficiency programs, they must select<br />
clients that are likely to resolve financial issues and increase their income by the end <strong>of</strong> the subsidy<br />
period. 60 For example, ACCESS Inc. in Jackson County created a secondary preference for people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong> in their HOME TBA self-sufficiency program, but reported some negative<br />
experiences after receiving referrals <strong>of</strong> clients who were probably better suited for long-term<br />
housing assistance. ACCESS and the OHOP Region 3 <strong>Housing</strong> Coordinator plan to work together<br />
to ensure the careful use <strong>of</strong> that preference for appropriate clients with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
One new affordable housing development opportunity that <strong>HIV</strong>/<strong>AIDS</strong> housing and services<br />
stakeholders may access through the CFC is the <strong>Housing</strong> PLUS (Permanent Living Utilizing<br />
<strong>Services</strong>) program, which will help finance permanent supportive housing for formerly homeless<br />
people. The program includes $16 million that will leverage additional funding to create 150 units.<br />
The first $4 million will be awarded by OHCS through the Spring 2008 CFC. Stakeholders across<br />
the state, including housing authorities and nonpr<strong>of</strong>it developers, have expressed interest in<br />
pursuing this new funding source. By <strong>of</strong>fering the leverage <strong>of</strong> support services and/or rental<br />
subsidy, the OHOP program may be able to partner with an affordable housing developer to make<br />
units available for formerly homeless people living with <strong>HIV</strong>/<strong>AIDS</strong>, as described below in the<br />
“Recommendations” section. For more information on this particular program, please refer to the<br />
contacts listed in Appendix 1: Affordable <strong>Housing</strong> Resource Guide.<br />
Local CDBG and HOME Funds<br />
Seven cities in the balance <strong>of</strong> state receive CDBG and/or HOME allocations and are required to<br />
prepare their own Con Plans: Ashland, Bend, Eugene, Corvallis, Medford, Salem, and Springfield<br />
(Eugene and Springfield submit a combined Con Plan).<br />
Most <strong>of</strong> these city Con Plans do not directly address the housing needs <strong>of</strong> people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong>. Both the City <strong>of</strong> Bend and the City <strong>of</strong> Medford Con Plans describe persons living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> as a “Low” priority among special needs populations. 61<br />
Table 6 on the following page summarizes the <strong>Oregon</strong> formula allocations for the CDBG and<br />
HOME programs for Fiscal Year 2007.<br />
59 “<strong>State</strong>s, HOME, and Tenant-Based Assistance,” Council <strong>of</strong> <strong>State</strong> Community Development Agencies, 1997. Available online:<br />
http://www.coscda.org/publications/TBA.htm (Accessed: November 30, 2007).<br />
60 Ibid.<br />
61 City <strong>of</strong> Bend. Consolidated Plan 2004-2009. Available online:<br />
http://www.ci.bend.or.us/depts/urban_renewal_economic_development/ (Accessed: November 28, 2007); and City <strong>of</strong> Medford.<br />
Consolidated Plan 2005-2009. Available online: http://www.ci.medford.or.us/Page.asp?NavID=632 (Accessed: November 28, 2007).
24 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Table 6:<br />
CDBG and HOME Allocations for <strong>Oregon</strong> <strong>Balance</strong> <strong>of</strong> <strong>State</strong>, Fiscal Year 2007<br />
Grantee CDBG HOME Total<br />
City <strong>of</strong> Ashland $212,738 $0 $212,738<br />
City <strong>of</strong> Bend $437,156 $0 $437,156<br />
City <strong>of</strong> Corvallis $556,048 $420,259 $976,307<br />
City <strong>of</strong> Eugene* $1,415,794 $1,451,705 $2,867,499<br />
City <strong>of</strong> Medford $636,217 $0 $636,217<br />
City <strong>of</strong> Salem $1,487,449 $924,794 $2,412,243<br />
City <strong>of</strong> Springfield* $628,101 $0 $628,101<br />
Subtotal for <strong>Balance</strong> <strong>of</strong> <strong>State</strong>: $5,373,503 $2,796,758 $8,170,261<br />
City <strong>of</strong> Beaverton $612,738 $0 $612,738<br />
City <strong>of</strong> Gresham $903,182 $0 $903,182<br />
City <strong>of</strong> Hillsboro $666,584 $0 $666,584<br />
City <strong>of</strong> Portland $10,441,050 $4,306,019 $14,747,069<br />
Clackamas County $2,171,598 $1,038,996 $3,210,594<br />
Multnomah County $302,746 $0 $302,746<br />
Washington County $2,057,753 $1,639,790 $3,697,543<br />
Subtotal for Portland EMA: $17,155,651 $6,984,805 $24,140,456<br />
<strong>Oregon</strong> <strong>State</strong> Program $14,314,757 $10,672,782 $24,987,539<br />
Total for <strong>Oregon</strong>: $36,843,911 $20,454,345 $57,298,256<br />
Source: U.S. <strong>Housing</strong> and Urban Development. 2007 Formula Allocations. Available online:<br />
http://www.hud.gov/<strong>of</strong>fices/cpd/about/budget/budget07/states/or.xls (Accessed: November 29, 2007).<br />
Note: the Cities <strong>of</strong> Eugene and Springfield submit a joint Consolidated Plan and issue joint funding announcements<br />
for their combined CDBG and HOME allocations.<br />
Low Income <strong>Housing</strong> Tax Credits<br />
Although Low Income <strong>Housing</strong> Tax Credits (LIHTC) funding is released through the OHCS<br />
Consolidated Funding Cycle, the program is additionally subject to guidelines established through<br />
the <strong>Oregon</strong> Qualified Allocation Plan (QAP), which OHCS also coordinates. Like the Con Plans,<br />
the QAP is open to public input. The 2007 QAP does not mention <strong>HIV</strong>/<strong>AIDS</strong>, and does not<br />
prioritize supportive housing or housing for people with special needs. 62<br />
<strong>Housing</strong> and service providers were asked how well the QAP served the needs <strong>of</strong> people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong>. Eighty-two percent <strong>of</strong> all respondents said that they did not know how well, and 11<br />
62 <strong>Oregon</strong> <strong>Housing</strong> and Community <strong>Services</strong>. 2007 Qualified Allocation Plan. Available online:<br />
www.ohcs.oregon.gov/OHCS/HRS_LIHTC_Program.shtml (Accessed: November 28, 2007).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 25<br />
percent responded “Not well.” This general lack <strong>of</strong> familiarity among <strong>HIV</strong>/<strong>AIDS</strong> stakeholders with<br />
priorities <strong>of</strong> the QAP (along with other housing planning processes) presents a challenge, as<br />
described in the “Critical Issues” chapter below.<br />
<strong>Housing</strong> Authorities<br />
Public housing authorities (PHAs) play a vital role in providing affordable housing in the balance <strong>of</strong><br />
state. PHAs are local governmental bodies that are authorized by state legislation to develop and/or<br />
administer public rental housing for low-income households, <strong>of</strong>ten making them the largest<br />
landlords in urban areas. In addition, PHAs administer the federal Section 8 <strong>Housing</strong> Choice<br />
Voucher Program, which provides rental assistance to individuals and families in privately-owned<br />
housing. There are 21 housing authorities in <strong>Oregon</strong>, including 17 outside the Portland EMA. PHA<br />
resources in the balance <strong>of</strong> state include 2,230 units <strong>of</strong> public housing and 19,026 Section 8<br />
<strong>Housing</strong> Choice Vouchers.<br />
Compared to the Portland EMA, housing resources in the balance <strong>of</strong> state rely more heavily on<br />
Section 8 than public housing. The housing authorities in the balance <strong>of</strong> state have 59 percent <strong>of</strong> the<br />
state’s Section 8 vouchers, and only 38 percent <strong>of</strong> the public housing units. 63 Most PHAs have long<br />
waiting lists for Section 8, and some have closed their lists to new applicants in response to<br />
decreasing federal funding and high demand for affordable housing. This is a critical piece <strong>of</strong><br />
context for people living with <strong>HIV</strong>/<strong>AIDS</strong> who need housing assistance, as HOPWA and other<br />
programs targeted to this population emphasize the importance <strong>of</strong> transitioning clients whenever<br />
possible to mainstream housing assistance, <strong>of</strong> which Section 8 is the single largest source.<br />
Table 7 on the following page shows the number <strong>of</strong> public housing units and Section 8 <strong>Housing</strong><br />
Choice Vouchers for each housing authority in <strong>Oregon</strong>.<br />
63 Source: U.S. <strong>Housing</strong> and Urban Development. <strong>Housing</strong> Authority Pr<strong>of</strong>iles. Available online:<br />
https://pic.hud.gov/pic/hapr<strong>of</strong>iles/hapr<strong>of</strong>ilelist.asp (Accessed: November 29, 2007).
26 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Table 7:<br />
Public <strong>Housing</strong> and Section 8 Resources for <strong>Oregon</strong> <strong>Housing</strong> Authorities<br />
<strong>Housing</strong> Authority<br />
Public<br />
<strong>Housing</strong> Units<br />
Section 8<br />
Vouchers<br />
Total<br />
Coos-Curry Counties 52 777 829<br />
Douglas County 155 651 806<br />
<strong>Housing</strong> Authority and Community <strong>Services</strong><br />
Agency (HACSA)<br />
708 2,639 3,347<br />
<strong>Housing</strong> Works (formerly CORHA) 48 1,026 1,074<br />
Jackson County 130 1,605 1,735<br />
Josephine <strong>Housing</strong> Council 0 842 842<br />
Klamath County 57 734 791<br />
Lincoln County 120 497 617<br />
Linn-Benton Counties 0 2,435 2,435<br />
Malheur County 40 349 389<br />
Marion County 46 1,175 1,221<br />
Mid-Columbia <strong>Housing</strong> Authority 0 551 551<br />
Northeast <strong>Oregon</strong> <strong>Housing</strong> Authority (NEOHA) 129 710 839<br />
Northwest <strong>Oregon</strong> <strong>Housing</strong> Authority (NOHA) 0 1,139 1,139<br />
Salem (SHA) 337 2,868 3,205<br />
Umatilla County 118 329 447<br />
West Valley <strong>Housing</strong> Authority 380 699 1,079<br />
Subtotal <strong>Balance</strong> <strong>of</strong> <strong>State</strong>: 2,320 19,026 21,346<br />
Clackamas County 567 1,542 2,109<br />
Portland (HAP) 2,896 7,723 10,619<br />
Yamhill County 70 1,303 1,373<br />
Washington County 293 2,576 2,869<br />
Subtotal Portland EMA: 3,826 13,144 16,970<br />
Total for <strong>Oregon</strong>: 6,146 32,170 38,316<br />
Source: U.S. <strong>Housing</strong> and Urban Development. <strong>Housing</strong> Authority Pr<strong>of</strong>iles. Available online:<br />
https://pic.hud.gov/pic/hapr<strong>of</strong>iles/hapr<strong>of</strong>ilelist.asp (Accessed: November 29, 2007).<br />
In addition to administering public housing and Section 8, some housing authorities play other roles<br />
in the community. For example, the housing authority in Lane County—<strong>Housing</strong> Authority and<br />
Community <strong>Services</strong> Agency (HACSA)—provides an extensive weatherization program that lowers<br />
utilities costs for low-income homes. Some housing authorities, including the Salem <strong>Housing</strong><br />
Authority, HACSA, the <strong>Housing</strong> Authority <strong>of</strong> Jackson County, the Umatilla <strong>Housing</strong> Authority, and<br />
<strong>Housing</strong> Works, have developed hundreds <strong>of</strong> units <strong>of</strong> affordable housing using tax credits and other<br />
competitive funding sources.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 27<br />
The survey <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> providers in the balance <strong>of</strong> state indicated that 56 percent had partnerships<br />
with local housing authorities. Over two-thirds <strong>of</strong> all respondents (both <strong>HIV</strong>/<strong>AIDS</strong> agencies and<br />
non-<strong>HIV</strong>/<strong>AIDS</strong> agencies) wanted to see PHAs more involved in efforts to improve systems<br />
integration <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> housing and services.<br />
The evaluation <strong>of</strong> the OHOP program identified long PHA wait lists as a challenge for transitioning<br />
OHOP clients to mainstream resources in order to be able to provide services to additional OHOPeligible<br />
clients. Wait list length and policy varies among PHAs in <strong>Oregon</strong>’s balance <strong>of</strong> state: for<br />
example, the <strong>Housing</strong> Authority <strong>of</strong> Jackson County keeps an open Section 8 wait list, which has run<br />
to as much as four years and more recently is about two and a half years long. The <strong>Housing</strong><br />
Authority and Community <strong>Services</strong> Agency <strong>of</strong> Lane County (HACSA), by contrast, closed its wait<br />
list in October 2005, and is serving July 2004 applicants. Most housing authorities in eastern<br />
<strong>Oregon</strong>, where affordable housing resources are particularly limited, have closed wait lists as well.<br />
<strong>Housing</strong> authorities have considerable discretion over whether to prioritize specific populations,<br />
such as people with disabilities, formerly homeless persons, or veterans, for either Section 8 (tenant-<br />
or project-based vouchers), or public housing. Most PHAs in the balance <strong>of</strong> state have not<br />
prioritized special needs populations for either program. One housing authority explained that they<br />
cannot mandate or fund services in their properties, and would be concerned about additional<br />
administrative costs <strong>of</strong> serving people with special needs. They cited bad experiences with<br />
placements in which tenants with personal challenges such as substance abuse histories were<br />
inadequately supported by services and relapsed. They also felt a no-preference policy was<br />
perceived as more fair by people in their jurisdiction.<br />
Another housing authority said that it did not have the staff capacity to assist people with<br />
disabilities to find housing once they received their vouchers. For the most part, PHA staff was<br />
unaware <strong>of</strong> the housing and case management services that are available for people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong>. This may point to a need for more robust or explicit agreements between service<br />
providers and housing providers, in order to encourage the latter to more actively use preferences.<br />
Increased efficiency and higher success rates stemming from this type <strong>of</strong> partnership could serve as<br />
a counterbalance to the administrative difficulty or public opposition that PHAs currently associate<br />
with preferences.<br />
Affordable <strong>Housing</strong> Developers<br />
<strong>Oregon</strong> has a strong network <strong>of</strong> affordable housing developers (including private agencies as well<br />
as PHAs) that leverage and combine limited resources to produce new housing for low-income<br />
households. Informants across most areas <strong>of</strong> the state reported that affordable housing developers<br />
had the expertise and skills needed for development, but were limited in their ability to take on<br />
additional projects to meet demand due to scarce funding resources.<br />
The survey <strong>of</strong> stakeholders asked what types <strong>of</strong> agencies would they like to see more involved in<br />
system integration efforts, and the highest number <strong>of</strong> respondents (88 percent) chose affordable<br />
housing agencies. Only 44 percent <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> agencies reported currently partnering with<br />
developers in their region (An example <strong>of</strong> this kind <strong>of</strong> partnership could be setting aside a number<br />
<strong>of</strong> units for people living with <strong>HIV</strong>/<strong>AIDS</strong> within larger affordable housing projects, given a<br />
commitment <strong>of</strong> rental subsidy).
28 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
By necessity, most developers look for new opportunities and housing approaches to access and<br />
leverage new funding sources. Developers interviewed for this plan mentioned several new projects<br />
they are examining that may benefit from partnering with service agencies. For example, several<br />
mentioned the new <strong>Housing</strong> PLUS funds for permanent supportive housing.<br />
The <strong>Housing</strong> Authority <strong>of</strong> Jackson County, which historically has not developed special needs<br />
housing, is looking at different potential scenarios for its first such project. One possibility is a<br />
Single Room Occupancy (SRO) project to serve formerly homeless individuals. Another possibility<br />
is the incorporation <strong>of</strong> special needs units into a large mixed-use, mixed-income redevelopment<br />
project in downtown Medford.<br />
<strong>Housing</strong> authorities have the ability to project-base a percentage <strong>of</strong> their overall Section 8 voucher<br />
allocation, which can be especially valuable for projects serving households below 30 percent <strong>of</strong><br />
Area Median Income (AMI). In most projects serving households at or below 30 percent <strong>of</strong> AMI,<br />
the rents collected from tenants are insufficient for covering the building’s operating costs. Projectbased<br />
Section 8 vouchers can help fill the gap between revenue and the project’s ongoing expenses.<br />
Jackson County reported that it has project-based a small number <strong>of</strong> vouchers, and is open to<br />
creating more to support new developments.<br />
In 2006, the City <strong>of</strong> Bend implemented an Affordable <strong>Housing</strong> Fee to provide new local funding for<br />
affordable housing. Revenue for the fund is provided through a fee assessed to new development in<br />
the city. The fee, 0.3 percent (one third <strong>of</strong> one percent) <strong>of</strong> the total Building Permit Valuation for<br />
new developments, is expected to provide about two million dollars per year for new construction<br />
and rehabilitation <strong>of</strong> affordable homeownership and rental housing. Local agencies apply<br />
competitively to the City <strong>of</strong> Bend for the funds, which are intended to be used to leverage state and<br />
federal financing for affordable housing initiatives. 64<br />
Other Affordable <strong>Housing</strong> Resources and Opportunities<br />
A number <strong>of</strong> large private service providers across the state manage affordable housing units that<br />
they or other entities have developed. Like housing authorities, other housing providers also employ<br />
a range <strong>of</strong> different wait list and tenant preference models. ShelterCare, in Eugene, maintains a<br />
centralized waiting list to place homeless people in housing that runs about nine to 12 weeks long.<br />
The agency selects people from its wait list whose needs (based on intake assessments) match the<br />
attributes <strong>of</strong> units that become available – for example, the staffing level and neighborhood that the<br />
units are in. In contrast, St. Vincent de Paul in Lane County does not maintain a wait list for its<br />
service-enriched housing, but instead accepts applications for referrals from social services agencies<br />
when a unit opens up.<br />
OHCS contracts with 13 Regional <strong>Housing</strong> Centers, including 11 serving the balance <strong>of</strong> state. These<br />
centers provide housing information and referrals to low-income renters and homeowners. Only one<br />
out <strong>of</strong> 16 <strong>HIV</strong>/<strong>AIDS</strong> service agencies from the stakeholder survey reported partnering with<br />
Regional <strong>Housing</strong> Centers. These centers can potentially assist both outreach by the OHOP<br />
program, and referrals for OHOP clients to additional housing resources.<br />
64 City <strong>of</strong> Bend, Department <strong>of</strong> Urban Renewal and Economic Development.<br />
http://www.ci.bend.or.us/depts/urban_renewal_economic_development (Accessed: November 30, 2007).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 29<br />
There are also occasional opportunities across the balance <strong>of</strong> state for housing providers to connect<br />
and share information on housing needs and programs. Each April, <strong>Oregon</strong> <strong>Housing</strong> and<br />
Community <strong>Services</strong> (OHCS) hosts the <strong>Oregon</strong> <strong>Housing</strong> Conference, which includes presentations<br />
from housing agencies across the state. Another example <strong>of</strong> a regional housing forum was the<br />
February 2006 Southern <strong>Oregon</strong> Workforce <strong>Housing</strong> Summit, which included representatives from<br />
Curry, Jackson, and Josephine Counties. 65<br />
Homeless <strong>Services</strong> and Prevention<br />
The impacts <strong>of</strong> homelessness can be particularly devastating for people living with <strong>HIV</strong>/<strong>AIDS</strong>, for<br />
whom housing stability is directly linked with access to treatment and health outcomes. Despite the<br />
need for homeless services and prevention for people living with <strong>HIV</strong>/<strong>AIDS</strong>, stakeholders reported<br />
limited involvement by <strong>HIV</strong>/<strong>AIDS</strong> housing and services providers in key homeless services<br />
planning processes. Agency-level links may exist (such as referral <strong>of</strong> clients to faith- or other<br />
community-based homeless shelters, as a bridge to permanent housing and other services), but<br />
understanding and accessing homelessness system planning is critical to meeting joint challenges.<br />
The following sections describe the two key planning processes: the Continuum <strong>of</strong> Care system, and<br />
state and local 10-Year Plans to End Homelessness.<br />
Continuum <strong>of</strong> Care Process<br />
The Continuum <strong>of</strong> Care system is a regional planning process that includes a combined annual<br />
application for HUD’s primary homeless assistance programs, including the Supportive <strong>Housing</strong><br />
Program (SHP), Single Room Occupancy (SRO) Program, and Shelter Plus Care. Like the<br />
Consolidated Plan process, the Continuum <strong>of</strong> Care provides opportunities for regional systems to<br />
set priorities for federal funding.<br />
There are five Continua <strong>of</strong> Care that cover the balance <strong>of</strong> state. Each Continuum is allocated an<br />
initial pro rata need funding amount based on the relative homeless assistance need determined by<br />
HUD. Communities can receive funding above this level through successful applications for<br />
“bonus” projects that must provide permanent housing for chronically homeless individuals.<br />
65 Southern <strong>Oregon</strong> Workforce <strong>Housing</strong> Summit. Available online: http://www.ashland.or.us/Files/wfh_book_final.pdf (Accessed:<br />
January 15, 2008).
30 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Table 8 shows the five Continua in the balance <strong>of</strong> state and their Fiscal Year 2006 funding<br />
allocations.<br />
Table 8:<br />
Continuum <strong>of</strong> Care Funding Allocations for Fiscal Year 2006<br />
Continuum <strong>of</strong> Care (CoC) FY 2006 Funding<br />
Central <strong>Oregon</strong> CoC $296,759<br />
Rural <strong>Oregon</strong> CoC (ROCC) $1,473,673<br />
Medford / Ashland / Jackson CoC $267,563<br />
Eugene / Springfield / Lane CoC $1,995,205<br />
Salem / Marion / Polk CoC $726,978<br />
Total for <strong>Balance</strong> <strong>of</strong> <strong>State</strong>: $4,760,178<br />
Total for <strong>Oregon</strong>: $12,707,015<br />
<strong>Housing</strong> and service providers were asked if their agencies participated in the Continuum <strong>of</strong> Care<br />
planning processes. Fifty percent <strong>of</strong> agencies that did not specifically serve people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> reported participating in their Continuum <strong>of</strong> Care, compared to just 13 percent <strong>of</strong><br />
<strong>HIV</strong>/<strong>AIDS</strong> agencies. Of all respondents, 67 percent did not know how well their Continuum <strong>of</strong> Care<br />
included the housing and services needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong>, and 17 percent<br />
respondened “Not well.”<br />
For Fiscal Year 2006, providers from the balance <strong>of</strong> state received only 37 percent <strong>of</strong> the state’s<br />
Continuum <strong>of</strong> Care funding. Representatives from local Continua <strong>of</strong> Care indicated that<br />
administrative requirements are an obstacle for many providers in the balance <strong>of</strong> state, particularly<br />
for Shelter Plus Care. Shelter Plus Care programs must ensure that clients meet HUD’s homeless<br />
definitions, and provide a one-to-one services funding match.<br />
For example, if the Salem/Marion/Polk Continuum <strong>of</strong> Care applied for a new bonus project next<br />
year, the maximum award available would be approximately $30,000 per year for two years. This<br />
limited funding may support three Shelter Plus Care vouchers, but would represent a new<br />
administrative cost for the sponsor agency and would require finding a substantial service match.<br />
Stakeholders in several regions <strong>of</strong> the state mentioned the potential opportunities for OHOP to<br />
leverage HOPWA and Ryan White resources by providing service matches and critical<br />
administrative functions for Continuum <strong>of</strong> Care programs. For example, <strong>Housing</strong> and Community<br />
<strong>Services</strong> Agency <strong>of</strong> Lane County (HACSA) and ShelterCare currently partner to run the only<br />
Shelter Plus Care program in the balance <strong>of</strong> state. To ensure that the program is maximizing its<br />
client capacity, they have begun discussion with <strong>HIV</strong> Care and Treatment to make some program<br />
slots available for OHOP clients.<br />
10-Year Plans to End Homelessness<br />
In 2006, <strong>Oregon</strong>’s Governor created the Ending Homelessness Advisory Council (EHAC) to<br />
develop the 10-Year Plan to End Homelessness in <strong>Oregon</strong>. In 2007, EHAC released a draft <strong>of</strong> the
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 31<br />
first section <strong>of</strong> the 10-Year Plan, “Understanding Homelessness in <strong>Oregon</strong>.” 66 Stakeholders indicate<br />
that the Council is still in its early planning stages. EHAC has focused thus far on understanding the<br />
extent <strong>of</strong> the problem and developing a case for more resources and improved coordination between<br />
agencies to use funding more effectively.<br />
Several counties in the balance <strong>of</strong> state, including Coos, Jackson, Lane, Lincoln, and Marion, are in<br />
the process <strong>of</strong> developing or implementing 10-Year Plans. Some counties have used the 10-Year<br />
Plan process to improve community awareness <strong>of</strong> homelessness issues. For example, the Lane<br />
County Project Homeless Connect (a one-day event to match drop-in homeless clients directly with<br />
services and resources in the community) served over 1,000 homeless people in February 2007. 67<br />
The survey <strong>of</strong> housing and service providers asked respondents if their agencies participated in the<br />
development <strong>of</strong> a local or statewide 10-Year Plan. Of agencies that did not specifically serve people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong>, 50 percent reported participating in their 10-Year Plan, compared to just 13<br />
percent <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> agencies. Of all respondents, 62 percent did not know how well their 10-Year<br />
Plan included the housing and services needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong>, and 21 percent<br />
responded “Not well.”<br />
Addictions and Mental Health <strong>Services</strong><br />
People with chemical dependency and/or mental illness face substantial barriers to housing. A 2005<br />
survey <strong>of</strong> <strong>Oregon</strong> community mental health programs found that more than 5,000 people with<br />
mental illness and over 2,000 alcohol and drug treatment clients were in immediate need <strong>of</strong><br />
affordable housing. Approximately 3,000 adults with mental illness and 3,000 people with<br />
substance abuse disorders were estimated to be currently homeless. The vacancy rates for all types<br />
<strong>of</strong> mental health and alcohol and drug housing programs were reported at well under five percent,<br />
indicating a very high utilization <strong>of</strong> existing housing resources. 68<br />
People living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong> have identified a high level <strong>of</strong> need for behavioral health<br />
treatment. More than three-quarters <strong>of</strong> Ryan White clients reported suffering from a mental health<br />
problem in the past 12 months. 69 People living with <strong>HIV</strong>/<strong>AIDS</strong> and co-occurring mental illness are<br />
significantly more likely to need ongoing help with housing (50 percent versus 31 percent <strong>of</strong> clients<br />
without mental health needs). Homelessness was similarly associated with behavioral health needs<br />
among people living with <strong>HIV</strong>/<strong>AIDS</strong>. 70<br />
The latest OHOP program evaluation identified clients with co-occurring mental illness as<br />
particularly difficult to serve. In addition, <strong>HIV</strong>/<strong>AIDS</strong> service providers in <strong>Oregon</strong> reported that<br />
many <strong>of</strong> their clients had co-occurring substance issues.<br />
66<br />
Ending Homelessness Advisory Council (EHAC). Draft 10 Year Plan to End Homelessness, Part 1: Understanding Homelessness<br />
in <strong>Oregon</strong>. Available online: http://www.ehac.oregon.gov (Accessed: November 27, 2007).<br />
67<br />
Ending Homeless Advisory Council. Summary <strong>of</strong> Local 10 Year Planning Efforts. Available online: www.ehac.oregon.gov<br />
(Accessed: November 29, 2007).<br />
68<br />
<strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Mental Health and Addiction <strong>Services</strong>. Results <strong>of</strong> the 2005 OMHAS <strong>Housing</strong> Survey.<br />
Available online: www.oregon.gov/dhs/mentalhealth/housing.shtml (Accessed: January 10, 2008).<br />
69<br />
<strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Ryan White Title II <strong>HIV</strong> Client <strong>Services</strong> Comprehensive Plan, 2006-2009. Available<br />
online: http://www.oregon.gov/DHS/ph/hiv/services/coalplan/2006plan.pdf (Accessed: November 27, 2007).<br />
70<br />
<strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Program Design and Evaluation <strong>Services</strong>. We Listened…2005: Survey for People Living<br />
with <strong>HIV</strong> and <strong>AIDS</strong> in <strong>Oregon</strong>. Available online: http://www.oregon.gov/DHS/ph/hiv/services/needs/reports.shtml (Accessed:<br />
November 27, 2007).
32 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
The Steering Committee identified the difficulty <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> clients accessing the limited number<br />
<strong>of</strong> crisis respite beds. There are a limited number <strong>of</strong> crisis beds across the state, and many rural<br />
counties lack any crisis respite beds. A 2005 report on community mental health programs<br />
identified 343 crisis respite beds in <strong>Oregon</strong>, including 288 in the balance <strong>of</strong> state, with an unmet<br />
need <strong>of</strong> over 250 beds. 71<br />
In order to access crisis-respite care, people living with <strong>HIV</strong>/<strong>AIDS</strong> must be enrolled in mental<br />
health services and receive referral from their mental health case workers. But many <strong>HIV</strong>/<strong>AIDS</strong><br />
clients do not have access to mental health case workers prior to crisis – a challenge addressed in<br />
the Critical Issues chapter below. In addition, some respite bed providers may be hesitant to accept<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong> due to lack <strong>of</strong> expertise in providing care for physical illnesses.<br />
Mental health stakeholders recommend that <strong>HIV</strong> case managers accompany clients to their initial<br />
meeting(s) with mental health case workers to coordinate treatment to meet the client’s needs.<br />
As described above, OHOP recently was awarded funding for a HOPWA Special Project <strong>of</strong><br />
National Significance (SPNS) to serve people living with <strong>HIV</strong>/<strong>AIDS</strong> and mental illness. This<br />
program will leverage HOPWA and Ryan White funds with behavioral health treatment provided<br />
by Cascadia Behavioral Health.<br />
In recent years, the <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Addictions and Mental Health (AMH)<br />
Division has increased its focus on the housing needs for people with mental illness or substance<br />
use issues. Three programs provide funding for housing development targeted at these populations.<br />
The newly-created Expanding Community Living Opportunities (ECLO) program provides funding<br />
for structured and specialized residential programs for individuals leaving state psychiatric<br />
hospitals; supportive housing for people leaving psychiatric hospitals, transitioning from youth to<br />
adult services, or who are ineligible for Medicaid; and housing development grants to develop new<br />
housing.<br />
The Community Mental Health <strong>Housing</strong> Fund supports the development <strong>of</strong> housing for persons<br />
with chronic mental illness. Up to $100,000 per project are available for creating new community<br />
housing opportunities for people with a serious mental illness; and these funds are distributed<br />
through an annual competitive application process conducted by AMH.<br />
The Alcohol and Drug Free <strong>Housing</strong> Fund supports the establishment <strong>of</strong> new housing for people in<br />
recovery from alcohol and drug abuse and who are actively involved in an approved treatment<br />
program. One million dollars are available through the ADF <strong>Housing</strong> Fund for the 2007-2009<br />
biennium.<br />
One potential opportunity for collaboration between behavioral health and <strong>HIV</strong>/<strong>AIDS</strong> services and<br />
housing providers is the development and strengthening <strong>of</strong> relationships between agencies serving<br />
special needs populations, and public housing authorities (PHAs) and nonpr<strong>of</strong>it housing providers.<br />
Few PHAs have priorities for mental health clients for Section 8 or other subsidized housing wait<br />
lists, and no priorities exist for alcohol and drug treatment clients. Community mental health<br />
providers did report working successfully with private landlords.<br />
71 <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Mental Health and Addiction <strong>Services</strong>. Results <strong>of</strong> the 2005 OMHAS <strong>Housing</strong> Survey.<br />
Available online: www.oregon.gov/dhs/mentalhealth/housing.shtml (Accessed: January 10, 2008).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 33<br />
Coordinating services integration is a particular challenge in rural areas. The multi-county Eastern<br />
<strong>Oregon</strong> Human <strong>Services</strong> Consortium (EOHSC) is one potential venue for improving systems<br />
integration. The EOHSC is a cooperative body <strong>of</strong> community mental health programs that addresses<br />
the practicalities <strong>of</strong> delivering mental health, alcohol and drug treatment, and developmental<br />
disability services to the widespread communities <strong>of</strong> Eastern <strong>Oregon</strong>, and represents the region’s<br />
interests to the state legislature. EOHSC includes the counties <strong>of</strong> Gilliam, Grant, Harney, Hood<br />
River, Malheur, Morrow, Sherman, Umatilla, Union, Wallowa, Wasco, and Wheeler. 72<br />
Human <strong>Services</strong> and Public Assistance<br />
The most recent <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> needs assessment estimated that two-thirds <strong>of</strong> people living<br />
with <strong>HIV</strong>/<strong>AIDS</strong> across the state have incomes below the federal poverty level. 73 People living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> frequently have an array <strong>of</strong> basic needs that are common to low-income people in<br />
general, that also may be linked to their medical condition. These can include food and nutritional<br />
assistance, medical insurance, transportation, hygiene, family support, and general financial needs.<br />
Many clients rely on entitlement programs, including Supplemental Security Income (SSI) and<br />
Social Security Disability Insurance (SSDI), which are administered directly by the federal<br />
government, and provide income support for people with disabilities. Clients may also seek and<br />
receive assistance from faith-based or other private relief organizations, which comprise an<br />
important part <strong>of</strong> the “safety net” in many communities.<br />
While mainstream public assistance and human service programs sometimes meet the needs <strong>of</strong><br />
people living with <strong>HIV</strong>/<strong>AIDS</strong> as they are, this population sometimes needs enhanced assistance. For<br />
example, some <strong>HIV</strong>/<strong>AIDS</strong> medications require high-calorie diets, and consumers with low incomes<br />
<strong>of</strong>ten need assistance purchasing food and designing well-balanced diets that meet those<br />
requirements.<br />
In the survey <strong>of</strong> service providers for this needs assessment, while 81 percent <strong>of</strong> respondents from<br />
<strong>HIV</strong>/<strong>AIDS</strong> agencies said that they had partnerships for food assistance, half <strong>of</strong> all respondents said<br />
that food and nutritional assistance was insufficient in their region. Fifty-six percent felt that<br />
increasing access to mainstream services such as food stamps and SSI/SSDI was one <strong>of</strong> the highest<br />
priorities for systems integration.<br />
The primary resources for meeting human services and general assistance needs (beyond what is<br />
covered by federal disability entitlements for those who qualify) tend to be state and local public<br />
assistance programs – historically known as welfare. The largest <strong>of</strong> these programs, Temporary Aid<br />
to Needy Families (TANF) and food stamps, are federally funded but administered by state agencies<br />
– in <strong>Oregon</strong>, by the Department <strong>of</strong> Human <strong>Services</strong> (DHS) Children, Adults and Families<br />
(CAF) Division. DHS also administers (through its Division <strong>of</strong> Medical Assistance Programs) the<br />
<strong>Oregon</strong> Health Plan, the state’s vehicle for administering Medicaid and other health funds, which<br />
may cover some basic services. Integration efforts among these programs has historically taken<br />
place at the level <strong>of</strong> state administrators, but integrated strategies must be reinforced at the local<br />
72<br />
Eastern <strong>Oregon</strong> Human <strong>Services</strong> Consortium. Available online: http://www.eoddr.com/aboutEohsc.html (Accessed: November 30,<br />
2007).<br />
73<br />
<strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Program Design and Evaluation <strong>Services</strong>. We Listened…2005: Survey for People Living<br />
with <strong>HIV</strong> and <strong>AIDS</strong> in <strong>Oregon</strong>. Available online: http://www.oregon.gov/DHS/ph/hiv/services/needs/reports.shtml (Accessed:<br />
November 27, 2007).
34 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
level, across the 110 <strong>of</strong>fices that DHS operates in 16 service delivery areas across <strong>Oregon</strong>, in order<br />
for these programs to cooperate effectively.<br />
<strong>Oregon</strong> counties and municipalities also <strong>of</strong>fer a range <strong>of</strong> human services and assistance programs,<br />
which vary widely from county to county. The structure <strong>of</strong> coordination among the local and state<br />
agencies and private or non-pr<strong>of</strong>it service providers also varies. The following are three examples <strong>of</strong><br />
human services integration efforts across the balance <strong>of</strong> state:<br />
• Lane County coordinates human service delivery with the cities <strong>of</strong> Eugene and Springfield,<br />
through the intergovernmental Human <strong>Services</strong> Commission, the region’s CAP agency,<br />
which also coordinates the region’s HUD Continuum <strong>of</strong> Care application.<br />
• The Association <strong>of</strong> <strong>Oregon</strong> Counties has affiliate organizations for particular types <strong>of</strong><br />
administrators involved in health and human services programming, including the Coalition<br />
<strong>of</strong> County Children and Families Commissions and <strong>Oregon</strong> Coalition <strong>of</strong> Local Health<br />
Officials. 74<br />
• In Jackson County, the Rogue Valley Family Center serves as a “one-stop” family resource<br />
center for a collection <strong>of</strong> services and assistance programs provided by different agencies.<br />
Though this model has been difficult to sustain in <strong>Oregon</strong> communities, in part because <strong>of</strong><br />
declines in county budgets, it is nationally recognized as a best practice for serving lowincome<br />
people who may be involved in a range <strong>of</strong> different public systems and have limited<br />
access to transportation or ability to keep appointments in multiple locations. The Rogue<br />
Valley facility focuses on families with children, and has staff “mentors” who conduct<br />
intake meetings with each client to help identify and meet the needs <strong>of</strong> his or her household<br />
as a whole. Staff conduct monthly Program Integration Team meetings, as well as weekly<br />
staffing meetings around particular clients. Some housing assistance is currently available<br />
through onsite staff <strong>of</strong> a local nonpr<strong>of</strong>it provider.<br />
Employment<br />
Many people living with <strong>HIV</strong>/<strong>AIDS</strong> are able and willing to do some kind <strong>of</strong> income-generating<br />
work, but face barriers related to periods <strong>of</strong> absence from the workforce, limited education or skills,<br />
or other risk factors. Those with low or no income may need assistance finding, obtaining, and<br />
retaining jobs. In the survey <strong>of</strong> <strong>Oregon</strong> stakeholders, nearly two thirds <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> agencies<br />
reported that employment assistance was unavailable or insufficient in their communities. Less than<br />
half <strong>of</strong> all respondents (both <strong>HIV</strong>/<strong>AIDS</strong> agencies and non-<strong>HIV</strong>/<strong>AIDS</strong> agencies) partnered with<br />
employment services agencies. Sixty-nine percent <strong>of</strong> all respondents listed “improve economic selfsufficiency<br />
<strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong>” as a high priority for systems integration.<br />
<strong>Oregon</strong> receives federal Workforce Investment Act (WIA) funding to provide an array <strong>of</strong> services<br />
to job seekers and businesses in <strong>of</strong>fices throughout the state. Most <strong>of</strong> these <strong>of</strong>fices are called<br />
WorkSource <strong>Oregon</strong> One Stop Career Centers and are co-located with the Employment Department<br />
and other agency partners. Five <strong>of</strong> the seven One Stop Career Centers serve the balance <strong>of</strong> state.<br />
These centers provide anyone who walks in the door with information to help them get a job or<br />
potentially go to school to train in a new career direction. <strong>Services</strong> may include information<br />
74 The Association <strong>of</strong> <strong>Oregon</strong> Counties. Available online: http://www.aocweb.org/aoc/ (Accessed: November 30, 2007).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 35<br />
regarding Unemployment Insurance payments, resume writing, application and interview help,<br />
work skills assessment and other job-seeker assistance. 75<br />
Criminal Justice<br />
Prison populations have grown exponentially nationwide over the past two decades. On any given<br />
day, 2.2 million people are incarcerated in prison or jail across the United <strong>State</strong>s, 76 and the number<br />
<strong>of</strong> prisoners is expected to grow significantly (by nearly 200,000) over the next five years. 77<br />
Because <strong>of</strong> this extraordinary incarceration rate, as well as the disproportionate number <strong>of</strong> people <strong>of</strong><br />
color in both poverty and the prison system, programs <strong>of</strong> all types that serve low-income people<br />
(from housing, to employment, to public assistance) increasingly find people with incarceration<br />
histories among their potential clients.<br />
In addition, the link between incarceration and risk for <strong>HIV</strong>/<strong>AIDS</strong> infection is increasingly strong.<br />
In 1997, individuals released from prison or jail accounted for nearly one-quarter <strong>of</strong> all people<br />
living with <strong>HIV</strong> or <strong>AIDS</strong> in the United <strong>State</strong>s. An estimated 98,000 to 145,000 <strong>HIV</strong>-positive<br />
inmates were released from prisons and jails in 1996; almost 39,000 <strong>of</strong> these had <strong>AIDS</strong>. 78<br />
Basic Facts about Corrections in <strong>Oregon</strong><br />
• 13,516 people were incarcerated in <strong>Oregon</strong> state prisons as <strong>of</strong> June 2007, out<br />
<strong>of</strong> a total state population <strong>of</strong> 3,700,758.<br />
• The Department <strong>of</strong> Corrections budget for the 2007-09 biennium is<br />
approximately $1.3 billion. DOC estimates the cost per inmate per day at<br />
$67.53.<br />
• Although Blacks/African Americans make up less than two percent <strong>of</strong><br />
<strong>Oregon</strong>'s population, they make up ten percent <strong>of</strong> <strong>Oregon</strong>'s prison population.<br />
• As <strong>of</strong> November 2006, the three-year post-release recidivism rate (<strong>of</strong>fenders<br />
convicted <strong>of</strong> new felony crimes) was 31 percent.<br />
75 <strong>Oregon</strong> Department <strong>of</strong> Community Colleges and Workforce Development. Available online:<br />
http://www.oregon.gov/CCWD/SERVICES/index.shtml (Accessed: November 30, 2007).<br />
76 William J. Sabol, Todd D. Minton, and Paige M. Harrison. Prison and Jail Inmates at Midyear 2006. Bureau <strong>of</strong> Justice Statistics<br />
Bulletin, Washington, DC: US DOJ, Office <strong>of</strong> Justice Programs, 2007. Available online:<br />
http://www.ojp.usdoj.gov/bjs/pub/pdf/pjim06.pdf (Accessed: November 26, 2007).<br />
77 Public Safety, Public Spending: Forecasting America’s Prison Population 2007-2011. Philadelphia, PA: Pew Charitable Trusts,<br />
2007. Available online: http://www.pewpublicsafety.org/pdfs/PCT%20Public%20Safety%20Public%20Spending.pdf (Accessed:<br />
November 26, 2007).<br />
78 National Commission on Correctional Health Care, The Health Status <strong>of</strong> Soon-To-Be-Released Prisoners: A Report to Congress,<br />
Vol. 1 (Chicago: National Commission on Correction Health Care, 2002), p. 17. Available online:<br />
http://www.ncchc.org/stbr/Volume1/Chapter3.pdf (Accessed: September 17, 2007).
36 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Prisoner reentry issues are gaining more attention; however, there are still few resources available to<br />
people being released from prison and jail. Employers, landlords, subsidized housing providers,<br />
housing authorities, and even supportive housing programs <strong>of</strong>ten screen out people with criminal<br />
histories. Formerly incarcerated people may also be ineligible for public assistance, educational<br />
loans, and voting. Without employment or a place to live, successful reentry into the community is<br />
very difficult. 79<br />
Respondents to the stakeholder survey indicated that <strong>of</strong>fender transition services were an important<br />
need for the <strong>HIV</strong>/<strong>AIDS</strong> population. Half <strong>of</strong> respondents thought that reentry transition assistance<br />
was currently insufficient, and nearly half (47 percent) thought improving discharge planning from<br />
correctional facilities and hospitals was one <strong>of</strong> the highest priorities for systems integration to meet<br />
the needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong> across the state. While more than half <strong>of</strong> respondents had<br />
partnerships with criminal justice or transition services agencies, 44 percent felt that criminal justice<br />
or corrections agencies should be more involved in improving <strong>HIV</strong>/<strong>AIDS</strong> housing and service<br />
system integration.<br />
The prevalence <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> in the <strong>Oregon</strong> state prison population is estimated to be one to two<br />
percent, or approximately 225 persons; 80 additional people living with <strong>HIV</strong>/<strong>AIDS</strong> cycle through<br />
local jails. Ten percent <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong> reported having spent time in jail<br />
or prison in the past two years. 81 Surveys by both DHS and Cascade <strong>AIDS</strong> Project found that<br />
housing needs and risk for homelessness were prevalent among clients with histories <strong>of</strong><br />
incarceration.<br />
With the support <strong>of</strong> the <strong>Oregon</strong> Department <strong>of</strong> Corrections (DOC), OHOP (as the grantee) and<br />
Cascade <strong>AIDS</strong> Project (as the sponsor) successfully applied for a HOPWA Special Project <strong>of</strong><br />
National Significance (SPNS) grant in 2006, creating the <strong>Oregon</strong> <strong>State</strong>wide Supportive Community<br />
Re-entry (OSSCR) program. As described above, OSSCR will serve up to 55 post-incarcerated<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong> per year over the three-year grant period with tenant-based<br />
rental assistance, housing information, and supportive services. OHOP has leveraged funds to<br />
complement $1.3 million in HOPWA award funds for a total <strong>of</strong> $3.1 million to serve both the<br />
Portland metropolitan area and <strong>Balance</strong> <strong>of</strong> <strong>State</strong>.<br />
Since 2003, the <strong>Oregon</strong> DOC has incorporated into its Strategic Plan an “<strong>Oregon</strong> Accountability<br />
Model” to promote successful transition by prisoners to the community after release. DOC included<br />
homelessness risk / housing need in its individual intake assessments for the first time in 2007, but<br />
does not currently provide housing assistance to any individuals released from DOC custody.<br />
Among the programs that DOC has implemented or partnered to implement to improve <strong>of</strong>fender<br />
reentry is the Home for Good in <strong>Oregon</strong> (HGO) transition program, a statewide partnership with<br />
faith- and community-based organizations and community corrections agencies in which volunteers<br />
assist and mentor released prisoners. 82 Pilot programs have been implemented in Marion, Linn,<br />
79 <strong>AIDS</strong> <strong>Housing</strong> <strong>of</strong> Washington, <strong>HIV</strong>/<strong>AIDS</strong>, Incarceration, and <strong>Housing</strong>, 2003. Available online:<br />
http://www.aidshousing.org/usr_doc/Incarceration_Factsheet_2003.pdf (Accessed: September 17, 2007).<br />
80 Unpublished voluntary recruitment <strong>HIV</strong> prevalence study by Portland <strong>State</strong> University, 2005 and surveillance data from Linda<br />
Drach, MPH, Epidemiologist, Program Design & Evaluation <strong>Services</strong>, <strong>Oregon</strong> DHS, May 2006, as reported in the 2006 SPNS<br />
application.<br />
81 <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>, Program Design and Evaluation <strong>Services</strong>. We Listened…2005: Survey for People Living<br />
with <strong>HIV</strong> and <strong>AIDS</strong> in <strong>Oregon</strong>. Available online: http://www.oregon.gov/DHS/ph/hiv/services/needs/reports.shtml (Accessed:<br />
November 27, 2007).<br />
82 <strong>Oregon</strong> DOC website, Transitional <strong>Services</strong> Division. Available online:<br />
http://www.oregon.gov/DOC/TRANS/religious_services/rs_hgo_program.shtml (Accessed: November 26, 2007).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 37<br />
Douglas, and Josephine Counties, and the program has been incorporated into DOC’s 2007-09<br />
strategic plan.<br />
In 2007, <strong>Oregon</strong> established a Governor’s Reentry Council, which met for the first time in<br />
November. 83 The Council is charged with focusing attention on inmate transition to reduce<br />
recidivism, and eliminating barriers to successful reentry, including promoting access to affordable<br />
housing. Members include directors <strong>of</strong> state agencies, representatives <strong>of</strong> local public safety<br />
agencies, legislators, and others.<br />
Additional criminal justice system resources in <strong>Oregon</strong> include the advisory Criminal Justice<br />
Commission, which includes representatives <strong>of</strong> six counties and two statewide representatives, 84<br />
and local public safety coordinating councils (LPSCC), 85 established by statute in 1997. LPSCCs<br />
are intended to serve as a structure for counties to develop plans for the use <strong>of</strong> state resources to<br />
serve the local <strong>of</strong>fender population, and to help coordinate local criminal justice policy among<br />
affected criminal justice entities. An annual conference <strong>of</strong> LPSCCs was held for the first time in<br />
2005 to allow them to exchange ideas. In counties where LPSCCs are active, they seem to focus on<br />
particular issues (such as providing a methamphetamine use prevention and resource guide, in<br />
Marion County) 86 . However, these bodies may be useful venues for engaging criminal justice<br />
agencies in addressing housing or other issues among released <strong>of</strong>fenders, and for proposing specific<br />
partnerships or collaborative activities.<br />
Agencies that currently provide housing assistance to transitioning <strong>of</strong>fenders in <strong>Oregon</strong> outside <strong>of</strong><br />
the Portland metropolitan area include Sponsors ex-prisoner transitional housing and services in<br />
Lane County, 87 and the ARCHES Project <strong>of</strong> the Mid-Willamette Valley Community Action Agency<br />
in Salem. 88<br />
Sponsors provides residential transition programs for both men and women, and operates 28 units <strong>of</strong><br />
alcohol- and drug-free housing for eligible program graduates. In addition, Sponsors houses 15 sex<br />
<strong>of</strong>fenders and runs an employment assistance program to promote <strong>of</strong>fender self-sufficiency.<br />
The ARCHES Project serves as a centralized drop-in center designed to provide referral and<br />
services to homeless individuals and families. In addition to a Day Center and Transitional <strong>Housing</strong><br />
Program, ARCHES operates a HOME Tenant Based Assistance (TBA) program, serving both City<br />
<strong>of</strong> Salem and Marion County. The HOME TBA program provides ongoing rental assistance and<br />
case management for homeless and at-risk individuals and families who are actively receiving<br />
services through Parole & Probation, Marion County Home for Good, and/or Drug Court. The<br />
RENT Tenant Education Program assists individuals and families who are homeless and<br />
encountering barriers to accessing housing due to poor rental histories or poor credit.<br />
83<br />
“‘Safety, Justice and Hope,’ Values Guide Governor's New Re-Entry Council” (press release), November 21, 2007. Available<br />
online: http://www.oregon.gov/Gov/P2007/press_112107.shtml (Accessed: January 16, 2008).<br />
84<br />
Criminal Justice Commission, <strong>Oregon</strong> Governor’s website. Available online: http://www.oregon.gov/CJC/index.shtml (Accessed:<br />
January 16, 2008).<br />
85<br />
Local public safety coordinating councils, <strong>Oregon</strong> Governor’s website. Available online:<br />
http://www.oregon.gov/CJC/lpscc_page.shtml (Accessed: January 16, 2008).<br />
86<br />
Marion County Bureau <strong>of</strong> Commissioners. Available online: http://www.co.marion.or.us/BOC/PSCC/ (Accessed: January 16,<br />
2008).<br />
87<br />
Sponsors, Inc. Available online: http://www.sponsorsinc.org/ (Accessed: December 3, 2007).<br />
88<br />
Email correspondence with Carla Cary, December 17, 2007. Program information available online: www.committed.to/arches<br />
(Accessed: December 3, 2007).
Section 2: Critical Issues and<br />
Recommendations
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 41<br />
Critical Issues<br />
This section summarizes critical issues that need to be addressed to ensure integration between<br />
<strong>HIV</strong>/<strong>AIDS</strong> housing and services and other systems, as developed by the <strong>Oregon</strong> <strong>HIV</strong> <strong>Housing</strong> and<br />
Service <strong>Systems</strong> Integration Plan Steering Committee.<br />
The <strong>Oregon</strong> <strong>HIV</strong> <strong>Housing</strong> and Service <strong>Systems</strong> Integration Plan Steering Committee met in Salem,<br />
<strong>Oregon</strong>, on December 18, 2007, to review findings from the assessment <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> resources and<br />
systems integration conducted by Building Changes during the second half <strong>of</strong> 2007. Based on these<br />
findings, the Committee identified critical issues in systems integration that pose challenges to<br />
meeting the housing and related needs <strong>of</strong> people living with <strong>HIV</strong> and <strong>AIDS</strong> in the state <strong>of</strong> <strong>Oregon</strong><br />
(outside <strong>of</strong> the Portland Metropolitan Area).<br />
The Committee identified both general issues related to the outreach and partnership strategies <strong>of</strong><br />
the <strong>Oregon</strong> <strong>Housing</strong> Opportunities in Partnership (OHOP) program, and issues specific to the<br />
various housing and service systems which should be involved in an integrated <strong>HIV</strong> housing and<br />
service plan for <strong>Oregon</strong> residents. These issues are described below and divided into two categories:<br />
Outreach and Partnership Development, and Integration with <strong>Housing</strong> and Service <strong>Systems</strong>.<br />
Outreach and Partnership Development<br />
1. Limited Awareness <strong>of</strong> Resources Dedicated to People Living with <strong>HIV</strong>/<strong>AIDS</strong><br />
Steering Committee members noted that many mainstream housing and services partners, all<br />
potential OHOP partners, lack awareness or accurate knowledge <strong>of</strong> the OHOP program. This lack<br />
<strong>of</strong> awareness <strong>of</strong> existing <strong>HIV</strong>/<strong>AIDS</strong> resources likely extends to the greater community, including<br />
among faith- and other community-based organizations, and may limit partnerships in several ways.<br />
Potential housing partners may not be familiar with the <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong>,<br />
Public Health, <strong>HIV</strong>/STD/TB Section, <strong>HIV</strong> Care and Treatment program, and thus might not<br />
recognize the availability <strong>of</strong> service match dollars or other partnership opportunities. For instance,<br />
providers may have misconceptions about the flexibility <strong>of</strong> DHS <strong>HIV</strong> Care and Treatment dollars to<br />
leverage housing funds. Because services administered by <strong>HIV</strong> Care and Treatment are supported<br />
by a blend <strong>of</strong> state, federal, and revenue funds, they can be used as a service match for federal<br />
housing programs such as HOME Tenant-Based Assistance, unlike federal Ryan White funding<br />
alone.<br />
In addition, some agencies use limited resources when those services could be covered by a<br />
dedicated funding stream for clients with an <strong>HIV</strong> diagnosis. For example, both the OHOP program<br />
and Community Action Agencies (CAAs) <strong>of</strong>fer emergency utility assistance. CAAs that do not<br />
have or share information about OHOP with their clients may end up spending out their utility<br />
assistance funds on OHOP-eligible clients, while OHOP funds remain underutilized.<br />
In addition, some government departments and agencies that are unfamiliar with OHOP and the<br />
<strong>HIV</strong> Care and Treatment Program do not keep OHOP staff and <strong>HIV</strong> Care and Treatment Program
42 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
case managers updated on planning processes (including opportunities for community input on<br />
Continuum <strong>of</strong> Care, Consolidated Plan, and other processes and applications) or inform them <strong>of</strong><br />
resource availability or collaborative opportunities. This limits the opportunities that <strong>HIV</strong>/<strong>AIDS</strong><br />
housing and services stakeholders have to help shape inclusive plans, and thus limits the degree to<br />
which people living with <strong>HIV</strong>/<strong>AIDS</strong> are included in mainstream housing and other services.<br />
Detailed information about the OHOP and <strong>HIV</strong> Care and Treatment programs is or will be available<br />
in the form <strong>of</strong> reports and publications such as this Plan, but not all potential partners are likely to<br />
seek out or read lengthy documents on these topics.<br />
2. Confidentiality Concerns<br />
The need to maintain client confidentiality restricts the ways that OHOP housing coordinators and<br />
other organizations and individuals can conduct outreach about their activities and resources. For<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong>, stigma and discrimination are significant factors in finding and<br />
maintaining housing, accessing support services, and seeking medical care. People living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> <strong>of</strong>ten struggle with keeping their <strong>HIV</strong> status private, particularly from landlords and<br />
neighbors. For this reason, OHOP staff and partners market their services quietly to avoid<br />
disclosing to landlords and other providers that HOPWA is the source <strong>of</strong> housing assistance for<br />
clients they place, or that clients qualify for OHOP via an <strong>HIV</strong> diagnosis. The need to maintain<br />
privacy around <strong>HIV</strong>/<strong>AIDS</strong>-related services and programs such as OHOP can limit opportunities for<br />
collaboration, outreach, and landlord education.<br />
Moreover, CAAs and other community-based providers that would like to be able to make referrals<br />
to the OHOP program do not necessarily know which <strong>of</strong> their clients are living with <strong>HIV</strong>/<strong>AIDS</strong>, or<br />
how to ask for or provide information in a way that allows those individuals to maintain privacy.<br />
3. Limited Staff Capacity<br />
OHOP and <strong>HIV</strong> Care and Treatment staff have limited resources and time to conduct marketing and<br />
outreach to mainstream housing and service providers, in addition to serving individual clients or<br />
coordinating specific housing activities. In addition, these staff may lack familiarity with aspects <strong>of</strong><br />
partner systems, including affordable housing, and have limited training to expand this knowledge.<br />
Integration with <strong>Housing</strong> and Service <strong>Systems</strong><br />
Affordable <strong>Housing</strong> Resources<br />
Coordination and partnerships with affordable housing developers and providers (including housing<br />
authorities) and affordable housing planning processes (such as the Consolidated Plan or Low<br />
Income <strong>Housing</strong> Tax Credit processes) can lead to the development or dedication <strong>of</strong> new housing<br />
resources, targeted either for people with disabilities in general or specifically for people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong>. Good communication can also lead affordable housing providers to prioritize existing<br />
resources for people living with <strong>HIV</strong>/<strong>AIDS</strong>, whether because <strong>of</strong> an increased perception <strong>of</strong> this<br />
population’s housing need or recognition <strong>of</strong> the resources that can be leveraged to serve them.<br />
4. Prioritizing Participation Among Many Planning and Implementation Processes<br />
Mechanisms for community input are frequently built in to affordable housing planning processes,<br />
but it can be difficult for OHOP staff and partners to track the time-limited opportunities to provide
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 43<br />
such input, as well as to prioritize in which meetings and processes their participation will be most<br />
effective and conducive to meeting OHOP goals.<br />
As part <strong>of</strong> this decision-making, OHOP staff and partners must differentiate among the many<br />
different stages <strong>of</strong> the affordable housing finance or development processes at different levels <strong>of</strong><br />
government. OHOP administrators must also determine the best use <strong>of</strong> limited OHOP resources,<br />
whether as part <strong>of</strong> development projects that create a long-term resource to benefit people living<br />
with <strong>HIV</strong>/<strong>AIDS</strong>, or in less resource-intense housing subsidies that depend on the availability <strong>of</strong><br />
existing stock for which OHOP clients compete with other low-income populations.<br />
OHOP administrators and partners must also consider how to direct resources into relationshipbuilding<br />
among different kinds <strong>of</strong> potential partners. Stakeholders in the development <strong>of</strong> this Plan<br />
identified landlords as a particularly critical group. In both planning and day-to-day work, staff<br />
must weigh the advantages <strong>of</strong> focusing on maintaining and expanding existing relationships or<br />
seeking to create new partnerships. On the administrator level, the competing interests among<br />
regions and between city-centered and rurally dispersed affordable housing planning and<br />
implementation processes must also be considered.<br />
5. Maximizing Access to New Resources for Special Populations<br />
As new resources become available within <strong>Oregon</strong> for populations that may include people living<br />
with <strong>HIV</strong>/<strong>AIDS</strong>, OHOP staff and partners must determine where overlap is significant and how to<br />
allocate resources for developing proposals and applications to leverage these funding streams. For<br />
example, OHOP could consider partnering to apply for some portion <strong>of</strong> the approximately $4<br />
million in <strong>Housing</strong> PLUS funds that will be available through the Spring 2008 Consolidated<br />
Funding Cycle.<br />
Steering Committee members noted that affordable housing funders and developers are asked to<br />
prioritize or include a variety <strong>of</strong> special population definitions and set-asides in their projects or<br />
guidelines. Affordable housing resources are limited across the balance <strong>of</strong> state, resulting in strong<br />
competition for funding opportunities, and some competitions <strong>of</strong>fer “bonus points” to applications<br />
for projects serving various special populations. While these special population priorities vary, both<br />
funders and developers value partners that can bring new resources into projects, such as through<br />
service matches or rental subsidies.<br />
6. Understanding Affordable <strong>Housing</strong> System Missions and Cultures<br />
Stakeholders in the affordable housing system have interests and goals that vary from entity to<br />
entity and may not be clear to OHOP stakeholders or consistent with OHOP goals. For example,<br />
Steering Committee members pointed out that affordable housing developers generally seek to<br />
balance high-need tenants with more independent low-income tenants in any housing complex,<br />
feeling that such a mix is needed to promote a sustainable community. This goal <strong>of</strong> balancing levels<br />
<strong>of</strong> service need may or may not be consistent with admitting particular proportions <strong>of</strong> people living<br />
with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
Homeless <strong>Services</strong><br />
<strong>Oregon</strong>, in step with numerous state and local jurisdictions nationally, has focused resources and<br />
developed infrastructure to address the needs <strong>of</strong> people who are homeless, both through the HUD<br />
Continuum <strong>of</strong> Care process and more recently through state and local 10-Year Plans to End
44 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Homelessness. However, the <strong>HIV</strong>/<strong>AIDS</strong> housing and services and homelessness systems are not<br />
well-coordinated.<br />
7. Lack <strong>of</strong> Shared Data and Coordinated Planning Between <strong>HIV</strong>/<strong>AIDS</strong> and Homeless<br />
<strong>Systems</strong><br />
Limited data is available on the overlap between the challenges <strong>of</strong> homelessness and <strong>HIV</strong>/<strong>AIDS</strong> in<br />
<strong>Oregon</strong>, and few <strong>HIV</strong>/<strong>AIDS</strong> agencies participate in homeless services or housing planning<br />
processes. Although research shows a strong correlation between <strong>HIV</strong> and housing instability, and<br />
HOPWA has recently required grantees to track homelessness among clients, information systems<br />
are not yet well integrated on the client or systems levels. This makes it difficult for OHOP to<br />
compare data from its epidemiological and programmatic sources against services being used<br />
through homeless services providers. Better data integration would allow OHOP to better document<br />
its resource leveraging and help prevent duplication <strong>of</strong> services for clients served by multiple<br />
systems, and could also prevent some clients from falling through the cracks and not receiving<br />
referrals for needed services.<br />
<strong>Oregon</strong> <strong>Housing</strong> and Community <strong>Services</strong> (OHCS) uses a customized Homeless Management<br />
Information System (HMIS) called OPUS to collect data for its homelessness services and Low<br />
Income Energy Assistance Programs (LIEAP) in the balance <strong>of</strong> state. The OHOP program has not<br />
historically used an HMIS program, but is planning to begin using ServicePoint, the HMIS system<br />
used in the Portland area. Since OHOP does administer an allocation <strong>of</strong> state LIEAP funds, staff are<br />
able to access OPUS for the limited purposes <strong>of</strong> that program, although there is limited funding to<br />
expand OHOP’s use <strong>of</strong> and integration with OPUS at this time.<br />
8. Incomplete Integration <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> Issues into Continua <strong>of</strong> Care<br />
Steering Committee members identified the need to provide better information about people living<br />
with <strong>HIV</strong>/<strong>AIDS</strong> for the sections <strong>of</strong> Continuum <strong>of</strong> Care applications that address subpopulations.<br />
The inclusion <strong>of</strong> this population in Continuum <strong>of</strong> Care planning should also be more meaningful,<br />
and include participation in meetings.<br />
The underutilization <strong>of</strong> Shelter Plus Care (S+C) was another issue noted by the Steering Committee.<br />
There is currently only one Shelter Plus Care project in <strong>Oregon</strong>’s balance <strong>of</strong> state, in the<br />
Eugene/Springfield/Lane County Continuum <strong>of</strong> Care. Some Continua <strong>of</strong> Care in <strong>Oregon</strong> are<br />
reluctant to apply for “bonus” projects (such as S+C projects) beyond pro-rata need, because <strong>of</strong> the<br />
potential burden on sponsor agencies <strong>of</strong> administrative costs and service match requirements. Those<br />
concerns must be addressed in order to ensure that <strong>Oregon</strong>’s communities leverage the maximum <strong>of</strong><br />
Continuum <strong>of</strong> Care funding opportunities. For example, the project in Lane County previously<br />
accepted client referrals from only one provider, but recently has begun working with OHOP to take<br />
referrals to fill unused program slots.<br />
Addictions and Mental Health<br />
9. Addictions and Mental Health <strong>Services</strong> Gap<br />
The Steering Committee saw a significant gap in services for addictions and mental health services<br />
among people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong>’s balance <strong>of</strong> state. <strong>Oregon</strong>’s new competitive<br />
HOPWA Special Project <strong>of</strong> National Significance (SPNS) grant (the <strong>Oregon</strong> <strong>Housing</strong> and<br />
Behavioral Health Initiative, or OHBHI) was recognized as an important source <strong>of</strong> support for<br />
services and an effort to better integrate <strong>HIV</strong>/<strong>AIDS</strong> housing and services with behavioral health
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 45<br />
care. But the OHBHI award will not eliminate the gap, and applies only to clients in the I-5<br />
corridor.<br />
10. Limited Access by People Living with <strong>HIV</strong>/<strong>AIDS</strong> to Mainstream Behavioral Health<br />
<strong>Services</strong><br />
Steering Committee members noted the availability <strong>of</strong> limited statewide housing development funds<br />
to serve people with behavioral health issues and unmet housing needs: Community Mental Health<br />
<strong>Housing</strong>, Alcohol and Drug Free <strong>Housing</strong>, and the new Expanding Community Living<br />
Opportunities fund. Demand for these funds exceeds availability, and to date they have not<br />
supported developments with units dedicated to people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
On an individual client level, OHOP housing coordinators and partners have also had trouble<br />
accessing the network <strong>of</strong> mental illness respite beds across the state. Qualification criteria can be<br />
strict, and there are limited points <strong>of</strong> referral such as mental health departments.<br />
Human <strong>Services</strong> and Public Assistance<br />
Many people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong> have an array <strong>of</strong> basic needs that are common to<br />
low-income people in general. These can include family support, transportation, food and<br />
nutritional assistance, hygiene, and general financial needs. Awareness and understanding <strong>of</strong> the<br />
service needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong> tend to be limited among the many government and<br />
nonpr<strong>of</strong>it agencies that provide general human services throughout the balance <strong>of</strong> state. Stigma<br />
based on misconceptions and generalizations about <strong>HIV</strong> disease and people who are living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> can be a barrier to fair and compassionate service delivery.<br />
11. Loss and Scarcity <strong>of</strong> Funding for Human <strong>Services</strong><br />
Nationwide, human services tend to be locally funded – and usually underfunded, especially in<br />
smaller, more rural counties. In some areas <strong>of</strong> <strong>Oregon</strong>, the loss <strong>of</strong> timber revenues upon which such<br />
counties have relied for many years has compounded with an aging population and loss <strong>of</strong> young<br />
people to the cities, dealing major blows to the budgets <strong>of</strong> human service agencies. The small<br />
number <strong>of</strong> “one-stop” centers in which multiple agencies coordinate their services to wrap around<br />
client households has dwindled, making the services that remain harder to access.<br />
12. Family Support Needs<br />
OHOP serves a substantial number <strong>of</strong> family households (as compared to individuals); this<br />
proportion varies by region, with more families receiving housing help in Eugene, for example, than<br />
in Salem. Families typically need larger housing units, <strong>of</strong> which the supply may be limited. Also,<br />
different family members may require different kinds <strong>of</strong> services, thereby increasing the number <strong>of</strong><br />
systems with which a household is involved and the complexity <strong>of</strong> meeting their needs. Some types<br />
<strong>of</strong> housing and services options funded for people living with <strong>HIV</strong>/<strong>AIDS</strong> may be more or less<br />
appropriate to family groups.<br />
Criminal Justice<br />
A large percentage <strong>of</strong> new <strong>HIV</strong> diagnoses in <strong>Oregon</strong> are among people who have served time in<br />
jails or prisons. Research also shows that people with histories <strong>of</strong> incarceration are much more<br />
likely to have <strong>HIV</strong>/<strong>AIDS</strong> than the general population. Members <strong>of</strong> the Steering Committee lauded<br />
the <strong>Oregon</strong> <strong>State</strong>wide Supportive Community Reentry (OSSCR) funding, a HOPWA competitive
46 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
grant targeted to serve 55 individuals released from incarceration, through a coordinated effort <strong>of</strong><br />
OHOP, the Department <strong>of</strong> Corrections, and an array <strong>of</strong> other partners.<br />
13. Lack <strong>of</strong> <strong>Housing</strong> Options<br />
Offenders living with <strong>HIV</strong>/<strong>AIDS</strong> face challenges related to their criminal histories as well as their<br />
health diagnoses. They are screened out <strong>of</strong> public and private housing by background checks, and<br />
can find it difficult to transition to mainstream housing assistance programs such as Section 8 from<br />
the OHOP program.<br />
14. Multiple Risk Factors<br />
Poverty, credit problems, substance abuse and mental illness are common among prison inmates,<br />
and may be magnified by their chronic health condition(s). Debts both related and unrelated to<br />
convictions climb while a person is incarcerated and in treatment, which may be required by the<br />
justice system. <strong>Housing</strong> and family situations are disrupted and may be difficult or impossible to reestablish.<br />
Such risk factors translate into high service needs – and gaps in receiving services – when<br />
prisoners return to the community.<br />
Primary Care, Hospitals and Assisted Living<br />
15. Lack <strong>of</strong> Research and Resources for People Living with <strong>HIV</strong>/<strong>AIDS</strong><br />
Steering Committee members identified a need for more assisted living and long-term care options<br />
(including in-home assistance) for people living longer with <strong>HIV</strong>, and those suffering from chronic<br />
diseases like diabetes, which provider observation suggests emerge earlier and more frequently<br />
among people with <strong>HIV</strong> than in the general population. The lack <strong>of</strong> research in the arena <strong>of</strong> chronic<br />
diseases among people living with <strong>HIV</strong>/<strong>AIDS</strong> limits the care a patient has access to. For example,<br />
when screening or preventative measures exist, insurance may not fund those measures for people<br />
with <strong>AIDS</strong> if they lack other risk factors.<br />
16. Additional <strong>Housing</strong> Challenges<br />
Holding housing units and maintaining housing assistance as people cycle in and out <strong>of</strong> assisted<br />
living situations can be difficult, and can require modifications to rules and incur additional<br />
administrative costs. People with chronic diseases may need additional accommodations within<br />
their living units, or may need to live closer to health providers, limiting their ability to move or<br />
choose among housing options. Moreover, traditional assisted-living environments for elderly<br />
people may not be a good fit for younger (middle-aged) people living with <strong>HIV</strong>/<strong>AIDS</strong>. The<br />
difficulty <strong>of</strong> placing clients in assisted living is broader than the <strong>HIV</strong>/<strong>AIDS</strong> population but is a<br />
challenge statewide.<br />
Employment<br />
17. Limited Coordination Among Employment, Service, and <strong>Housing</strong> <strong>Systems</strong><br />
Additional coordination and improved awareness <strong>of</strong> service needs and available resources are<br />
needed between <strong>AIDS</strong> and employment service systems. Typically, employment centers (such as<br />
One Stop Centers established under the federal Workforce Investment Act) are evaluated based on<br />
number <strong>of</strong> successful job placements and similar measures. This may discourage them from serving<br />
clients with the multiple challenges that people living with <strong>HIV</strong>/<strong>AIDS</strong> may have (including gaps in
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 47<br />
work history or absences from work due to health issues), and from providing the ongoing<br />
employment support that they need to retain these jobs.<br />
Differences in agency missions and cultures among the systems as pertains to employment can<br />
contribute to poor coordination. Health, human services, and homelessness services providers may<br />
not prioritize work and self-sufficiency as much as mainstream affordable housing providers<br />
typically do, adding complexity to partnerships among these systems.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 49<br />
Recommendations<br />
Recommendations and action steps for addressing the critical issues identified during this needs<br />
assessment and planning process are presented in this section <strong>of</strong> the plan.<br />
The <strong>Oregon</strong> <strong>HIV</strong> <strong>Housing</strong> and Service <strong>Systems</strong> Integration Plan Steering Committee met in Salem,<br />
<strong>Oregon</strong>, on December 18, 2007, and then convened by telephone conference on January 24, 2008,<br />
to develop strategic recommendations to address the critical issues identified at the December 18<br />
meeting and described in the previous section.<br />
As noted in the previous section, the Steering Committee considered issues related to the outreach<br />
and partnership strategies <strong>of</strong> the OHOP program, as well as issues specific to the relevant housing<br />
and service systems. The recommendations described below are divided into the same two<br />
categories, with some recommendations broken down further into possible action steps identified by<br />
the Steering Committee.<br />
Outreach and Partnership Development<br />
1. Develop simple, discreet material to publicize OHOP and related services and<br />
opportunities, and disseminate widely.<br />
Provide posters, brochures, and other materials to community action agencies, local DHS <strong>of</strong>fices,<br />
mainstream housing providers, faith- and other community-based organizations, and homeless<br />
shelters and drop-in centers. Develop or adapt a brochure that describes OHOP as a housing<br />
assistance program, includes eligibility parameters inside the brochure, provides contact<br />
information for housing coordinators, and assures that contact with the housing coordinator will be<br />
kept confidential.<br />
Action steps may include:<br />
• Develop a simple website showcasing the systems integration plan and affordable housing<br />
resource guide for housing and service partners to link to.<br />
• Seek opportunities to include information on OHOP services on materials and applications<br />
for assistance programs administered by community action agencies and other social service<br />
providers.<br />
• Post the affordable housing resource guide created for this Plan (Appendix 1) online, with<br />
separate pages (that can be easily linked to) for each region and topic. Link this information<br />
with the existing <strong>Oregon</strong> <strong>AIDS</strong> Hotline website. Update the resource guide regularly.<br />
2. Present to current and potential partners with information tailored to their interests.<br />
Continue to seek the support and engagement <strong>of</strong> potential stakeholders and partners, such as local<br />
governments and regional housing, homeless services, faith-based and community-based grass roots<br />
organizations, and <strong>HIV</strong>/<strong>AIDS</strong> advocacy groups. Presentations to affordable housing developers and<br />
funders should provide general background on <strong>HIV</strong>/<strong>AIDS</strong> housing and services need, but then focus
50 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
on the availability <strong>of</strong> service matches through <strong>HIV</strong> Care and Treatment services, and rent subsidies<br />
through OHOP.<br />
Action steps may include:<br />
• Take advantage <strong>of</strong> events in which Steering Committee members are involved in planning,<br />
such as the <strong>Oregon</strong> <strong>Housing</strong> and Homeless Conference (April 11, 2008).<br />
• Briefly summarize the detailed information available about the needs <strong>of</strong> and resources for<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong> (such as this Plan), and focus on aspects <strong>of</strong> OHOP<br />
and <strong>HIV</strong> Care and Treatment and their clients that are most relevant to the particular agency<br />
or audience being targeted. To the extent possible, present locally specific information about<br />
<strong>HIV</strong>/<strong>AIDS</strong> and housing needs in each jurisdiction.<br />
• Tailor outreach efforts for critical audiences, with specific goals or strategies highlighted. For<br />
example, information on the cost-savings <strong>of</strong> providing housing to people with <strong>HIV</strong>/<strong>AIDS</strong> in<br />
each region can help persuade local government <strong>of</strong>ficials to allocate funding from human<br />
service budgets to meet these needs, or to prioritize them in Consolidated Plans.<br />
3. Engage provider agency staff, clients, and other regional participants in publicizing the<br />
need, opportunity, and benefits <strong>of</strong> investing in housing and services for people living<br />
with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
Work with local stakeholders to build their capacity to foster support and monitor progress in their<br />
jurisdictions. Stakeholders may include <strong>HIV</strong>/<strong>AIDS</strong> service agencies, <strong>HIV</strong> <strong>Housing</strong> Task Force<br />
members, <strong>HIV</strong> Care case managers, consumer representatives, and other partners across the state.<br />
Action steps may include:<br />
• Use the calendar <strong>of</strong> local funding and planning processes in the affordable housing resource<br />
guide (Appendix 1) to guide timely outreach efforts, such as participation or presentation at<br />
public meetings.<br />
• Create “talking points” for regional partners to guide presentations that advocate for focusing<br />
local resources on the housing needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
• If staff capacity is insufficient for this range <strong>of</strong> activities, OHOP could choose to direct<br />
technical assistance funds to contract with a consultant, or seek a university partner, to design<br />
and coordinate a proactive outreach plan.<br />
4. Offer trainings and create forums for sharing best practices to build OHOP and<br />
partner staff capacity.<br />
Provide staff with opportunities to build knowledge and share successful program strategies, and<br />
elicit engagement and guidance from a diverse oversight body.<br />
Action steps may include:<br />
• Convene monthly or bi-monthly meetings via phone conference for OHOP housing<br />
coordinators and Ryan White case managers to collaborate on case problem-solving and<br />
discuss resources for clients. Empower OHOP housing coordinators to seek assistance as<br />
needed directly from HOPWA technical assistance providers (Building Changes staff) for<br />
HOPWA program questions.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 51<br />
• Resume regular meetings (likely twice per year) <strong>of</strong> the <strong>HIV</strong> <strong>Housing</strong> Task Force that guided<br />
the development <strong>of</strong> the OHOP program. The membership <strong>of</strong> this Task Force should include<br />
OHOP staff, other <strong>HIV</strong>/<strong>AIDS</strong> service agencies, and affordable housing providers across the<br />
state. The Task Force should promote the dissemination and implementation <strong>of</strong> this Plan. In<br />
addition, members <strong>of</strong> the Task Force can help diffuse some <strong>of</strong> the workload <strong>of</strong> Plan<br />
implementation by building connections with regional partners and attending meetings such<br />
as the Continuum <strong>of</strong> Care.<br />
• Convene <strong>HIV</strong> Care and Treatment case managers and OHOP housing coordinators for an<br />
annual retreat to review program changes, successes and challenges; discuss roles; identify<br />
ways to improve coordination; and set goals for optimal client case management.<br />
• To ensure housing discrimination issues and related concerns are addressed and resolved,<br />
continue working with the Fair <strong>Housing</strong> Council <strong>of</strong> <strong>Oregon</strong> to educate staff and partners and<br />
to coordinate appropriate strategies for addressing resistant parties.<br />
Integration with <strong>Housing</strong> and Service <strong>Systems</strong><br />
Affordable <strong>Housing</strong> Resources<br />
5. Participate consistently in the statewide Consolidated Plan, Continuum <strong>of</strong> Care, and<br />
other planning processes.<br />
Participate in state and local Consolidated Plan (“Con Plan”) and Continuum <strong>of</strong> Care planning<br />
processes to ensure that the needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong> are recognized and addressed.<br />
Reach out to planning representatives to ensure that OHOP staff receive regular updates and<br />
meeting announcements.<br />
Action steps may include:<br />
• OHOP staff should provide information on the housing needs <strong>of</strong> people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> to local governments as they develop their five-year Con Plans, especially in cities<br />
that have previously identified people living with <strong>HIV</strong>/<strong>AIDS</strong> as a “low” priority for housing<br />
resources.<br />
• Ensure that each Continuum <strong>of</strong> Care in the balance <strong>of</strong> state has information and expertise<br />
available on the local needs <strong>of</strong> homeless people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
• Such participation requires a public planning environment that is supportive to local input.<br />
Approach agencies who regularly participate in advocacy efforts, such as the <strong>HIV</strong> Alliance in<br />
Lane County, to benefit from their guidance and suggestions.<br />
• Join with broader advocates for people with disabilities to encourage scoring incentives for<br />
projects serving special needs populations through the Consolidated Funding Cycle, Qualified<br />
Allocation Plan (QAP), and other funding sources.<br />
6. Prioritize strategically between building on existing relationships or seeking new<br />
partnerships with affordable housing developers and providers.<br />
Reach out to pr<strong>of</strong>essional associations, including the Association <strong>of</strong> <strong>Oregon</strong> Community<br />
Development Organizations / Community Development Network, to disseminate information<br />
among their members and to identify both areas <strong>of</strong> interest to them and potential partners, including
52 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
service providers, advocacy groups, and community- and faith-based organizations. Select a few<br />
agencies that are either receptive to partnership, represent significant resources in areas <strong>of</strong> need, or<br />
both to develop and pitch specific potential joint ventures. Successful early partnerships with<br />
housing providers can serve as examples for future collaborations in other regions <strong>of</strong> the state.<br />
7. Seek housing development opportunities in which relatively modest <strong>HIV</strong>/<strong>AIDS</strong>-specific<br />
resources can leverage significant investment from other sources.<br />
Steering Committee members underscored that even modest commitments <strong>of</strong> funding for operating<br />
costs and supportive services in affordable housing development applications can be persuasive to<br />
government funders. For example, in one case, just $35,000 allocated by the Division <strong>of</strong> Addictions<br />
and Mental Health for housing development has leveraged $1.5M in <strong>Oregon</strong> <strong>Housing</strong> and<br />
Community <strong>Services</strong> (OHCS) funds.<br />
Given the limited resources available for <strong>HIV</strong> Care and Treatment and OHOP, focus development<br />
or rehabilitation partnerships on units integrated into buildings (rather than stand-alone units).<br />
Promote set-asides for tenants living with <strong>HIV</strong>/<strong>AIDS</strong> who already receive case management and<br />
services, and thus are unlikely to create challenges or administrative costs for property managers.<br />
Homeless <strong>Services</strong><br />
8. Focus attention on improving coordination with planning, data, and other elements <strong>of</strong><br />
homeless systems.<br />
Connect with, and track the activities <strong>of</strong>, the state Ending Homelessness Advisory Council (EHAC).<br />
Participate regularly in Continuum <strong>of</strong> Care and state and local 10-Year Plan processes, using<br />
strategies described in the previous sections. Seek integration <strong>of</strong> data at the client level by linking<br />
information systems across mental health, <strong>HIV</strong> care, and homeless services, including partnering<br />
with OHCS to compare OHOP and <strong>HIV</strong>/<strong>AIDS</strong> epidemiology data with homeless services<br />
information.<br />
9. Promote Shelter Plus Care and other bonus projects through agreements to streamline<br />
or share sponsor administrative costs.<br />
Seek to allay the concerns <strong>of</strong> Continuum <strong>of</strong> Care partners and potential sponsors <strong>of</strong> “bonus” projects<br />
for serving chronically homeless people through coordinated planning to share administrative<br />
responsibilities. OHOP cannot allocate additional overhead above the administrative percentage<br />
allowed by its grants, but coordination between OHOP staff and partners may create efficiencies. If<br />
successful, initial partnering with existing Shelter Plus Care (S+C) providers can enhance and<br />
demonstrate the capacity <strong>of</strong> OHOP staff to seek additional S+C projects with new partners.<br />
10. Conduct outreach and seek partnerships with landlords and property managers.<br />
Link with regional housing centers that conduct fair housing and other trainings for landlords and<br />
potential landlords (including faith-based organizations), to promote the inclusion <strong>of</strong> information on<br />
the housing challenges and resources available to people living with <strong>HIV</strong>/<strong>AIDS</strong>. Effectively use<br />
existing tenant certification programs, such as St. Vincent de Paul’s Second Chance renter<br />
rehabilitation program, that connect landlords to tenants who have completed certification. Explore<br />
opportunities to create or participate in a landlord risk mitigation fund for clients who have histories<br />
<strong>of</strong> homelessness or other risk factors.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 53<br />
Addictions and Mental Health<br />
11. Partner with substance abuse and mental health service providers to spotlight need<br />
and seek expanded support for these services.<br />
Capitalize on existing and new opportunities, such as the Expanding Community Living<br />
Opportunities, Community Mental Health <strong>Housing</strong> Fund, and Alcohol and Drug Free <strong>Housing</strong> Fund<br />
programs, to maximize the availability <strong>of</strong> resources to people affected by both <strong>HIV</strong>/<strong>AIDS</strong> and<br />
behavioral health issues.<br />
Make targeted presentations to Local Alcohol and Drug Planning Committees, which are appointed<br />
by county commissioners to identify needs and establish priorities for alcohol and other drug<br />
services in the county. 89<br />
Join efforts to advocate for increased state and local prioritization and funding for mental health and<br />
substance abuse services, as an important component in supporting client health and housing<br />
stability.<br />
When appropriate, encourage community- and faith-based organizations to provide, and seek to<br />
connect clients with, addiction counseling, peer networking, and other social support structures to<br />
address substance abuse issues.<br />
12. Build relationships with behavioral health crisis providers.<br />
Identify and pursue ways to access limited treatment beds for clients with behavioral health crises,<br />
including partnerships with mental health departments to refer OHOP clients to crisis beds. Support<br />
efforts to increase the number <strong>of</strong> crisis beds and to streamline access to them.<br />
Human <strong>Services</strong> and Public Assistance<br />
13. Prioritize education and outreach to local DHS <strong>of</strong>fices and community action agencies<br />
around <strong>HIV</strong>/<strong>AIDS</strong> and client issues, and support coordinated service delivery models.<br />
The Steering Committee advised that in the human services sector, outreach to relatively<br />
independent local <strong>of</strong>fices can be more valuable than outreach at the state level. Address<br />
coordination issues that can emerge in the delivery <strong>of</strong> services, rather than in policy, with these<br />
<strong>of</strong>fices. Fortify relationships with “one-stop” centers, such as the Rogue Valley Family Center, that<br />
provide evidence-based models <strong>of</strong> co-located services and assistance, and foster the replication <strong>of</strong><br />
this model when possible.<br />
Criminal Justice<br />
14. Pursue partnerships with local and state criminal justice agencies and stakeholders,<br />
and seek federal and other resources to serve people with incarceration histories.<br />
Expand on the success <strong>of</strong> the <strong>Oregon</strong> <strong>State</strong>wide Supportive Community Reentry initiative, and<br />
continue building relationships with Department <strong>of</strong> Corrections as well as with local criminal justice<br />
agencies.<br />
89 Contact information for local committees is available online at: http://www.oregon.gov/OHCS/HRS_ADF_Program.shtml<br />
(Accessed: January 25, 2008).
54 <strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Action steps may include:<br />
• Conduct outreach to agencies that serve people released from prison and jail in <strong>Oregon</strong>, such<br />
as Sponsors and Mid-Willamette Valley Community Action Agency, and provide materials<br />
and education around <strong>HIV</strong>/<strong>AIDS</strong> and the HOPWA program to staff and clients.<br />
• Work with landlords (such as those in high vacancy areas) as well as community- and faithbased<br />
organizations who are willing to consider tenants with criminal histories, and help to<br />
build bridges between these landlords and community corrections <strong>of</strong>ficers and service<br />
providers.<br />
• Consider master leasing (an eligible HOPWA program activity) as a strategy to provide<br />
housing for clients who face the highest barriers to obtaining private market housing.<br />
• Connect with the Governor’s Reentry Task Force, whose members were announced in<br />
November 2007.<br />
• Explore opportunities to access federal and private resources to support the safe and<br />
successful transition <strong>of</strong> prisoners (including those with <strong>HIV</strong>/<strong>AIDS</strong>) to the community, such as<br />
the U.S. Department <strong>of</strong> Justice’s Prisoner Reentry Initiative. 90<br />
Primary Care, Hospitals and Assisted Living<br />
15. Anticipate that clients may need periodic or long-term care in assisted living situations<br />
while setting OHOP policies and allocating resources.<br />
Strategize ways to ensure that housing assistance can continue if clients must move temporarily or<br />
permanently into assisted living situations, including planning to make transitions smooth.<br />
Incorporate information on this emerging challenge in OHOP and <strong>HIV</strong> Care and Treatment staff<br />
trainings and discussion. Consider ways to provide services to clients in their own homes when<br />
appropriate, as an alternative to long-term hospitalizations.<br />
16. Conduct outreach about emerging primary care and assisted living needs <strong>of</strong> people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong>, including to providers <strong>of</strong> these services.<br />
Connect with the <strong>Oregon</strong> Health Care Association to raise awareness among members about the<br />
changing needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong> and co-occurring chronic diseases. Seek improved<br />
connections to and partnerships with hospitals and health care providers, including assisted-living<br />
providers, to promote the successful integration <strong>of</strong> people with <strong>HIV</strong>/<strong>AIDS</strong> into their services and<br />
seamless transitions from one setting to another. Ensure that health department and other outreach<br />
workers are educated and kept up to date on OHOP resources, program activities, and policies.<br />
Advocate to increase the availability <strong>of</strong> a continuum assisted living supports, using the challenges <strong>of</strong><br />
people living with <strong>HIV</strong>/<strong>AIDS</strong> in gaining access to such supports to illustrate the need.<br />
Employment<br />
17. Collaborate with workforce systems to provide employment supports and training for<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
90 Available online: http://www.ojp.usdoj.gov/BJA/grant/reentry.html (Accessed: February 1, 2008).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan 55<br />
Seek connections with Workforce Training One-Stop Centers: OHOP housing coordinators or <strong>HIV</strong><br />
Care and Treatment case managers could meet with staff there, familiarize themselves with services<br />
<strong>of</strong>fered, and <strong>of</strong>fer to work collaboratively to support people with <strong>HIV</strong>. Additionally, identify<br />
agencies that provide life skills and benefits trainings for case managers and staff that focus on<br />
going back to work, and participate in these trainings. Encourage community- and faith-based<br />
partners to eliminate barriers to employment that are correlated with <strong>HIV</strong>/<strong>AIDS</strong> risk (such as<br />
histories <strong>of</strong> incarceration) and to hire people living with <strong>HIV</strong>/<strong>AIDS</strong>.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and<br />
<strong>Services</strong> <strong>Systems</strong> Integration<br />
Plan<br />
Appendices<br />
August 2008
The research, development, and publication <strong>of</strong> this plan was funded in part by the <strong>Housing</strong><br />
Opportunities for Persons with <strong>AIDS</strong> (HOPWA) National Technical Assistance Program in partnership<br />
with the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development's Office <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong>. The<br />
substance and findings <strong>of</strong> the work are dedicated to the public. The author and publisher are solely<br />
responsible for the accuracy <strong>of</strong> the statements and interpretations contained in this publication. Such<br />
interpretations do not necessarily reflect the views <strong>of</strong> the Government.
Table <strong>of</strong> Contents<br />
Appendix 1: Affordable <strong>Housing</strong> Resource Guide .....................................................................A-1<br />
<strong>Housing</strong> Planning Processes ........................................................................................................A-2<br />
<strong>Housing</strong> Resources ....................................................................................................................A-15<br />
Appendix 2: Stakeholder Survey Results ..................................................................................A-35<br />
Appendix 3: <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> Options .................................................................................A-41<br />
Emergency <strong>Housing</strong> Assistance.................................................................................................A-42<br />
Transitional <strong>Housing</strong> Assistance ...............................................................................................A-43<br />
Permanent <strong>Housing</strong> Assistance..................................................................................................A-44<br />
<strong>Services</strong> to Support <strong>Housing</strong> Stability .......................................................................................A-48<br />
Appendix 4: Federal and <strong>State</strong> Financing Sources for Affordable <strong>Housing</strong>..........................A-49<br />
U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development (HUD).................................................A-49<br />
Low Income <strong>Housing</strong> Tax Credits.............................................................................................A-53<br />
Human Resources <strong>Services</strong> Administration, Ryan White <strong>HIV</strong>/<strong>AIDS</strong> Treatment<br />
Modernization Act ....................................................................................................................A-54<br />
U.S. Department <strong>of</strong> Agriculture Rural Development, Rural <strong>Housing</strong> Service..........................A-55<br />
U.S. Department <strong>of</strong> Veterans Affairs Homeless Providers Grant and Per Diem Program.......A-55<br />
Appendix 5: Glossary <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong>- and <strong>Housing</strong>-Related Terms ........................................A-57
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-1<br />
Appendix 1: Affordable <strong>Housing</strong> Resource Guide<br />
The purpose <strong>of</strong> this resource guide is to describe existing housing resources, identify potential<br />
partnerships and referral sources, and facilitate the implementation <strong>of</strong> the <strong>Systems</strong> Integration Plan.<br />
As part <strong>of</strong> the development <strong>of</strong> the <strong>Oregon</strong> <strong>HIV</strong> <strong>Housing</strong> and Service <strong>Systems</strong> Integration Plan,<br />
Building Changes compiled this affordable housing resource guide for the balance <strong>of</strong> state (31<br />
counties outside the Portland metropolitan area). This resource guide is divided into two sections:<br />
information on housing planning processes, and information on available housing resources.<br />
The first section, <strong>Housing</strong> Planning Processes, describes statewide and local funding opportunities<br />
and planning processes for affordable housing, including state and local Consolidated Plans, and the<br />
Continuum <strong>of</strong> Care system. Each resource includes information on the planning process and<br />
provides the main contact. At the end <strong>of</strong> the first section are two calendars displaying timelines for<br />
funding applications and planning processes across the balance <strong>of</strong> state.<br />
The second section, <strong>Housing</strong> Resources, describes existing affordable housing resources in the<br />
balance <strong>of</strong> state, including housing authorities, local resource guides, regional housing centers,<br />
affordable housing developers, and community action agencies. Resources are grouped according to<br />
the four regions served by the <strong>Oregon</strong> <strong>Housing</strong> Opportunities in Partnership (OHOP) program (see<br />
map on page A-15 for map <strong>of</strong> OHOP regions).<br />
For information on the OHOP program, contact:<br />
Ryan Deibert<br />
Program Coordinator<br />
(971) 673-0145, ryan.j.deibert@state.or.us<br />
Denise Fry<br />
<strong>Housing</strong> Coordinator, Region 1 (Northwest)<br />
503-559-4389, denise.fry@state.or.us<br />
Renee Yandell<br />
<strong>Housing</strong> Coordinator, Region 2 (Central)<br />
541-914-2032, renee.c.yandell@state.or.us<br />
Jakki Calhoun<br />
<strong>Housing</strong> Coordinator, Region 3 (Southern)<br />
541-840-3592, jacole.j.calhoun@state.or.us<br />
Meredith Bricker<br />
<strong>Housing</strong> Coordinator, Region 4 (Eastern)<br />
541-325-1014, meredith.bricker@state.or.us
A-2 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
<strong>Housing</strong> Planning Processes<br />
As in most communities, funding for affordable housing in <strong>Oregon</strong> is dispersed across many levels<br />
<strong>of</strong> government and is subject to different policies, priorities, and timelines. The following sections<br />
indentify the planning processes across the state (excluding the five-county Portland metropolitan<br />
area) that define funding priorities for some <strong>of</strong> the most important resources. Two calendars for<br />
funding applications and planning processes are found at the end <strong>of</strong> the section.<br />
Consolidated Plans and Related Processes<br />
The U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development (HUD) requires a single, consolidated<br />
submission process for four formula programs: Community Development Block Grants (CDBG),<br />
Emergency Shelter Grants (ESG), HOME Investment Partnership Program, and <strong>Housing</strong><br />
Opportunities for Persons with <strong>AIDS</strong> (HOPWA). Local and state governments develop<br />
Consolidated Plans (Con Plans) with public input to define the funding priorities for these four<br />
programs in their jurisdictions.<br />
<strong>State</strong> <strong>of</strong> <strong>Oregon</strong> Consolidated Plan<br />
Online: www.oregon.gov/OHCS/HRS_Consolidated_Plan_5yearplan.shtml<br />
Background: <strong>Oregon</strong> <strong>Housing</strong> and Community <strong>Services</strong> (OHCS) administers the HOME program;<br />
<strong>Oregon</strong> Economic and Community Development Department (OECDD) administers<br />
the CDBG program; and <strong>Oregon</strong> Department <strong>of</strong> Human <strong>Services</strong> (DHS) administers<br />
the HOPWA program in the balance <strong>of</strong> state (OHOP).<br />
Process: The current five-year Con Plan covers 2006-2010. Each year, OHCS develops an<br />
Annual Action Plan to describe the implementation <strong>of</strong> the five-year plan in the<br />
coming year. The draft 2008 Annual Action Plan was released in September 2007 for<br />
public comment until October 2007.<br />
Contact: Loren Schultz, Consolidated Plan Manager, OHCS<br />
503-230-9963, loren.schultz@hcs.state.or.us<br />
Notes: Ryan Deibert, OHOP Program Coordinator, participated in the development <strong>of</strong> the<br />
2008 Annual Action Plan.<br />
<strong>State</strong> <strong>of</strong> <strong>Oregon</strong> Consolidated Funding Cycle (CFC)<br />
Online: www.oregon.gov/OHCS/HRS_CFC_Overview.shtml<br />
Background: OHCS allocates its affordable housing funding through the Spring and Fall CFC<br />
process, including the Low Income <strong>Housing</strong> Tax Credit, <strong>Housing</strong> PLUS, <strong>Oregon</strong><br />
Affordable <strong>Housing</strong> Tax Credit, HOME Investment Partnerships, <strong>Housing</strong><br />
Development Grant (Trust Fund), Low-Income Weatherization, and HELP<br />
(Financing Adjustment Factor Savings Fund) programs. Starting in 2008, the<br />
majority <strong>of</strong> funding will shift from the Fall to the Spring cycle. The Fall 2007 CFC<br />
included $27.5 million in funding. The Spring 2008 CFC includes $11.6 million,<br />
including the first $4 million distribution <strong>of</strong> the new <strong>Housing</strong> PLUS funds.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-3<br />
Process: Funding priorities are influenced by the <strong>Oregon</strong> Consolidated Plan (for HOME), the<br />
Qualified Allocation Plan (for Low Income <strong>Housing</strong> Tax Credits), and OHCS<br />
performance measures based on legislative goals.<br />
For the Fall 2007 funding cycle, OHCS released the application in May, held<br />
trainings in June, and set the application deadline for July 27, 2007. For the Spring<br />
2008 funding cycle, OHCS released the application in December 2007 with a<br />
deadline <strong>of</strong> February 29, 2008.<br />
In order to apply for CFC funding, the agency must contact an OHCS Regional<br />
Advisor more than one month before the application deadline to schedule a site visit.<br />
Contact: OHCS Regional Advisors:<br />
Vince Chiotti, Metro and Northwest Region<br />
503-963-2284, vince.chiotti@hcs.state.or.us<br />
Jack Duncan, Mid-Willamette Region<br />
503-986-2044, jack.duncan@hcs.state.or.us<br />
(Temporary Vacancy), Southwest Region<br />
Contact Deborah Price (see below)<br />
Deborah Price, Central Region<br />
541-460-3231, deborah.price@hcs.state.or.us<br />
Bruce Buchanan, East Region<br />
541-980-6300, bruce.buchanan@hcs.state.or.us<br />
Notes: OHCS sets funding targets for the CFC, including 10 percent <strong>of</strong> units dedicated for<br />
30 percent AMI or below, and 50 percent <strong>of</strong> units for individuals with special needs.<br />
These targets were not met in 2006. The special needs target has not been met since<br />
2002. In 2007, the definition <strong>of</strong> special needs was expanded to include ex-<strong>of</strong>fenders<br />
and chronically homeless persons.
A-4 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Figure 1 shows the map <strong>of</strong> the five OHCS regions.<br />
Figure 1:<br />
Map <strong>of</strong> OHCS Regions<br />
Qualified Allocation Plan (Low Income <strong>Housing</strong> Tax Credits)<br />
Online: www.ohcs.oregon.gov/OHCS/HRS_LIHTC_Program.shtml<br />
Background: The Qualified Allocation Plan (QAP) defines funding priorities for the Low Income<br />
<strong>Housing</strong> Tax Credit program.<br />
Process: OHCS accepted public comments on the draft 2007 QAP from April through June<br />
2006. OHCS is expected to release the draft 2008 QAP in March 2008 and accept<br />
comments for 30 days.<br />
Contact: Karen Clearwater, OHCS<br />
503-986-0968, karen.clearwater@hcs.state.or.us
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-5<br />
Local Consolidated Plan Five-Year Cycles<br />
Each jurisdiction involves substantial community input during the year preceding the adoption <strong>of</strong> a<br />
new five-year Con Plan. The following list includes the expiration months for each Con Plan in the<br />
balance <strong>of</strong> state:<br />
June 2008: Corvallis<br />
June 2009: Bend<br />
December 2009: Ashland, Medford, and Salem<br />
June 2010: Eugene/Springfield<br />
December 2010: <strong>State</strong> <strong>of</strong> <strong>Oregon</strong><br />
City <strong>of</strong> Ashland Consolidated Plan<br />
Online: http://www.ashland.or.us/CCBIndex.asp?CCBID=196<br />
Background: In FY 2007, Ashland received $210,000 in CDBG funds. Ashland has a 2005-2009<br />
Con Plan.<br />
Process: Applications for funding are due in March 2008, and funding decisions are expected<br />
in May 2008.<br />
Contact: Brandon Goldman, Martha Bennett<br />
541-552-2076, brandong@ashland.or.us<br />
541-552-2100, bennettm@ashland.or.us<br />
City <strong>of</strong> Bend Consolidated Plan<br />
Online: http://www.ci.bend.or.us/depts/urban_renewal_economic_development/<br />
Background: In FY 2007, Bend received $437,156 in CDBG funds. The 2004-2009 Con Plan<br />
described persons living with <strong>HIV</strong>/<strong>AIDS</strong> as a “Low” priority among special needs<br />
populations. The Con Plan described the unmet housing need as “Minimal,” and had<br />
a goal <strong>of</strong> developing 20 units <strong>of</strong> housing for people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
Process: Bend released an RFP for CDBG funds, with applications due in January 2008, and<br />
funding decisions expected in May 2008.<br />
Contact: John Russell, Jim Long<br />
541-312-4915, jrussell@ci.bend.or.us, jlong@ci.bend.or.us<br />
City <strong>of</strong> Corvallis Consolidated Plan<br />
Online: www.ci.corvallis.or.us/index.php?option=content&task=view&id=296&Itemid=247<br />
Background: In FY 2007, Corvallis received $556,048 in CDBG funds and $420,259 in HOME<br />
funds. The 2003-2008 Con Plan described persons living with <strong>HIV</strong>/<strong>AIDS</strong> as a “Low”<br />
priority among special needs populations.<br />
Process: Corvallis issued an RFP for CDBG and HOME funds for 2008-2009. Applications<br />
are due in January 2008, with funding decisions expected in April. Corvallis is<br />
currently developing the next five-year Con Plan. The Corvallis <strong>Housing</strong> and<br />
Community Development Commission (HCDC) formulates and recommends<br />
policies on housing issues. Meetings are typically the third Wednesday <strong>of</strong> the month.<br />
Contact: Kent Weiss<br />
541-757-6944 x4, kentweiss@ci.corvallis.or.us
A-6 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
City <strong>of</strong> Eugene Consolidated Plan<br />
Online: http://www.eugene-or.gov/portal/server.pt?open=512&objID=229&PageID<br />
=0&cached=true&mode=2&userID=2<br />
Background: In FY 2007, Eugene received $1,415,794 in CDBG funds and $1,451,705 in HOME<br />
funds. Eugene has a joint Con Plan with Springfield for 2005-2010.<br />
Process: Applications for the latest RFP are due by February 2008, with funding decisions<br />
expected in June 2008.<br />
Contact: Linda Dawson, Richie Weinman<br />
541-682-5071, Linda.L.Dawson@ci.eugene.or.us<br />
541-682-5533, richie.d.weinman@ci.eugene.or.us<br />
City <strong>of</strong> Medford Consolidated Plan<br />
Online: http://www.ci.medford.or.us/Page.asp?NavID=632<br />
Background: In FY 2007, Medford received $636,217 in CDBG funds. The 2005-2009 Con Plan<br />
described persons living with <strong>HIV</strong>/<strong>AIDS</strong> as a “Low” priority among special needs<br />
populations, and had a goal <strong>of</strong> developing zero units <strong>of</strong> housing for people living<br />
with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
Process: Applications are due by February 2008, and funding decisions are expected by May<br />
2008.<br />
Contact: Louise Dix, Dan Goltz<br />
541-774-2090, Louise.dix@ci.medford.or.us<br />
541-774-2089, dan.goltz@ci.medford.or.us<br />
City <strong>of</strong> Salem Consolidated Plan<br />
Online: www.salem.or.us/export/departments/urbandev/housing_federal_cdbg.htm<br />
Background: In FY2007, the City <strong>of</strong> Salem received $1.5 million in CDBG funds and $920,000 in<br />
HOME funds. Salem’s 2005-2009 Consolidated Plan identified four funding<br />
priorities: homelessness, affordable housing, removal <strong>of</strong> affordable housing barriers,<br />
and community development.<br />
Process: Salem adopted its 2007-2008 Annual Action Plan in April 2007. Applications for<br />
2008-2009 CDBG / HOME funding were released in October 2007, and were due by<br />
December 2007.<br />
Contact: Rena Peck<br />
503-588-6178, rpeck@city<strong>of</strong>salem.net<br />
City <strong>of</strong> Springfield Consolidated Plan<br />
Online: http://www.ci.springfield.or.us/dsd/<strong>Housing</strong>/housing.home.htm<br />
Background: In FY 2007, Springfield received $628,101 in CDBG funds. Springfield and Eugene<br />
have a joint Con Plan for 2005-2010.<br />
Process: Applications for the latest RFP are due by February 2008, with funding decisions<br />
expected in June 2008.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-7<br />
Contact: Kevin Ko<br />
541-726-3656, kko@ci.springfield.or.us<br />
Continua <strong>of</strong> Care (CoC)<br />
In order to encourage the integration and coordination <strong>of</strong> community homeless assistance, HUD’s<br />
three primary homeless assistance programs – the Supportive <strong>Housing</strong> Program (SHP), Shelter Plus<br />
Care (S+C), and the Section 8 Moderate Rehabilitation Single Room Occupancy Program (SRO<br />
Mod. Rehab.) – are combined under the Continuum <strong>of</strong> Care (CoC) planning and allocation process.<br />
The establishment <strong>of</strong> a CoC system involves a community-wide or region-wide process involving<br />
government agencies, nonpr<strong>of</strong>it housing and service providers, private foundations, homeless or<br />
formerly homeless individuals, and other stakeholders.<br />
Each CoC is allocated an initial pro rata need funding amount based on the relative homeless<br />
assistance need assigned to a community using U.S. Census Bureau data. Communities can receive<br />
funding above this level through successful applications for “bonus” projects that must provide<br />
permanent housing for chronically homeless individuals.<br />
Figure 2 on the following page shows the map <strong>of</strong> the CoC in <strong>Oregon</strong>, followed by a discussion <strong>of</strong><br />
each CoC in the balance <strong>of</strong> state.
A-8 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Figure 2:<br />
Map <strong>of</strong> Continua <strong>of</strong> Care in <strong>Oregon</strong><br />
Salem / Marion / Polk Continuum <strong>of</strong> Care<br />
Background: This CoC serves Marion and Polk Counties, including the cities <strong>of</strong> Salem and Keizer.<br />
The pro-rata share for this CoC is approximately $400,000. Because <strong>of</strong> their<br />
successful applications, their awards for 2006 were about $800,000. Going forward,<br />
the maximum possible bonus project would be $34,000 per year, which would likely<br />
fund three tenant vouchers for chronically homeless individuals. There may be<br />
agencies interested in pursuing bonus projects for the 2008 application.<br />
Process: The steering committee is called the <strong>Housing</strong> Collaborative, and evaluates and<br />
prioritizes programs for funding prior to submitting the application. The CoC meets<br />
bimonthly, second Friday at 10:30am. Next meeting is March 14, 2008.<br />
Contact: Carla Cary, Mid-Willamette Valley Community Action Agency (MWVCAA)<br />
503-585-6232, 503-399-9080, caryc@mwvcaa.org<br />
Lane County Continuum <strong>of</strong> Care<br />
Background: This CoC serves Lane County, including the cities <strong>of</strong> Eugene and Springfield. The<br />
pro-rata share is similar to Marion / Polk CoC (approximately $400,000), but
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-9<br />
funding awards have been higher (nearly $2 million), partly because <strong>of</strong> use <strong>of</strong> Shelter<br />
Plus Care. Going forward, the maximum possible bonus project would be about<br />
$60,000 over two years. Administration costs are the biggest barrier to applying for<br />
bonus.<br />
Process: CoC typically meets once per month. Contact Pearl Wolfe (below) for information<br />
on meetings.<br />
Contact: Pearl Wolfe, Lane County Human <strong>Services</strong> Commission<br />
541-682-4629, pearl.wolfe@co.lane.or.us<br />
Jackson County Continuum <strong>of</strong> Care<br />
Background: This CoC serves Jackson County, including the cities <strong>of</strong> Medford and Ashland. The<br />
pro-rate share is approximately $200,000, and the CoC was not awarded extra<br />
funding in FY 2006. Administration and homelessness definitions are obstacles for<br />
local providers. The <strong>Housing</strong> Authority <strong>of</strong> Jackson County has not historically had<br />
interest in special needs housing.<br />
Process: The Jackson County Homeless Task Force is the guiding body for the Jackson<br />
County 10-Year Plan to End Homelessness (with Jackson County Health and Human<br />
<strong>Services</strong>) and for the CoC. Contact Ed Angeletti (below) for more information.<br />
Contact: Ed Angeletti, Cindy Dyer, ACCESS, Inc.<br />
541-774-4330, eangeletti@access-inc.org<br />
541-774-4319, cdyer@access-inc.org<br />
Central <strong>Oregon</strong> Continuum <strong>of</strong> Care<br />
Background: This CoC serves Crook, Deschutes, and Jefferson Counties in central <strong>Oregon</strong>,<br />
including the cities <strong>of</strong> Bend and Redmond. The CoC covers a large rural area and<br />
has a pro-rata share <strong>of</strong> less than $200,000. The CoC uses its funding across a<br />
number <strong>of</strong> programs.<br />
Process: The CoC usually meets the third Friday <strong>of</strong> the month at 8:30am, in Bend or<br />
Redmond. There currently is no <strong>HIV</strong>/<strong>AIDS</strong> representation at the CoC.<br />
Contact: Corky Senecal, Neighbor Impact<br />
541-548-2380 x101, corkys@neighborimpact.org<br />
Rural <strong>Oregon</strong> Continuum <strong>of</strong> Care (ROCC), also called <strong>Oregon</strong> <strong>Balance</strong> <strong>of</strong> <strong>State</strong> CoC<br />
Background: ROCC serves rural areas <strong>of</strong> the state, including Baker, Benton, Clatsop, Columbia,<br />
Coos, Curry, Douglas, Gilliam, Grant, Harney, Hood River, Josephine, Klamath,<br />
Lake, Lincoln, Linn, Malheur, Morrow, Sherman, Tillamook, Umatilla, Union,<br />
Wallowa, Wasco, Wheeler, and Yamhill Counties. The 2007 awards totaled $1.5<br />
million, including 19 transitional and two permanent housing projects. One <strong>of</strong> the<br />
permanent housing projects is a partnership with the Office <strong>of</strong> Addictions and<br />
Mental Health (AMH) to serve chronically homeless individuals with mental illness.<br />
Process: ROCC usually meets the second Wednesday <strong>of</strong> each month in Salem.<br />
Contact: Ann Brown, OHCS<br />
503-986-2122, ann.brown@hcs.state.or.us
A-10 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Other Planning Processes and Funding Sources<br />
Ending Homelessness Advisory Committee (EHAC)<br />
Online: http://www.ehac.oregon.gov/OHCS/EHAC/<br />
Background: Established by the Governor in 2006 to create the 10-Year Plan to End Homelessness<br />
for <strong>Oregon</strong>. As <strong>of</strong> April 2007, five counties in the balance <strong>of</strong> state were in the<br />
process <strong>of</strong> developing 10-Year Plans, and eight more were reported to be considering<br />
plans. As <strong>of</strong> January 2008, the first phase, understanding homelessness, was<br />
completed and the committee was working to narrow and define strategies.<br />
Process: EHAC typically meets the third Friday <strong>of</strong> the month, 10am to noon in Salem.<br />
Contact: Roberto Franco, OHCS<br />
503-986-6732, Roberto.Franco@hcs.state.or.us<br />
Lane County Intergovernmental <strong>Housing</strong> Policy Board<br />
Online: www.eugene-or.gov/portal/server.pt?open=512&objID=281&PageID=<br />
542&cached=true&mode=2&userID=2<br />
Background: The <strong>Housing</strong> Policy Board advises the Board <strong>of</strong> Commissioners and the Springfield<br />
and Eugene City Councils on the housing needs <strong>of</strong> the low-income residents, and<br />
develops a budget and work plan for targeting local government resources for<br />
housing related activities.<br />
Process: The <strong>Housing</strong> Policy Board is comprised <strong>of</strong> nine members, including city and county<br />
<strong>of</strong>ficials and public citizens. It typically meets the first Monday <strong>of</strong> the month.<br />
Contact: Richie Weinman<br />
541-682-5533, richie.d.weinman@ci.eugene.or.us<br />
Ryan White <strong>HIV</strong>/<strong>AIDS</strong> Treatment Modernization Act<br />
Online: http://egov.oregon.gov/DHS/ph/hiv/<br />
Background: The Ryan White CARE Act is a federally funded program that provides services to<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong>. Short-term and emergency housing are allowable<br />
under Ryan White.<br />
Process: In 2006, the <strong>HIV</strong> <strong>Housing</strong> Task Force created recommendations to help guide the<br />
OHOP and Ryan White housing programs.<br />
Contact: Annick Benson<br />
971-673-0142, annick.benson@state.or.us<br />
Addictions and Mental Health (AMH) Division – ECLO <strong>Housing</strong> Programs<br />
Background: AMH accepted funding requests until November 9, 2007, for the Expanding<br />
Community Living Opportunities (ECLO) 2007-2009 application process. ECLO<br />
provides funding for: structured and specialized residential programs for individuals<br />
under civil commitment; supportive housing for people leaving psychiatric hospitals,<br />
transitioning from youth to adult services, or who are ineligible for Medicaid; and<br />
housing development grants to develop new housing. All programs serve individuals<br />
with mental illness.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-11<br />
Process: Depending on the awards made from this funding round (to be announced in<br />
December 2007), AMH may announce additional application rounds during this<br />
biennium.<br />
Contact: Vicki Skryha, Community <strong>Housing</strong>, Employment & Supports Manager<br />
503-945-9722, vicki.skryha@state.or.us<br />
AMH Division – Community Mental Health <strong>Housing</strong> Fund (CMHHF)<br />
Background: These funds are used to support the development <strong>of</strong> housing for persons with<br />
chronic mental illness. Applicants may request up to $100,000 from the CMHHF for<br />
the purpose <strong>of</strong> creating new community housing opportunities for people with<br />
serious mental illness.<br />
Process: Solicitation usually occurs October <strong>of</strong> every year. Applications are reviewed and<br />
rated by an AMH appointed review panel. The review panel’s recommendations are<br />
presented to the AMH Assistant Director who makes the final funding decisions.<br />
Contact: Jeff Puterbaugh, <strong>Housing</strong> Development Coordinator<br />
503-947-5533, jeffrey.l.puterbaugh@state.or.us<br />
AMH Division – Alcohol and Drug Free (ADF) <strong>Housing</strong> Fund<br />
Background: The ADF <strong>Housing</strong> Fund awards were initiated in 1999 when the <strong>Oregon</strong> legislature<br />
approved funds for the expansion <strong>of</strong> alcohol and drug treatment services. One<br />
million dollars are available through the ADF <strong>Housing</strong> Fund in 2007-09. These<br />
funds are available to assist with the establishment <strong>of</strong> new housing for people in<br />
recovery from alcohol and drug abuse and who are actively involved in an approved<br />
treatment program.<br />
Process: Funds are available every biennium subject to legislatively approved budget.<br />
Applications are reviewed and rated by an AMH appointed review panel. The<br />
review panel’s recommendations are presented to the AMH Assistant Director who<br />
makes the final funding decisions.<br />
Contact: Elizabeth Anguiano, <strong>Housing</strong> Projects Coordinator<br />
503-947-5544, elizabeth.anguiano@state.or.us<br />
City <strong>of</strong> Bend Affordable <strong>Housing</strong> Fee RFP<br />
Online: http://www.ci.bend.or.us/depts/urban_renewal_economic_development/<br />
Background: Bend implemented an Affordable <strong>Housing</strong> Fee in 2006, and intends to release an<br />
RFP for new construction and rehabilitation <strong>of</strong> affordable homeownership and rental<br />
housing.<br />
Process: Latest round <strong>of</strong> applications were due in September 2007. The Affordable <strong>Housing</strong><br />
Advisory Committee meets monthly to discuss local affordable housing and make<br />
funding decisions.<br />
Contact: John Russell, Jim Long<br />
541-312-4915, jrussell@ci.bend.or.us, jlong@ci.bend.or.us
A-12 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Planning Calendars<br />
The calendars on the following two pages represent summaries <strong>of</strong> the planning processes and<br />
funding applications for affordable housing resources in the balance <strong>of</strong> state. The first calendar<br />
includes dates for availability <strong>of</strong> funding applications, application deadlines, and funding<br />
announcements. Dates are included for 2008 applications except where noted. The second calendar<br />
describes the monthly meeting schedules for the Continua <strong>of</strong> Care and other state and local planning<br />
processes.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-13<br />
Spring CFC<br />
Fall CFC<br />
HUD CoC<br />
SuperNOF<br />
A<br />
LIHTC<br />
QAP<br />
Salem<br />
Con Plan<br />
Corvallis<br />
Con Plan<br />
Eugene /<br />
Springfield<br />
Con Plan<br />
Ashland<br />
Con Plan<br />
Medford<br />
Con Plan<br />
Bend<br />
Con Plan<br />
Bend<br />
Affordable<br />
Hsg Fee<br />
JAN FEB MARCH APRIL MAY JUNE JULY AUG SEPT OCT NOV DEC<br />
App.<br />
Due:<br />
Jan 10<br />
App.<br />
Avail:<br />
Jan 10<br />
App.<br />
Due:<br />
Jan 9<br />
App.<br />
Due:<br />
Late Feb<br />
App.<br />
Due:<br />
Feb 27<br />
App.<br />
Due:<br />
Feb 22<br />
App.<br />
Avail:<br />
March 07<br />
Draft QAP available for<br />
public comments<br />
App.<br />
Due:<br />
March<br />
Funding<br />
Decision:<br />
April 8<br />
Funding<br />
Decision:<br />
May 23<br />
App. Avail:<br />
May<br />
Funding<br />
Decision:<br />
May<br />
Funding<br />
Decision:<br />
May<br />
Funding<br />
Decision:<br />
May 7<br />
App.<br />
Due:<br />
June 07<br />
Funding<br />
Decision:<br />
June<br />
App.<br />
Due:<br />
Late July<br />
App. Avail:<br />
July 07<br />
App.<br />
Due:<br />
Sept 07<br />
App.<br />
Avail:<br />
Oct 07<br />
App. Avail:<br />
Dec 07<br />
Funding<br />
Decision:<br />
Dec<br />
Funding<br />
Decision:<br />
Dec 07<br />
App. Due:<br />
Dec 07<br />
Funding<br />
Decision:<br />
Dec 07
A-14 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
First<br />
Second<br />
Third<br />
Fourth<br />
Meeting dates<br />
vary<br />
Schedule <strong>of</strong> Regular Meetings<br />
MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY<br />
Lane County<br />
Intergovernmental<br />
<strong>Housing</strong> Board<br />
Rural <strong>Oregon</strong><br />
CoC, in Salem<br />
Abbreviation Guide:<br />
CFC: Consolidated Funding Cycle<br />
CoC: Continuum <strong>of</strong> Care<br />
Con Plan: Consolidated Plan<br />
LIHTC QAP: Low Income <strong>Housing</strong> Tax Credit Qualified Allocation Plan<br />
Eugene / Springfield / Lane County CoC (monthly)<br />
Jackson County CoC<br />
City <strong>of</strong> Bend Affordable <strong>Housing</strong> Advisory Committee (monthly)<br />
Salem / Marion / Polk CoC<br />
(bimonthly – odd months)<br />
10:30am in Salem<br />
Central <strong>Oregon</strong> CoC,<br />
8:30am in Bend or Redmond<br />
Ending Homelessness<br />
Advisory Committee<br />
10am in Salem
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-15<br />
<strong>Housing</strong> Resources<br />
The following sections identify housing resources that are available across the balance <strong>of</strong> state,<br />
include online resource guides, housing authorities, housing resource centers, USDA Rural<br />
Development <strong>of</strong>fices, and affordable housing developers. The resources are grouped by region:<br />
statewide, Region 1 (Northwest), Region 2 (Central), Region 3 (Southern), and Region 4 (Eastern).<br />
Figure 3 shows the map <strong>of</strong> the <strong>Oregon</strong> <strong>Housing</strong> Opportunities in Partnership (OHOP) program<br />
regions, which cover the balance <strong>of</strong> state outside the Portland metropolitan area.<br />
<strong>State</strong>wide Resources<br />
Figure 3:<br />
Map <strong>of</strong> OHOP Regions<br />
HUD Subsidized Apartment Search<br />
Online: http://www.hud.gov/apps/section8/step2.cfm?state=OR<br />
Contact: n/a<br />
Programs: HUD <strong>of</strong>fers this online tool to search by city, county, or ZIP for subsidized rental<br />
housing. Listings include number <strong>of</strong> bedrooms and contact information.
A-16 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
USDA Rural Development Multifamily <strong>Housing</strong> Property Search<br />
Online: http://rdmfhrentals.sc.egov.usda.gov/RDMFHRentals/ (click on <strong>Oregon</strong>)<br />
Contact: See below for contact information <strong>of</strong> USDA RD regional service <strong>of</strong>fices.<br />
Programs: USDA <strong>of</strong>fers this online tool to search by county for subsidized rental housing.<br />
Listings include number <strong>of</strong> units, size <strong>of</strong> units, and contact information.<br />
USDA Rural Development in <strong>Oregon</strong><br />
Online: http://www.rurdev.usda.gov/OR/<br />
Contact: See below for contact information <strong>of</strong> USDA RD regional service <strong>of</strong>fices.<br />
Programs: USDA provides several housing programs in rural areas, including Rural Rental<br />
<strong>Housing</strong> loans to finance development <strong>of</strong> multifamily housing; home preservation<br />
grants; homeownership loans; and rental assistance for low-income households.<br />
<strong>Oregon</strong> <strong>AIDS</strong> Hotline<br />
Online: http://www.oregonaidshotline.com/<br />
Contact: n/a<br />
Programs: Cascade <strong>AIDS</strong> Project and <strong>Oregon</strong> DHS maintain these listings <strong>of</strong> services available<br />
throughout the state (including the Portland metropolitan area). Use menu bars on the<br />
left to search for resources by county. <strong>Housing</strong> resources are under the “Financial –<br />
Practical” heading.<br />
Our House <strong>of</strong> Portland<br />
Online: http://www.ourhouse<strong>of</strong>portland.org/<br />
Contact: 503-234-0175<br />
Programs: Our House operates a residential care facility in Portland that provides services for<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong> across the state. Residents work with skilled<br />
pr<strong>of</strong>essionals in nursing, social work and occupational therapy. Our House operates<br />
additional programs serving people living with <strong>HIV</strong>/<strong>AIDS</strong> in the Portland area.<br />
Oxford Houses<br />
Online: http://www.oxfordhouse.org/directory.php (directory by state)<br />
http://www.oxfordhouse.org/locate_houses.php (search for vacancies and by<br />
gender)<br />
Contact: See online listings for contacts.<br />
Programs: Oxford Houses are self-run recovery house programs for individuals recovering from<br />
alcoholism and drug addiction. Most houses have between six and 12 residents. They<br />
are strictly alcohol- and drug-free environments. There are approximately 130<br />
Oxford Houses across the state, including the Portland metropolitan area.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-17<br />
<strong>Oregon</strong> Tribal <strong>Housing</strong> Guide<br />
Online: http://www.frbsf.org/community/native/tribeshousingguide_oregon.pdf<br />
Contact: n/a<br />
Programs: The Federal Reserve Bank <strong>of</strong> San Francisco compiled this housing guide for Native<br />
American tribes in <strong>Oregon</strong> in 2004.<br />
<strong>Oregon</strong> Health Care Association<br />
Online: http://www.ohca.com/default.htm<br />
Contact: 503-726-5260<br />
Programs: The OHCA is a statewide trade association that represents the network <strong>of</strong> skilled<br />
nursing facilities, assisted living and residential care facilities, integrated health<br />
systems, independent senior living communities and licensed in-home care agencies.<br />
Association <strong>of</strong> <strong>Oregon</strong> Community Development Organizations / Community Development<br />
Network<br />
Online: http://www.aocdo.org/<br />
Contact: Sophia McDonald, smcdonald@aocdo.org, (503) 223-4041 (executive director)<br />
Mike Anderson, mike@cdnportland.org (communications director)<br />
Programs: Not a direct housing resource, but a way to connect with housing partners. AOCDO<br />
will merge with Portland-based CDN in July 2008. The two organizations represent<br />
agencies working in affordable housing and community development.<br />
<strong>Oregon</strong> Community Development Collaborative<br />
Online: http://www.tnpf.org/programs/support_or_cdc/ocdc.php<br />
Contact: 503-226-3001, info@tnpf.org<br />
Programs: Not a direct housing resource, but a collaboration between Neighborhood Partnership<br />
Fund, Enterprise Community Partners, and <strong>Oregon</strong> <strong>Housing</strong> and Community<br />
<strong>Services</strong>. OCDC provides operating support and technical assistance to communitybased<br />
organizations.
A-18 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Region 1 Resources<br />
<strong>Housing</strong> Authorities<br />
<strong>Housing</strong> Authority <strong>of</strong> Lincoln County<br />
Online: www.halc.info<br />
Contact: 541-265-6057, gstone.halc@newportnet.com<br />
Programs: Provides 497 Section 8 vouchers, 120 public housing units, and over 100 additional<br />
low-income units in Lincoln County. Waiting list for Section 8 is up to two years.<br />
Other waiting lists may be shorter.<br />
Linn-Benton <strong>Housing</strong> Authority<br />
Online: www.l-bha.org<br />
Contact: 541-926-4497, mail@l-bha.org, donna@l-bha.org<br />
Programs: Provides 2,435 Section 8 vouchers, and 108 additional low-income units in Linn and<br />
Benton Counties. The Section 8 wait list is open. Other programs include:<br />
• Family Self-Sufficiency program for Section 8 residents<br />
• Special needs housing for individuals with mental illness<br />
• Homeownership assistance<br />
Marion County <strong>Housing</strong> Authority<br />
Online: www.co.marion.or.us/HA/<br />
Contact: 503-373-4448, housingauthority@co.marion.or.us<br />
Programs: Provides 1,175 Section 8 vouchers and 46 public housing units in Marion County<br />
(outside the Salem / Keizer Urban Growth Boundary). Waiting list for Section 8 is<br />
up to six months, typically shorter than Salem <strong>Housing</strong> Authority waiting list.<br />
Northwest <strong>Oregon</strong> <strong>Housing</strong> Authority<br />
Online: www.nwoha.org<br />
Contact: 503-861-0119, john@nwoha.org<br />
Programs: Provides 1,139 Section 8 vouchers, and 128 additional low-income units in Clatsop,<br />
Columbia, and Tillamook Counties. Waiting list for Section 8 is up to two years. In<br />
addition, Tenant Based Rental Assistance (TBRA) program provides rental<br />
assistance for up to six months.<br />
Salem <strong>Housing</strong> Authority<br />
Online: www.city<strong>of</strong>salem.net/sha<br />
Contact: 503-588-6368, housing@city<strong>of</strong>salem.net<br />
Programs: Provides 2,868 Section 8 vouchers, 337 public housing units, and 341 additional<br />
low-income housing units in the Cities <strong>of</strong> Salem and Keizer. Waiting list for Section
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-19<br />
8 is up to two years. Other waiting lists range from three months to three years. SHA<br />
is an active developer <strong>of</strong> low-income housing, but has not targeted special needs,<br />
besides senior housing. Additional programs include:<br />
• HOME security deposit program for Section 8 recipients<br />
West Valley <strong>Housing</strong> Authority<br />
Online: www.wvpha.org<br />
• The Interim <strong>Housing</strong> Program provides a cash assistance grant to help with<br />
one month’s rent or a security deposit<br />
• Family Self-Sufficiency program for Section 8 and public housing residents.<br />
Program helps families increase income, and funds an escrow account that is<br />
released at program completion<br />
• Homeownership programs include Individual Development Accounts, down<br />
payment assistance, low interest loans, and training<br />
Contact: 503-623-8387, wvpha@wvpha.org, ljenning@wvpha.org<br />
Programs: Provides 699 Section 8 vouchers and 380 public housing units in Polk County<br />
(outside the Salem / Keizer Urban Growth Boundary). Waiting list for Section 8 is<br />
typically shorter than Salem <strong>Housing</strong> Authority waiting list.<br />
Regional <strong>Housing</strong> Centers<br />
Linn-Benton-Lincoln <strong>Housing</strong> Center<br />
Online: www.csc.gen.or.us/lblrhc.htm<br />
Contact: 541-752-0667, kramsden@csc.gen.or.us<br />
Programs: Provides housing information and referrals in Benton, Lincoln, and Linn Counties.<br />
Operated by Community <strong>Services</strong> Consortium in Corvallis.<br />
Northwest <strong>Oregon</strong> Regional <strong>Housing</strong> Center<br />
Online: www.cat-team.org<br />
Contact: 503-397-3511<br />
Programs: Provides housing information and referrals in Clatsop, Columbia, and Tillamook<br />
Counties. Operated by Community Action Team, Inc. (CAT) in St. Helens.<br />
Yamhill-Polk Regional <strong>Housing</strong> Center<br />
Online: www.hayc.org/homeowners/housing_resource_center<br />
Contact: 503-883-4307, 888-434-6571, kbrummert@hayc.org<br />
Programs: Provides housing information and referrals in Yamhill and Polk Counties. Operated<br />
by the <strong>Housing</strong> Authority <strong>of</strong> Yamhill County in McMinnville.
A-20 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
USDA Rural Development Offices<br />
USDA Rural Development, Salem Local Office<br />
Online: http://www.rurdev.usda.gov/OR/<br />
Contact: 503-399-5741<br />
Programs: Serves Clackamas, Clatsop, Columbia, Marion, Multnomah, Polk, Tillamook,<br />
Washington, and Yamhill Counties.<br />
Affordable <strong>Housing</strong> Developers<br />
Community Action Team, Inc. (CAT)<br />
Online: www.cat-team.org<br />
Contact: 503-397-3511<br />
Programs: Affordable housing developer in Columbia, Clatsop, and Tillamook Counties.<br />
Programs include emergency housing, rehabilitation, and energy assistance.<br />
Polk Community Development Corporation<br />
Online: http://www.polkcdc.org/<br />
Contact: 503-831-3173<br />
Programs: Affordable housing developer.<br />
Salem Keizer Community Development Corporation<br />
Online: http://www.salemcdc.org/<br />
Contact: 503-856-7077<br />
Programs: Affordable housing developer in Marion County. Other programs include<br />
Homeownership and Financial Education, and Individual Development Accounts.<br />
Shangri-La Corp.<br />
Online: http://www.shangrilacorp.org/<br />
Contact: 503-581-1732, (x329 for housing assistance programs)<br />
Programs: Affordable housing developer in Marion, Polk, and Lincoln Counties. Operates lowincome<br />
and special needs housing. Other programs include:<br />
• Supported employment services<br />
• <strong>Services</strong> for people with mental illness and co-occurring disorders<br />
• Educational services for ex-<strong>of</strong>fenders<br />
Other <strong>Housing</strong> and Related Resources<br />
Mid-Willamette Valley Community Action Agency, Community Resource Program<br />
Online: www.mwvcaa.org/crp/crp.html
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-21<br />
Contact: 503-585-6232, 503-399-9080<br />
Programs: Programs include Tenant Based Rental Assistance in Marion and Polk Counties, a<br />
homeless referral and drop-in center (the ARCHES project), and the <strong>Housing</strong><br />
Stabilization program for families.
A-22 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Region 2 Resources<br />
<strong>Housing</strong> Authorities<br />
Coos-Curry <strong>Housing</strong> Authority<br />
Online: n/a<br />
Contact: 541-756-4111, pcolbert@uci.net<br />
Programs: Provides 777 Section 8 vouchers and 52 public housing units in the City <strong>of</strong> North<br />
Bend and in Coos and Curry Counties.<br />
<strong>Housing</strong> and Community <strong>Services</strong> Agency <strong>of</strong> Lane County (HACSA)<br />
Online: www.hacsa.org<br />
Contact: 541-682-3755, 541-682-2542, section8info@hacsa.org, housinginfo@hacsa.org,<br />
gsustello@hacsa.org<br />
Programs: Provides 2,639 Section 8 vouchers, 708 public housing units, and more than 400<br />
low-income housing units in Lane County. The Section 8 waiting list is currently<br />
closed. Additional housing programs include:<br />
• Free weatherization services to income-eligible home-owners and renters.<br />
Seniors and persons with disabilities are targeted as first priority.<br />
Linn-Benton <strong>Housing</strong> Authority<br />
Online: www.l-bha.org<br />
• Family Self-Sufficiency program for Section 8 and public housing residents.<br />
Program helps families increase income, and funds an escrow account that is<br />
released at program completion.<br />
• HACSA receives Shelter Plus Care funding from the Continuum <strong>of</strong> Care, and<br />
partners with ShelterCare to serve formerly homeless people.<br />
Contact: 541-926-4497, mail@l-bha.org, donna@l-bha.org<br />
Programs: (See listing in Region 1 for more details.)<br />
Regional <strong>Housing</strong> Centers<br />
Homeownership Center <strong>of</strong> Lane County<br />
Online: http://www.nedcocdc.org/homeown.htm<br />
Contact: 541-345-7106<br />
Programs: Provides housing information and referrals in Lane County. Operated by NEDCO<br />
(see following page).<br />
Linn-Benton-Lincoln <strong>Housing</strong> Center<br />
Online: www.csc.gen.or.us/lblrhc.htm
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-23<br />
Contact: 541-752-0667, kramsden@csc.gen.or.us<br />
Programs: Provides housing information and referrals in Benton, Lincoln, and Linn Counties.<br />
Operated by Community <strong>Services</strong> Consortium in Corvallis.<br />
USDA Rural Development Offices<br />
USDA Rural Development, Eugene Local Office<br />
Online: http://www.rurdev.usda.gov/OR/<br />
Contact: 541-465-6443<br />
Programs: Serves Benton, Lane, Linn and Lincoln Counties.<br />
Affordable <strong>Housing</strong> Developers<br />
Metropolitan Affordable <strong>Housing</strong> Corp.<br />
Online: http://www.metroaffordablehousing.org/<br />
Contact: 541-683-1751<br />
Programs: Affordable housing developer in Lane County.<br />
Neighborhood Economic Development Corporation (NEDCO)<br />
Online: http://www.nedcocdc.org/<br />
Contact: 541-345-7106<br />
Programs: Affordable housing developer. NEDCO also administers Valley Individual<br />
Development Accounts (VIDA), which provide a savings match for homeownership<br />
or job training.<br />
St. Vincent de Paul Lane County<br />
Online: http://www.svdp.us/<br />
Contact: Anne Williams, 541-687-5820 x 127, awilliams@svdp.us, info@svdp.us<br />
Programs: Affordable housing developer. St. Vincent has existing partnerships with <strong>HIV</strong><br />
Alliance Ryan White case managers. St. Vincent has a closed wait list system but<br />
accepts applications for brief windows in January, April, July, and October. Other<br />
programs include:<br />
• Second Chance renters’ rehabilitation program that links to 60 landlords for<br />
program graduates<br />
• Vet LIFT supported housing program for dually-diagnosed veterans<br />
• Vocational services<br />
• Overnight parking program<br />
• Social <strong>Services</strong> Office and emergency assistance
A-24 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Umpqua CDC<br />
Online: http://www.umpquacdc.org/<br />
Contact: 541-267-6505, 541-673-4909<br />
Programs: Affordable housing developer in Douglas, Coos, and Curry Counties. Special needs<br />
housing currently includes programs for people with brain injuries, victims <strong>of</strong><br />
domestic violence, and autistic adults. Other programs include housing rehabilitation<br />
and regional housing centers.<br />
Other <strong>Housing</strong> and Related Resources<br />
Lane County Human <strong>Services</strong> Commission<br />
Online: http://www.lanecounty.org/hsc/<br />
Contact: HOME TBA program, 541-682-3798<br />
Pearl Wolfe, Homeless services, 541-682-4629, pearl.wolfe@co.lane.or.us<br />
Programs: Community action agency sponsored by Lane County. Programs include:<br />
• HOME Tenant Based Rental Assistance (TBA)<br />
• Weatherization and energy assistance<br />
• List <strong>of</strong> other services available online at:<br />
http://www.lanecounty.org/HSC/ProvidersPrograms.htm<br />
ShelterCare<br />
Online: http://www.sheltercare.org<br />
Contact: Erin Bonner, 541-686-1262 x313, ebonner@sheltercare.org<br />
Chris Steele, 541-686-1262 x311, csteele@sheltercare.org<br />
Programs: Lane County housing and services provider focusing on homeless and mentally ill<br />
populations. People are selected <strong>of</strong>f wait lists into programs that match their service<br />
needs, not necessarily in order <strong>of</strong> application. Programs include:<br />
• Shelter Plus Care vouchers for formerly homeless, administered with HACSA<br />
• Emergency Shelter and Support provides support and housing in community<br />
residential settings<br />
• Transitional <strong>Services</strong> provides ongoing staff support after families leave<br />
shelter for housing in the community<br />
• Homelessness Prevention provides small amounts <strong>of</strong> financial assistance<br />
coupled with one-on-one support and training<br />
• Crisis management and intensive care programs provide varying levels <strong>of</strong><br />
support and housing needed during a mental health crisis<br />
• Supported vocational services for individuals with mental illness<br />
Sponsors, Inc.<br />
Online: http://www.sponsorsinc.org/
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-25<br />
Contact: 541-485-8341<br />
Programs: Provides housing with services for ex-<strong>of</strong>fenders in Lane County. Programs include:<br />
• Men’s and Women’s Transitional housing for ex-prisoners. These programs<br />
are alcohol- and drug-free and seek to help achieve self-sufficiency.<br />
• Sex <strong>of</strong>fender housing for up to two years
A-26 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Region 3 Resources<br />
<strong>Housing</strong> Authorities<br />
Coos-Curry <strong>Housing</strong> Authority<br />
Online: n/a<br />
Contact: 541-756-4111, pcolbert@uci.net<br />
Programs: Provides 777 Section 8 vouchers and 52 public housing units in the City <strong>of</strong> North<br />
Bend and in Coos and Curry Counties.<br />
<strong>Housing</strong> Authority <strong>of</strong> Douglas County<br />
Online: n/a<br />
Contact: 541-673-6548, telye@hadcor.org, jambrosini@hadcor.org<br />
Programs: Provides 651 Section 8 vouchers and 155 public housing units in Douglas County.<br />
<strong>Housing</strong> Authority <strong>of</strong> Jackson County<br />
Online: www.hajc.net<br />
Contact: 541-779-5785, info@hajc.net, Charlene@hajc.net<br />
Programs: Provides 1,605 Section 8 vouchers, 130 public housing units and has 11 buildings<br />
providing low-income housing units in Jackson County. The <strong>Housing</strong> Authority<br />
maintains an open wait list that can be as long as 2.5 years for Section 8. There are<br />
no preferences for people with disabilities or special needs units. Other programs:<br />
• HOME Tenant Based Rental Assistance (TBA)<br />
• Home rehabilitation loans<br />
Josephine <strong>Housing</strong> and Community Development Council<br />
Online: n/a<br />
Contact: 541-479-5520, teresa_jhcdc@charterinternet.com<br />
Programs: Provides 842 Section 8 vouchers to very low-income families in Josephine County.<br />
Klamath <strong>Housing</strong> Authority<br />
Online: n/a<br />
Contact: 541-884-0649, khadirector@cvc.net<br />
Programs: Provides 734 Section 8 vouchers and 57 public housing units in Klamath and Lake<br />
Counties.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-27<br />
Regional <strong>Housing</strong> Centers<br />
Klamath-Lake Regional <strong>Housing</strong> Center<br />
Online: http://www.klrhc.com<br />
Contact: 541-884-5593<br />
Programs: Provides housing information and referrals in Klamath and Lake Counties.<br />
Southern <strong>Oregon</strong> <strong>Housing</strong> Resource Center (SOHRC)<br />
Online: www.access-inc.org<br />
Contact: 541-779-6691<br />
Programs: Housed at ACCESS, SOHRC provides housing information and referrals in Jackson<br />
and Josephine Counties. SOHRC also maintains a thorough listing <strong>of</strong> housing<br />
resources, online at: http://www.access-inc.org/SectionIndex.asp?SectionID=9<br />
Southern <strong>Oregon</strong> Coast <strong>Housing</strong> Opportunities Center<br />
Online: http://www.umpquacdc.org/html/regional_housing_center.html<br />
Contact: Brenda Lewis, 541-267-6505, blewis@umpquacdc.org<br />
Programs: Provides housing information and referrals in Coos and Curry Counties. Operated by<br />
Umpqua CDC.<br />
Umpqua Regional <strong>Housing</strong> Center<br />
Online: http://www.umpquarhc.org<br />
Contact: 541-673-4909<br />
Programs: Provides housing information and referrals in Douglas County. Operated by Umpqua<br />
CDC.<br />
USDA Rural Development Offices<br />
USDA Rural Development, Medford Local Office<br />
Online: http://www.rurdev.usda.gov/OR/<br />
Contact: 541-776-4267<br />
Programs: Serves Jackson, Josephine, Klamath, and Lake Counties.<br />
USDA Rural Development, Roseburg Local Office<br />
Online: http://www.rurdev.usda.gov/OR/<br />
Contact: 541-673-6071<br />
Programs: Serves Coos, Curry, and Douglas Counties.
A-28 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Affordable <strong>Housing</strong> Developers<br />
ACCESS, Inc.<br />
Online: www.access-inc.org<br />
Contact: 541-779-6691<br />
Programs: Affordable housing developer in Jackson County. ACCESS conducts biannual needs<br />
assessment <strong>of</strong> community to determine project priorities. Current biennium is July<br />
2007 to June 2009. ACCESS will begin its next assessment in September 2008<br />
through surveys to clients and key stakeholders. Programs include:<br />
• HOME Tenant Based Rental Assistance (TBA) program with secondary<br />
preference for people living with <strong>HIV</strong>/<strong>AIDS</strong>, focusing on self-sufficiency<br />
• Weatherization and energy assistance<br />
• Rental and deposit assistance<br />
• Emergency homeless prevention (one or two months rent to prevent eviction)<br />
• Nutritional assistance<br />
OnTrack Recovery<br />
Online: http://www.ontrackrecovery.org/<br />
Contact: Rita Sullivan, 541-772-1777<br />
Programs: Affordable housing developer, including special needs housing. Currently operates<br />
Allan’s House, the only housing dedicated to people living with <strong>HIV</strong>/<strong>AIDS</strong> in the<br />
balance <strong>of</strong> state. Space is limited. Other programs include:<br />
• Stevens Place and Stewart Avenue (special needs housing)<br />
• Transitional housing<br />
• Programs for mother and child(ren), and father and child(ren)<br />
• Chemical dependency services<br />
Options for Southern <strong>Oregon</strong><br />
Online: http://www.optionsonline.org/<br />
Contact: 541-476-1526, 541-476-2373<br />
Programs: Affordable housing developer. Focus on programs and services for low-income<br />
individuals and people with psychiatric disabilities, in Josephine County.<br />
Other <strong>Housing</strong> and Related Resources<br />
Coos County Resource Guide<br />
Online: http://www.co.coos.or.us/ccf/ccfrg.pdf<br />
Contact: n/a<br />
Programs: Provides list <strong>of</strong> service agencies in Coos County.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-29<br />
Josephine County Community Action<br />
Online: n/a<br />
Contact: 541-474-5440<br />
Programs: Josephine County Community Action assists with Rental Assistance programs,<br />
energy assistance, food share, transportation, senior programs and information and<br />
referrals in Josephine County.<br />
Klamath County Resources Guide<br />
Online: http://www.klamathresources.org/services/index.asp<br />
Contact: n/a<br />
Programs: Provides list <strong>of</strong> service agencies in Klamath County.<br />
Klamath Lake Community Action Agency<br />
Online: n/a<br />
Contact: 541-850-5388<br />
Programs:<br />
<strong>Oregon</strong> Coast Community Action (ORCCA)<br />
Online: www.orcca.us<br />
Contact: Robert Moore, 541-888-7022, 541-888-7025<br />
Programs: Serves Coos County. Programs include rental listings, housing stabilization program,<br />
HOME TBRA program (up to 12 months), and supportive housing in partnership<br />
with Coos County Mental Health.<br />
Rogue Valley Community Development Corporation<br />
Online: http://www.rvcdc.com<br />
Contact: 541-734-2355<br />
Programs: RVCDC is primarily involved in the development <strong>of</strong> for-purchase affordable<br />
housing. RVCDC also works in coordination with the USDA Rural Development<br />
Self-Help program.<br />
Southwestern <strong>Oregon</strong> Community Action Committee (SWOCAC)<br />
Online: n/a<br />
Contact: 541-888-7016<br />
Programs:<br />
Umpqua Community Action Network (UCAN)<br />
Online: http://www.ucancap.org/<br />
Contact: 542-492-3501<br />
Programs: Affordable housing developer in Douglas and Josephine Counties. Other programs<br />
include weatherization and emergency rental or mortgage assistance.
A-30 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Region 4 Resources<br />
<strong>Housing</strong> Authorities<br />
<strong>Housing</strong> Works (Central <strong>Oregon</strong> Regional <strong>Housing</strong> Authority)<br />
Online: www.corha.org, www.oregonhousingworks.org<br />
Contact: 541-923-1018<br />
Programs: Provides 1,026 Section 8 vouchers, 48 public housing units and 395 low income<br />
housing units in Deschutes, Jefferson and Crook Counties. Section 8 wait list is<br />
currently closed. Other programs include:<br />
• Family Self-Sufficiency program<br />
• <strong>Housing</strong> Quest homeownership assistance program<br />
• Gateway Center, in Redmond, is a "one-stop shop" for employment services<br />
<strong>Housing</strong> Authority <strong>of</strong> Malheur County<br />
Online: n/a<br />
Contact: 541-889-9661, tjl@cableone.net, s8hamc@cableone.net<br />
Programs: Provides 349 Section 8 vouchers and 40 public housing units in Malheur and Harney<br />
Counties.<br />
Mid-Columbia <strong>Housing</strong> Authority<br />
Online: www.mid-columbiahousingauthority.org<br />
Contact: 541-296-5462, info@mid-columbiahousingauthority.org<br />
Programs: Provides 551 Section 8 vouchers in Wasco, Sherman and Hood River Counties.<br />
Northeast <strong>Oregon</strong> <strong>Housing</strong> Authority<br />
Online: neoha.oregonsearch.net<br />
Contact: 541-963-5360, neoha@uwtc.net<br />
Programs: Provides 710 Section 8 vouchers and 129 public housing units in Union, Baker,<br />
Grant and Wallowa Counties. Wait list is up to two years long. Other programs:<br />
• Family Self-Sufficiency program<br />
• Section 8 Homeownership program<br />
• Transitional housing program<br />
• <strong>Housing</strong> for individuals with mental illness<br />
<strong>Housing</strong> Authority <strong>of</strong> the County <strong>of</strong> Umatilla<br />
Online: www.umatillacountyha.org<br />
Contact: 541-567-3241, info@umatillacountyha.org, loretta1@uci.net
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-31<br />
Programs: Provides 329 Section 8 vouchers, 118 public housing units and more than 260 lowincome<br />
housing units in Umatilla, Morrow, Gilliam and Wheeler Counties.<br />
Regional <strong>Housing</strong> Centers<br />
Community Connections <strong>Housing</strong> Resource Center<br />
Online: www.admin.ccno.org/housingcenter.htm<br />
Contact: Sherri Becker, 541-963-3186, sherri@ccno.org<br />
Programs: Provides housing information and referrals in Baker, Grant, Union, and Wallowa<br />
Counties. Operated by CCNO (see listing below).<br />
Mid-Columbia <strong>Housing</strong> Resource Center<br />
Online: www.MidColumbia<strong>Housing</strong>Center.org<br />
Contact: John Hutchison, 541-296-5462, info@MidColumbia<strong>Housing</strong>Center.org<br />
Programs: Provides housing information and referrals in Hood River, Sherman & Wasco<br />
Counties. Operated by Columbia Cascade <strong>Housing</strong> Corp.<br />
NeighborImpact Homeownership Center<br />
Online: www.neighborimpact.org/homeownership.html<br />
Contact: 541-548-2380 x.109, 541-318-3302, homeownership@neighborimpact.org<br />
Programs: Provides housing information and referrals in Crook, Deschutes, and Jefferson<br />
Counties. Operated by NeighborImpact (see listing on following page).<br />
USDA Rural Development Offices<br />
USDA Rural Development, Pendleton Local Office<br />
Online: www.rurdev.usda.gov/OR/<br />
Contact: 541-278-8049<br />
Programs: Serves Baker, Gilliam, Grant, Malheur, Morrow, Umatilla, Union, and Wallowa<br />
Counties.<br />
USDA Rural Development, Redmond Local Office<br />
Online: www.rurdev.usda.gov/OR/<br />
Contact: 541-923-4358<br />
Programs: Serves Crook, Deschutes, Harney, Hood River, Jefferson, Sherman, Wasco, and<br />
Wheeler Counties.<br />
Affordable <strong>Housing</strong> Developers<br />
Community Connections <strong>of</strong> Northeast <strong>Oregon</strong> (CCNO)<br />
Online: www.admin.ccno.org/
A-32 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Contact: Margaret Davidson, 541-963-3186, 800-836-3186, margaret@ccno.org<br />
Programs: Affordable housing developer in Baker, Union, and Wallowa Counties. Other<br />
programs include:<br />
• Energy assistance<br />
• <strong>Housing</strong> rehabilitation<br />
• Food assistance<br />
NeighborImpact<br />
Online: www.neighborimpact.org/<br />
Contact: Corky Senecal, 541-548-2380 x101, corkys@neighborimpact.org<br />
541-317-1141 Bend<br />
541-416-0107 Prineville<br />
541-475-7017 Madras<br />
Programs: Affordable housing developer in Deschutes, Crook and Jefferson Counties. Other<br />
programs include:<br />
• Transitional housing<br />
• Group housing for single women<br />
• Emergency shelter for families<br />
• Emergency motel vouchers<br />
• Emergency utility assistance<br />
• Emergency rental assistance and eviction prevention<br />
Other <strong>Housing</strong> and Related Resources<br />
Beehive Cascades Referral Network<br />
Online: www.thebeehive.org/ (Select “Cascades” region under <strong>Oregon</strong>)<br />
Contact: n/a<br />
Programs: Information listings on services agencies in Crook, Deschutes, and Jefferson<br />
Counties.<br />
Bethlehem Inn<br />
Online: www.bethleheminn.org/<br />
Contact: 541-322-8768<br />
Programs: Offers a nightly shelter and support services for homeless persons in the City <strong>of</strong><br />
Bend. Accepts clean and sober men and women over the age <strong>of</strong> 18. Limited case<br />
management provided.<br />
CAP <strong>of</strong> East Central <strong>Oregon</strong> (CAPECO)<br />
Online: www.capeco-works.org/<br />
Contact: Pendleton: 541-276-1926, 541-276-5073
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-33<br />
Hermiston: 541-567-7889, 541-289-7755<br />
Programs: Serves Gilliam, Morrow, Umatilla, and Wheeler Counties. Programs include:<br />
• Emergency rental assistance<br />
• Home weatherization<br />
• Food assistance<br />
Cascade Youth and Family <strong>Services</strong><br />
Online: www.jbarj.org/CYFC/cyfc.html<br />
Contact: 541-382-0934, 1-800-660-0934<br />
Programs: Offers an emergency and transitional shelter in Deschutes and Jefferson Counties.<br />
Accepts homeless or at-risk youth between the ages <strong>of</strong> 12 and 20.<br />
Deschutes County Social <strong>Services</strong> Resource Guide<br />
Online: www.co.deschutes.or.us/go/living-here/social-services<br />
Contact: n/a<br />
Programs: Information listings on service agencies in Deschutes County.<br />
Harney-Malheur Community Action Agency (HMCAA)<br />
Online: n/a<br />
Contact: 541-573-6024<br />
Programs: Newest community action agency in <strong>Oregon</strong>.<br />
Madras Ministerial Association<br />
Online: n/a<br />
Contact: 541-475-2201<br />
Programs: Offers a limited number <strong>of</strong> one-night motel vouchers, hot meals, and auto fuel<br />
vouchers in the City <strong>of</strong> Madras.<br />
Mid-Columbia Community Action Council (MCCAC)<br />
Online: www.mccac.com<br />
Contact: 541-298-5131<br />
Programs: Programs in Wasco, Hood River and Sherman Counties, including:<br />
• Emergency rental assistance<br />
• Transitional housing<br />
• Home weatherization<br />
• Food assistance<br />
Redmond Ministerial Association<br />
Online: n/a<br />
Contact: 541-504-3400
A-34 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Programs: Offers a limited number <strong>of</strong> one-night motel vouchers, hot meals, and auto fuel<br />
vouchers in the City <strong>of</strong> Redmond only.<br />
Salvation Army<br />
Online: www.centormall.com/Salvation_Army/index.html<br />
Contact: 541-447-4168<br />
Programs: Offers a one-night motel voucher or food voucher for the grocery store.<br />
St. Vincent de Paul (Bend)<br />
Online: n/a<br />
Contact: 541-389-6643<br />
Programs: Offers a limited number <strong>of</strong> motel vouchers in the City <strong>of</strong> Bend.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-35<br />
Appendix 2: Stakeholder Survey Results<br />
This section includes a summary <strong>of</strong> a survey <strong>of</strong> housing and services providers administered by<br />
Building Changes as part <strong>of</strong> this systems integration planning process. The survey was distributed<br />
both to <strong>HIV</strong>/<strong>AIDS</strong> housing and services providers, and agencies that do not specifically target people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
Building Changes distributed an electronic survey to a list <strong>of</strong> stakeholders identified by the Steering<br />
Committee. Thirty-two total respondents completed the survey, including 16 respondents that<br />
identified their agencies as having a primary focus on serving people living with <strong>HIV</strong>/<strong>AIDS</strong>, and 16<br />
that did not. Seven respondents were from the <strong>Oregon</strong> <strong>Housing</strong> Opportunities in Partnership<br />
(OHOP) Region 1, seven from Region 2, eight from Region 3, eight from Region 4, and two from<br />
the Portland metropolitan area.<br />
Some questions were asked only <strong>of</strong> the <strong>HIV</strong>/<strong>AIDS</strong> providers, some were asked only <strong>of</strong> the<br />
providers that do not primarily focus on serving people living with <strong>HIV</strong>/<strong>AIDS</strong>, and some were<br />
asked <strong>of</strong> both groups. The following section summarizes survey responses.<br />
Question: What services are not available or insufficient in your region? (asked <strong>HIV</strong>/<strong>AIDS</strong> providers<br />
only)<br />
Gap %<br />
Transportation assistance 69%<br />
<strong>Housing</strong> assistance 63%<br />
Employment assistance 63%<br />
Food and nutritional assistance 50%<br />
Reentry transition assistance 50%<br />
Mental health care 38%<br />
Substance use treatment 38%<br />
Medical care 19%<br />
Case management 6%
A-36 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Question: What barriers do people living with <strong>HIV</strong>/<strong>AIDS</strong> in your area face in becoming stable and/or<br />
getting access to housing and other assistance? (asked <strong>HIV</strong>/<strong>AIDS</strong> providers only)<br />
Barrier %<br />
Lack <strong>of</strong> affordable housing 100%<br />
Lack <strong>of</strong> transportation 75%<br />
Lack <strong>of</strong> education or job training opportunities<br />
impacts ability to earn sufficient income<br />
Application process for housing and/or services is<br />
too slow or bureaucratic<br />
69%<br />
63%<br />
Not enough funding for support services 63%<br />
Restrictions on uses <strong>of</strong> funding 38%<br />
Lack <strong>of</strong> coordination / communication between<br />
providers<br />
Question: Please note the types <strong>of</strong> non-<strong>HIV</strong>/<strong>AIDS</strong> agencies that your organization coordinates or<br />
partners with. (asked <strong>HIV</strong>/<strong>AIDS</strong> providers only)<br />
31%<br />
Partners %<br />
Food assistance agencies 81%<br />
<strong>Housing</strong> agencies 75%<br />
Chemical dependency agencies 69%<br />
Mental health agencies 69%<br />
Criminal justice / corrections agency 63%<br />
Hospital 63%<br />
Employment services agency 44%<br />
Homeless services agency 44%<br />
Veterans agency 25%<br />
Question: If you partner with a housing agency or agencies, which type(s) <strong>of</strong> agencies? (asked<br />
<strong>HIV</strong>/<strong>AIDS</strong> providers only)<br />
<strong>Housing</strong> Partners %<br />
<strong>Housing</strong> authority 56%<br />
Landlord or property management firm 50%<br />
Affordable or supportive housing developer 44%<br />
Halfway house 13%<br />
Regional <strong>Housing</strong> Center 6%
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-37<br />
Question: Does your agency have partnerships with <strong>HIV</strong>/<strong>AIDS</strong> providers? (asked non-<strong>HIV</strong>/<strong>AIDS</strong><br />
providers only)<br />
Partner with <strong>HIV</strong>/<strong>AIDS</strong> Agencies? %<br />
Yes 50%<br />
No 44%<br />
Don’t Know 6%<br />
Question: Does your organization partner with other agencies or programs for any <strong>of</strong> the following<br />
services? (asked non-<strong>HIV</strong>/<strong>AIDS</strong> providers only)<br />
Partners %<br />
<strong>Housing</strong> services 75%<br />
Mental health services 69%<br />
Chemical dependency services 63%<br />
Medical care and health services 56%<br />
Employment services 50%<br />
Reentry or transition services 44%<br />
Question: Does your agency participate in the following housing and services planning processes?<br />
(asked all agencies)<br />
% <strong>of</strong> <strong>HIV</strong><br />
Providers<br />
71%<br />
Planning Process<br />
Ryan White program planning (including<br />
<strong>Oregon</strong> <strong>HIV</strong> Care Coalition)<br />
% <strong>of</strong> Non-<strong>HIV</strong><br />
Providers<br />
19%<br />
13% Continuum <strong>of</strong> Care 50%<br />
13% 10 Year Plans to End Homelessness 50%<br />
7% Consolidated Plan 44%<br />
Question: How well do the following planning processes include consideration <strong>of</strong> the housing and<br />
services needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong>? (asked all agencies)<br />
Planning Process<br />
Qualified Allocation Plan<br />
(LIHTC)<br />
Don’t<br />
Know<br />
Not Well<br />
Fairly<br />
Well<br />
Very Well or<br />
Extremely<br />
Well<br />
82% 11% 4% 4%<br />
Continuum <strong>of</strong> Care 67% 17% 7% 10%<br />
Consolidated Plan 64% 11% 18% 7%<br />
10 Year Plans to End<br />
Homelessness<br />
62% 21% 14% 3%
A-38 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Question: Please rate your agency’s staff’s ability to refer clients with <strong>HIV</strong>/<strong>AIDS</strong> to the resources that<br />
they need, on a scale from one (not confident) to four (extremely confident). (asked all agencies)<br />
Non-<strong>HIV</strong>/<strong>AIDS</strong> providers rated their confidence lower (2.5) than <strong>HIV</strong>/<strong>AIDS</strong> providers (3.4). The<br />
lowest scores were in Region 4, especially from non-<strong>HIV</strong>/<strong>AIDS</strong> agencies in the Bend area.<br />
Question: What types <strong>of</strong> agencies or stakeholders would you like to see more involved in efforts to<br />
improve the systems integration <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> housing and services? (asked all agencies)<br />
Stakeholders %<br />
Affordable housing agencies 88%<br />
<strong>Housing</strong> authorities 69%<br />
Mental health agencies 63%<br />
Homeless services agencies 56%<br />
Employment services agencies 56%<br />
Chemical dependency agencies 50%<br />
Hospitals and health agencies 50%<br />
Elected <strong>of</strong>ficials 47%<br />
Criminal justice / corrections agencies 44%<br />
Questions: What outcomes are the highest priorities for systems integration to meet the needs <strong>of</strong><br />
people living with <strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong>? (asked all agencies)<br />
Goals <strong>of</strong> <strong>Systems</strong> Integration %<br />
Create more housing opportunities for people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong> (PLWHA)<br />
78%<br />
Improve access to support services for PLWHA 78%<br />
Increase economic self-sufficiency <strong>of</strong> PLWHA 69%<br />
Increase public awareness <strong>of</strong> the needs <strong>of</strong><br />
PLWHA<br />
Increase access to mainstream federal services<br />
(food stamps, SSI/SSDI, etc.)<br />
Improve discharge planning form correctional<br />
facilities and hospitals<br />
Questions: What is the biggest challenge to improving systems integration for people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> in <strong>Oregon</strong>? (asked all agencies)<br />
Non-<strong>HIV</strong>/<strong>AIDS</strong> providers listed insufficient funding for systems integration work as the biggest<br />
challenge to improving systems integration for PLWHA. <strong>HIV</strong>/<strong>AIDS</strong> agencies listed lack <strong>of</strong> staff time<br />
to do systems integration work as the biggest challenge. The chart on the following page shows the<br />
aggregate <strong>of</strong> all responses.<br />
56%<br />
56%<br />
47%
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-39<br />
Stakeholders %<br />
Insufficient funding for systems integration work 72%<br />
Not enough staff time to devote to systems integration work 59%<br />
Lack <strong>of</strong> interest from non-<strong>HIV</strong>/<strong>AIDS</strong> providers 44%<br />
Incompatibility <strong>of</strong> funding sources 31%<br />
Lack <strong>of</strong> government interest 25%
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-41<br />
Appendix 3: <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> Options<br />
This section describes each <strong>HIV</strong>/<strong>AIDS</strong> housing continuum type and its relative advantages and<br />
disadvantages. In addition, eligible HOPWA activities within each housing assistance type are<br />
noted. HOPWA may be used to fund some <strong>of</strong> these activities if approved within the Consolidated<br />
Plan or grant agreements.<br />
These housing assistance program options are included for reference for the reader and for future<br />
program planning.<br />
Generally, <strong>HIV</strong>/<strong>AIDS</strong> housing needs fall into an overall, community-wide housing continuum. This<br />
continuum, which provides a comprehensive way <strong>of</strong> evaluating a community’s resources, divides housing<br />
needs and resources into the following categories, each <strong>of</strong> which are explained in detail in this section:<br />
• Emergency <strong>Housing</strong> Assistance<br />
• Transitional <strong>Housing</strong> Assistance<br />
• Permanent <strong>Housing</strong> Assistance<br />
• <strong>Services</strong> to Support <strong>Housing</strong> Stability<br />
There are many different methods for delivering each <strong>of</strong> the above housing services. The charts in this<br />
section outline many <strong>of</strong> the housing solutions for each category <strong>of</strong> housing services, and summarize the<br />
advantages and disadvantages <strong>of</strong> each program type. Please note that many different funding sources may be<br />
required to establish any <strong>of</strong> these programs, and that each funding source may have restrictions that disallow<br />
certain program activities.<br />
In addition, many <strong>of</strong> the best housing resources for people living with <strong>HIV</strong>/<strong>AIDS</strong> are provided by<br />
mainstream organizations that serve a wide variety <strong>of</strong> people. It is usually faster, cheaper, and more<br />
appropriate to draw on mainstream housing resources than to create new facilities and services just for<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong>. Training other providers to understand the special needs <strong>of</strong> people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong> can provide the same result as, and <strong>of</strong>ten more efficiently than, providing a new service tailored<br />
to specific needs. New <strong>HIV</strong>/<strong>AIDS</strong> housing programs should focus on filling gaps not covered by other<br />
community resources or adapting mainstream resources to meet the needs <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong>.
A-42 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Emergency <strong>Housing</strong> Assistance<br />
Very short-term assistance provided to address an immediate housing crisis for those who are homeless or at imminent risk.<br />
GOALS & DESCRIPTIONS<br />
Assistance to help households facing a<br />
crisis that could result in displacement<br />
from their housing<br />
Best where financial crises can be<br />
overcome with short-term assistance<br />
For use when no alternative exists but<br />
living on streets or in substandard/inappropriate<br />
housing<br />
Best when local waiting lists for<br />
affordable housing are relatively short,<br />
and people can transition relatively<br />
quickly<br />
Basic, temporary, overnight sleeping<br />
accommodation<br />
Best where significant homeless<br />
population and much affordable<br />
transitional & permanent housing is<br />
available as a next step<br />
ASSISTANCE TYPES &<br />
HOPWA–ELIGIBLE USES<br />
STRMU (Short Term Rent,<br />
Mortgage, Utility)<br />
- Limited to 21/52 weeks, only<br />
for people who are already<br />
housed<br />
Hotel-Motel Voucher<br />
(considered Supportive<br />
<strong>Services</strong>)<br />
- Last resort; need reasonable<br />
rates<br />
Emergency Shelter<br />
- Stays limited to 60/180 days in<br />
facilities housing 50 or fewer<br />
- Can fund facility operations<br />
- Can fund acquisition, rehab, etc.<br />
ADVANTAGES DISADVANTAGES<br />
- Easier than developing new<br />
housing options<br />
- Can serve many households<br />
with limited funding<br />
- Pay once or twice<br />
- Useful where many in need are<br />
homeowners<br />
- Usually available immediately<br />
- Simple to administer<br />
- Can be used for families or<br />
people too sick for shelter<br />
- Can serve as bridge to other<br />
solutions when subsidy wait lists<br />
are short<br />
- Immediate response<br />
- Can be cost-effective<br />
- Often first point <strong>of</strong> contact for<br />
newly homeless<br />
- Does not create long-term<br />
housing<br />
- Does not address needs <strong>of</strong><br />
homeless<br />
- Many need ongoing assistance to<br />
stay in home<br />
- May be costly<br />
- Not home-based housing – no<br />
cooking facilities or refrigeration,<br />
less privacy for family members<br />
- Hotels/motels that will<br />
participate may be in unsafe<br />
neighborhoods<br />
- Not long-term solution<br />
- Out during day<br />
- Shared space <strong>of</strong>fers little privacy,<br />
refrigeration access<br />
- May be unsanitary / unhealthy<br />
- Few accommodations for<br />
families<br />
- Not long-term solution
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-43<br />
Transitional <strong>Housing</strong> Assistance<br />
Limited duration housing assistance – usually 30 days to 2 years – intended to help people transition from housing crisis into permanent, stable<br />
housing. Effective where consumers are likely to become self-sufficient or transition to permanent housing by the time it ends.<br />
GOALS & DESCRIPTIONS<br />
Assistance for more than 1 or 2<br />
payments. Based on income and<br />
FMR; <strong>of</strong>ten lasts up to 2 yrs<br />
Best where consumers remain in<br />
housing while waiting for subsidy;<br />
and can transition to permanent<br />
housing within time limit<br />
Temporary housing plus support<br />
services to help people overcome<br />
problems that led to homelessness<br />
and return to permanent<br />
independent housing<br />
Best where homeless population is<br />
significant and support services are<br />
in place<br />
ASSISTANCE TYPES &<br />
HOPWA–ELIGIBLE USES<br />
Tenant-Based Transitional<br />
<strong>Housing</strong> Assistance<br />
- Monthly rental assistance<br />
payments for people on wait lists<br />
- HUD housing quality standards<br />
apply<br />
Supportive Transitional <strong>Housing</strong><br />
- Can fund facility operations<br />
- Can fund acquisition, rehab, etc.<br />
ADVANTAGES DISADVANTAGES<br />
- Tenants can choose housing<br />
location<br />
- Can prevent homelessness for<br />
people waiting for permanent<br />
housing<br />
- Can be implemented quickly –<br />
less complex than facility-based<br />
assistance<br />
- Can promote long-term stability<br />
even after clients leave<br />
- Provides leverage (conditions <strong>of</strong><br />
residency) to ensure that clients<br />
benefit from support services<br />
- Does not create long-term housing<br />
- Some landlords unwilling<br />
- Does not include support services<br />
that some may need to retain<br />
housing<br />
- Sometimes not enough quality<br />
rental units at FMR<br />
- Support services costly<br />
- To achieve success, clients must<br />
be able to access permanent<br />
affordable housing supply after<br />
leaving
A-44 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
Permanent <strong>Housing</strong> Assistance<br />
Safe, stable, decent long-term housing opportunities with or without support services.<br />
GOALS & DESCRIPTIONS<br />
Ongoing assistance to cover difference<br />
between market rents (or FMR) and<br />
30% <strong>of</strong> tenant’s household income, for<br />
as long as income falls below<br />
qualifying standard<br />
Best administered by partners: housing<br />
authority willing to administer the<br />
subsidy and service organization<br />
willing to market subsidies, prescreen<br />
tenants, and help them find<br />
appropriate units<br />
Rent or mortgage subsidies based on a<br />
smaller, fixed amount, rather than the<br />
difference between FMR and 30% <strong>of</strong><br />
tenant’s household income<br />
Best when housing costs are level, and<br />
consumers are close to being able to<br />
afford housing independently<br />
ASSISTANCE TYPES &<br />
HOPWA–ELIGIBLE USES<br />
Tenant-Based Rental<br />
Assistance (TBRA)<br />
Monthly rental assistance<br />
payments<br />
HUD $ formula and housing<br />
standards apply<br />
Shallow Rent/Mtge Subsidy<br />
(TBRA)<br />
Not HOPWA-eligible except by<br />
special approval for a<br />
competitive grant<br />
ADVANTAGES DISADVANTAGES<br />
- Local discretion for housing<br />
undocumented immigrants and<br />
people with criminal histories<br />
-Tenants pay only 30% <strong>of</strong> their<br />
income and choose housing<br />
location<br />
- Can be used in existing units<br />
- Some HAs give Section 8<br />
preference to people with<br />
terminal illnesses or w/<br />
HOPWA rental assistance<br />
-Easier than housing<br />
development<br />
- Tenants can choose housing<br />
location or remain in current<br />
homes<br />
- Can serve many households<br />
with limited funding<br />
- Can be implemented quickly –<br />
less complex than facility-based<br />
assistance<br />
-Does not create long-term housing<br />
- Some landlords unwilling<br />
- Does not include support services<br />
that some may need to retain housing<br />
- Sometimes not enough quality rental<br />
units at FMR<br />
- Available properties may be in<br />
unsafe neighborhoods<br />
-Funding for many TBRA programs<br />
can be limited to 3-5 years and<br />
difficult to renew<br />
- Few funding sources allow this<br />
activity<br />
- Does not create long-term housing<br />
- Does not provide enough assistance<br />
for many
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-45<br />
GOALS & DESCRIPTIONS<br />
Negotiated set-asides <strong>of</strong> units for<br />
PLWHA in mainstream affordable<br />
housing projects<br />
Best in projects already developed<br />
with rents affordable to PLWHA, or<br />
when <strong>AIDS</strong> service organizations can<br />
contribute debt-free funding (such as<br />
HOPWA)<br />
A long-term lease agreement with a<br />
property manager in which a service<br />
organization funds a rent reserve to<br />
pay the difference between market rent<br />
and the amount that consumers can<br />
pay<br />
Best when market rents are not<br />
affordable and landlords are willing to<br />
enter long-term agreements<br />
A service organization leases units that<br />
are then sub-leased at an affordable<br />
cost to PLWHA<br />
Best in communities with active rental<br />
markets in healthy neighborhoods with<br />
access to support services<br />
ASSISTANCE TYPES &<br />
HOPWA–ELIGIBLE USES<br />
Set-Asides in Other <strong>Housing</strong><br />
Projects<br />
- Can fund acquisition, rehab,<br />
etc. (new construction for SRO<br />
and group homes only)<br />
-Can fund facility operations<br />
Lease Buy-Downs<br />
- Rent reserves are not<br />
HOPWA-eligible<br />
- Can fund monthly lease,<br />
operations, and repair costs<br />
Master Leasing<br />
-Can fund monthly lease,<br />
operations, and repair costs<br />
ADVANTAGES DISADVANTAGES<br />
- Can help experienced<br />
developers to create new longterm<br />
housing capacity<br />
- Can be quicker and more<br />
economically efficient than<br />
dedicated development<br />
- Can be long-term<br />
- Residents can integrate into<br />
community<br />
- Can be economically efficient<br />
and ensure stability without<br />
ongoing subsidy<br />
- Less complex than facilitybased<br />
assistance<br />
- Residents can integrate into the<br />
community<br />
- Can allow organizations to<br />
place consumers quickly<br />
- Community acceptance issues<br />
can <strong>of</strong>ten be avoided<br />
- Residents can integrate into the<br />
community<br />
- <strong>Housing</strong> providers’ rules may<br />
disqualify some consumers<br />
- Some providers not willing to set<br />
aside units, or legally constrained<br />
- Only effective when rents are<br />
affordable<br />
- Physical design and operations may<br />
not accommodate health needs <strong>of</strong><br />
PLWHA<br />
- Usually requires lump sum to fund<br />
entire rent reserve up front; cost may<br />
be high<br />
- Developing contracts can be<br />
complicated and time-consuming<br />
- Funders may prefer ownership to<br />
long-term lease, or set different<br />
commitment periods<br />
- Property managers may not wish to<br />
enter into long-term leases<br />
- <strong>Housing</strong> providers’ rules may<br />
disqualify some consumers<br />
- Operating subsidies usually needed<br />
for each unit<br />
- Available properties may be in<br />
unsafe neighborhoods<br />
- When necessary, displacing tenants<br />
can be complicated and expensive<br />
- <strong>Housing</strong> conditions must be<br />
carefully assessed, and close landlord<br />
relationship maintained
A-46 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
GOALS & DESCRIPTIONS<br />
A service organization purchases<br />
condominiums or single-family homes<br />
and leases the units to PLWHA<br />
Best in communities with active<br />
housing markets and networks that can<br />
deliver services to dispersed<br />
populations<br />
Congregate living assistance ranging<br />
from a group home owned by a service<br />
organization to a housemate referral<br />
service<br />
Best where consumer preference<br />
indicates sufficient demand to keep<br />
beds filled<br />
Independent apartment projects to<br />
meet the permanent housing needs <strong>of</strong><br />
PLWHA, or to serve a mixed<br />
population that includes PLWHA<br />
Best where consumer preference<br />
indicates sufficient demand to keep<br />
units filled<br />
ASSISTANCE TYPES &<br />
HOPWA–ELIGIBLE USES<br />
Scattered Site Acquisition<br />
- Can fund acquisition, rehab,<br />
etc. (new construction for SRO<br />
and group homes only)<br />
Group Homes/Shared Living<br />
- Can fund acquisition, rehab,<br />
etc.<br />
- Can fund facility operations<br />
Independent Apartment<br />
Development Projects<br />
- Can fund acquisition, rehab,<br />
etc. (new construction for SRO<br />
and group homes only)<br />
- Can fund monthly lease,<br />
operations, and repair costs<br />
ADVANTAGES DISADVANTAGES<br />
- Can allow quick access to<br />
housing, relative to construction<br />
- Can effectively meet scattered<br />
demand<br />
- A small number <strong>of</strong> units can be<br />
developed efficiently<br />
- Residents can integrate into the<br />
community<br />
- Can be less expensive than<br />
individual apartments<br />
- Can <strong>of</strong>fer peer support<br />
- Various organizations can<br />
sponsor individual rooms<br />
- Creates new long-term housing<br />
capacity<br />
- Offers owner most control, or<br />
opportunities to partner with<br />
other organizations<br />
- Units can be developed to<br />
address specific needs<br />
- Large development projects<br />
can increase an organization’s<br />
capacity to raise private<br />
donations and grants<br />
- Creates new long-term housing<br />
capacity<br />
- Can require complicated property<br />
management<br />
- Operating subsidies may be needed<br />
to keep rents affordable<br />
- Condominiums can require monthly<br />
maintenance fees and other costs;<br />
<strong>of</strong>fer less control than traditional<br />
ownership; and place restrictions on<br />
residents<br />
- Most consumers prefer independent<br />
living; many prefer not to live in<br />
<strong>HIV</strong>/<strong>AIDS</strong>-dedicated facilities<br />
- If demand drops, difficult to convert<br />
facility to new use<br />
- Can be difficult to manage conflicts<br />
between housemates and to preserve<br />
confidentiality<br />
- Expensive, complex, and timeconsuming<br />
- Multifamily-zoned land can be hard<br />
to find<br />
- Can attract community opposition<br />
- Number <strong>of</strong> units needed for<br />
economic efficiency may be greater<br />
than local demand for <strong>AIDS</strong> housing<br />
- Many consumers prefer not to live<br />
in <strong>HIV</strong>/<strong>AIDS</strong>-dedicated facilities<br />
- Requires long-term commitment<br />
and operating subsidies
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-47<br />
GOALS & DESCRIPTIONS<br />
Short- and long-term housing<br />
combined with services designed to<br />
assist people whose health makes<br />
independent living impossible<br />
Best where there is a large<br />
concentration <strong>of</strong> PLWHA who require<br />
higher-end care<br />
ASSISTANCE TYPES &<br />
HOPWA–ELIGIBLE USES<br />
Specialized Care Facilities<br />
- Can fund acquisition,<br />
rehab, etc.<br />
- Can fund facility operations<br />
ADVANTAGES DISADVANTAGES<br />
- Can provide a high level <strong>of</strong><br />
care for people whose medical<br />
or behavioral health does not<br />
allow them to live<br />
independently, as an alternative<br />
to hospitalization<br />
- Very expensive, due to skilled<br />
staffing needs<br />
- Consumers living longer prefer not<br />
to live in specialized care facilities<br />
- Only possible in areas with a large<br />
concentration <strong>of</strong> PLWHA
A-48 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
<strong>Services</strong> to Support <strong>Housing</strong> Stability<br />
One-time assistance for move-in or occupancy or ongoing services to support housing stability<br />
GOALS & DESCRIPTIONS<br />
Supportive services <strong>of</strong>fered as a<br />
complement to housing, such as<br />
case management, health care or<br />
treatment, food and transportation<br />
assistance, etc.<br />
Should be an integral part <strong>of</strong> every<br />
housing solution. Requires good<br />
referral arrangements with other<br />
service providers<br />
Assists households in overcoming<br />
the one-time challenges <strong>of</strong><br />
establishing a new residence<br />
Essential where homeless people<br />
are transitioning into permanent<br />
housing<br />
ASSISTANCE TYPES &<br />
HOPWA–ELIGIBLE USES<br />
Support <strong>Services</strong>*<br />
- <strong>Services</strong> including housing<br />
advocacy, home care, counseling,<br />
nutrition and meal services, crisis<br />
intervention, legal assistance,<br />
transportation, day health<br />
programs, mental health services,<br />
personal assistance, and substance<br />
use treatment<br />
- Can be <strong>of</strong>fered with or without<br />
housing<br />
Move-In/Occupancy Needs<br />
Assistance*<br />
- First month’s rent, deposits and<br />
tenant screening fees up to the<br />
value <strong>of</strong> 2 mos. rent under<br />
HOPWA supportive services<br />
category, permanent housing<br />
placement activity<br />
ADVANTAGES DISADVANTAGES<br />
- Can help tenants remain in their<br />
home<br />
- Existing providers and volunteer<br />
teams can contribute<br />
- Less complex than facility-based<br />
assistance; few start-up costs<br />
required<br />
- Relatively inexpensive<br />
- Easy to administer<br />
- Volunteer teams and local<br />
businesses can contribute<br />
- Some consumers will also need<br />
financial assistance to keep<br />
housing.<br />
- Providing services in widely<br />
scattered locations can be<br />
expensive<br />
- Securing ongoing funding can be<br />
difficult<br />
- Many need more assistance<br />
- Deposits may be kept by landlords<br />
or departing tenants
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-49<br />
Appendix 4: Federal and <strong>State</strong> Financing Sources<br />
for Affordable <strong>Housing</strong><br />
This section provides information on financing affordable housing for people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
Contact information for grant administrators in the <strong>Oregon</strong> balance <strong>of</strong> state is available the<br />
Affordable <strong>Housing</strong> Resource Guide in Appendix 1.<br />
This section provides brief descriptions <strong>of</strong> programs for financing for affordable housing, many <strong>of</strong> which<br />
were referenced in the body <strong>of</strong> this <strong>Systems</strong> Integration Plan. Because housing is expensive to develop and<br />
operate, especially when enriched with support services, and because people living with <strong>HIV</strong>/<strong>AIDS</strong> may<br />
have very little income available to pay for rent and services, <strong>Housing</strong> Opportunities for Persons with <strong>AIDS</strong><br />
(HOPWA) funds alone are not sufficient to develop and operate housing.<br />
An essential component <strong>of</strong> HOPWA program grants management is the use <strong>of</strong> grant funds to leverage<br />
additional resources to increase housing opportunities for people living with <strong>HIV</strong>/<strong>AIDS</strong>. Nationally, HUD<br />
estimates that every HOPWA program dollar is leveraged by more than two dollars <strong>of</strong> other funding to<br />
support people living with <strong>HIV</strong>/<strong>AIDS</strong>. For every HOPWA program dollar that is allocated to housing<br />
development, more than five dollars <strong>of</strong> other funding is utilized for <strong>HIV</strong>/<strong>AIDS</strong> housing programs.<br />
The list below is not exhaustive, but it comprises some <strong>of</strong> the larger programs and those most directly related<br />
to housing people living with <strong>HIV</strong>/<strong>AIDS</strong>. More information and resources on financing affordable housing<br />
are available through the Building Changes / <strong>AIDS</strong> <strong>Housing</strong> <strong>of</strong> Washington website (www.aidshousing.org)<br />
and the Corporation for Supportive <strong>Housing</strong> website (www.csh.org/financing).<br />
U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development (HUD)<br />
Regional Contacts<br />
HUD Region X, Seattle Regional Office<br />
Regional Director<br />
John Meyers<br />
909 1st Avenue, Suite 200<br />
Seattle, WA 98104-1000<br />
(877) 741-3281<br />
HUD Field Office, Portland<br />
Field Office Director<br />
Roberta Ando<br />
Community Planning and Development Director<br />
Doug Carlson<br />
400 SW Sixth Ave., #700<br />
Portland, OR 97204<br />
(971) 222-2600
A-50 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
HUD Consolidated Plan Programs<br />
HUD requires a single, consolidated submission process, including all <strong>of</strong> the planning, application, and<br />
performance assessment documentation for the following formula programs:<br />
• Community Development Block Grants (CDBG)<br />
• Emergency Shelter Grants (ESG)<br />
• HOME Investment Partnerships Program (HOME)<br />
• <strong>Housing</strong> Opportunities for Persons with <strong>AIDS</strong> (HOPWA)<br />
<strong>State</strong>s, large cities, and urban counties that get any <strong>of</strong> these grants must have a Consolidated Plan (Con Plan).<br />
This planning process is intended to help local jurisdictions develop a vision for housing and community<br />
development and to coordinate their activities. Local governments develop the plan in consultation with<br />
public and private agencies that provide supportive housing and social and health services, community<br />
members, and neighboring localities, and Public <strong>Housing</strong> Authority (PHA) Plans must be consistent with the<br />
Con Plan. The Con Plan must indicate the activities that will be carried out in the coming year to address<br />
emergency shelter and transitional housing needs, homelessness prevention, the transition to permanent<br />
housing and independent living, and services for people who are not homeless but have supportive housing<br />
needs.<br />
Community Development Block Grant (CDBG)<br />
http://www.hud.gov/<strong>of</strong>fices/cpd/communitydevelopment/programs/<br />
CDBG program funds may be used in a variety <strong>of</strong> ways to support community development, including the<br />
acquisition, construction, and rehabilitation <strong>of</strong> public facilities and housing. However, communities are not<br />
required to include housing when determining how they would like to use CDBG funds.<br />
All CDBG-funded activities must address one <strong>of</strong> the three national objectives <strong>of</strong> the program:<br />
1. Benefit low- and moderate-income people.<br />
2. Eliminate or prevent slums or blight.<br />
3. Meet other urgent community development needs, where existing conditions pose a serious and<br />
immediate threat to the health and welfare <strong>of</strong> the community, and no other financial resources are<br />
available.<br />
Emergency Shelter Grants (ESG) Program<br />
http://www.hud.gov/<strong>of</strong>fices/cpd/homeless/programs/esg/<br />
The ESG Program funds are designated to improve the quality <strong>of</strong> existing emergency shelters and transitional<br />
housing for homeless people, to help create additional emergency shelters, to pay for certain operating and<br />
social service expenses in connection with homeless shelters, and for homeless prevention activities.<br />
HOME Investment Partnerships Program (HOME)<br />
http://www.hud.gov/<strong>of</strong>fices/cpd/affordablehousing/programs/home/<br />
Communities have the flexibility to use HOME funds for the housing activities that best meet local needs and<br />
priorities. Uses can include property acquisition, rehabilitation, site improvements, demolition, new
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-51<br />
construction, and tenant-based rental assistance. Assistance can take the form <strong>of</strong> loans, advances, equity<br />
investments, interest subsidies, and others. A portion (at least 15 percent) <strong>of</strong> HOME funds must be set aside<br />
for community housing development organizations (CHDOs), which are nonpr<strong>of</strong>it organizations that meet<br />
certain HUD-established criteria.<br />
<strong>Housing</strong> Opportunities for Persons with <strong>AIDS</strong> (HOPWA)<br />
http://www.hud.gov/<strong>of</strong>fices/cpd/aidshousing/programs/<br />
The HOPWA program is also part <strong>of</strong> the Consolidated Plan process. HOPWA provides grant funds to state<br />
and local governments to design long-term, comprehensive strategies for meeting the housing needs <strong>of</strong> lowincome<br />
people living with <strong>HIV</strong>/<strong>AIDS</strong> and their families. Participating jurisdictions have the flexibility to<br />
create a range <strong>of</strong> housing programs, including housing information services, resource identification, project-<br />
or tenant-based rental assistance, short-term rent, mortgage, and utility payments to prevent homelessness,<br />
development and housing operations, and support services. Ninety percent <strong>of</strong> HOPWA funds are awarded<br />
through formula entitlement grants, and the remaining 10 percent are awarded through a competitive grant<br />
program.<br />
HOPWA Formula Grants<br />
HUD awards 75 percent <strong>of</strong> HOPWA Formula Grant funds to eligible states and qualifying cities. Eligibility<br />
is based on the number <strong>of</strong> cases <strong>of</strong> <strong>AIDS</strong> reported by the Centers for Disease Control and Prevention as <strong>of</strong><br />
March 31 <strong>of</strong> the year prior to the appropriation. Eligible metropolitan statistical areas (EMSAs) and states<br />
receive direct allocations <strong>of</strong> HOPWA funding when 1,500 cumulative cases <strong>of</strong> <strong>AIDS</strong> are diagnosed in a<br />
region. The remaining 25 percent <strong>of</strong> funds is allocated among metropolitan areas that have had a higher than<br />
average per capita incidence <strong>of</strong> <strong>AIDS</strong>.<br />
HOPWA formula entitlement grantees may carry out eligible programs themselves, deliver them through any<br />
<strong>of</strong> their administrative entities, select or competitively solicit project sponsors, and/or contract with service<br />
providers.<br />
HOPWA Competitive Grants<br />
Competitive grants are awarded in the following categories:<br />
• Special Projects <strong>of</strong> National Significance (SPNS). Because <strong>of</strong> their innovation or ability to be<br />
replicated, these projects are intended to be models for addressing the needs <strong>of</strong> low-income people<br />
living with <strong>HIV</strong>/<strong>AIDS</strong> and their families.<br />
• Long-Term Comprehensive Strategies for Providing <strong>Housing</strong> and Related <strong>Services</strong>.<br />
Applications in this category can be submitted by state or local governments that are not eligible for<br />
HOPWA formula allocations during that fiscal year.<br />
HUD Homeless Assistance Continuum <strong>of</strong> Care<br />
In order to encourage the integration and coordination <strong>of</strong> community homeless assistance, HUD’s primary<br />
homeless assistance programs—Supportive <strong>Housing</strong> Program, Shelter Plus Care, Emergency Shelter Grants<br />
(ESG – which is also included in the Consolidated Plan), and Single Room Occupancy Program (formerly<br />
Section 8 SRO Mod. Rehab.)—are combined under the Continuum <strong>of</strong> Care planning and allocation process.<br />
The Continuum <strong>of</strong> Care system includes four components: outreach to and needs assessment <strong>of</strong> individuals<br />
or families who are homeless, emergency shelters with supportive services, transitional housing with support<br />
services, and permanent independent or supportive housing to meet long-term needs. The establishment <strong>of</strong> a<br />
Continuum <strong>of</strong> Care system involves a community-wide or region-wide process involving nonpr<strong>of</strong>it
A-52 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
organizations (including those representing persons with <strong>AIDS</strong> and other disabilities), government agencies,<br />
other homeless providers, housing developers and service providers, private foundations, neighborhood<br />
groups, and homeless or formerly homeless individuals. It is very important for applicants to understand that<br />
funding for the Supportive <strong>Housing</strong> Program, Shelter Plus Care, and Single Room Occupancy projects must<br />
be applied for within the context <strong>of</strong> the Continuum <strong>of</strong> Care process.<br />
Supportive <strong>Housing</strong> Program (SHP)<br />
http://www.hud.gov/<strong>of</strong>fices/cpd/homeless/programs/shp/<br />
SHP program funds are used to provide supportive housing, either as transitional housing for homeless<br />
people or permanent housing for homeless people who have disabilities, including people living with<br />
<strong>HIV</strong>/<strong>AIDS</strong>. In addition, SHP funds can also be used for safe havens, which provide specialized permanent<br />
housing for severely mentally ill homeless persons who have been unwilling to participate in support services<br />
as well as support services for people not living in supportive housing, and other innovative supportive<br />
housing models. SHP funds can be used for a range <strong>of</strong> activities from land acquisition to administrative<br />
expenses.<br />
Shelter Plus Care (S+C)<br />
http://www.hud.gov/<strong>of</strong>fices/cpd/homeless/programs/splusc/<br />
The Shelter Plus Care program provides rental assistance for permanent housing, linked with support<br />
services funded by other sources, to homeless and disabled people and their families. Activities under Shelter<br />
Plus Care include tenant-based rental assistance, project-based rental assistance, sponsor-based rental<br />
assistance, and moderate rehabilitation assistance for single room occupancy dwellings through the Single<br />
Room Occupancy Program described below.<br />
Single Room Occupancy Program (Section 8 SRO Mod. Rehab.)<br />
http://www.hud.gov/<strong>of</strong>fices/cpd/homeless/programs/sro/<br />
Under the <strong>Housing</strong> Choice Voucher Single Room Occupancy Program (formerly the Section 8 Moderate<br />
Rehabilitation Program for Single Room Occupancy Dwellings), HUD contracts with public housing<br />
authorities (PHAs) to enable the moderate rehabilitation 1 <strong>of</strong> residential properties that, when completed, will<br />
contain multiple single room dwelling units. The PHAs make rental assistance payments to the landlords on<br />
behalf <strong>of</strong> the homeless individuals who rent the rehabilitated dwellings, covering the difference between a<br />
portion <strong>of</strong> the tenant’s income (normally 30 percent) and the HUD-established Fair Market Rent <strong>of</strong> the unit.<br />
The program does not provide financing for the rehabilitation work, but a portion <strong>of</strong> this cost is reflected in<br />
the rent.<br />
Other HUD Programs<br />
HUD has many other programs, but three are particularly relevant when developing housing for people living<br />
with <strong>HIV</strong>/<strong>AIDS</strong>: Section 811 - Supportive <strong>Housing</strong> for Persons with Disabilities; the <strong>Housing</strong> Choice<br />
Voucher Program (formerly Section 8); and the <strong>Housing</strong> Choice Voucher Mainstream Disabilities Program.<br />
1 HUD considers moderate rehabilitation to be a minimum <strong>of</strong> $3,000 <strong>of</strong> rehabilitation work per unit.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-53<br />
Section 811 - Supportive <strong>Housing</strong> for Persons with Disabilities<br />
http://www.hud.gov/<strong>of</strong>fices/hsg/mfh/progdesc/disab811.cfm<br />
Nonpr<strong>of</strong>it organizations can use Section 811 funds to construct, acquire, and/or rehabilitate supportive<br />
housing for very low-income persons with disabilities, including those with disabilities resulting from <strong>HIV</strong>infection.<br />
The support services should address the residents’ individual needs, provide optimal independent<br />
living, and provide access to the community and employment opportunities.<br />
Section 811 funding is provided in two parts: a one-time capital advance, essentially a grant, to fund<br />
development, and ongoing project-based rental assistance that pays the difference between the tenant<br />
payment and the operating cost.<br />
<strong>Housing</strong> Choice Voucher (Section 8) Rental Assistance Programs<br />
http://www.hud.gov/<strong>of</strong>fices/pih/programs/hcv/about/index.cfm<br />
The <strong>Housing</strong> Choice Voucher Program (formerly called the Section 8 Program) provides vouchers which are<br />
administered by public housing authorities. Vouchers allow income-eligible households to find and obtain<br />
rental housing independently. Tenants typically pay 30 percent <strong>of</strong> their income, while the voucher pays the<br />
difference, up to the HUD-established Fair Market Rent (FMR) for the area. A tenant can pay more than 30<br />
percent <strong>of</strong> their income if the cost <strong>of</strong> the unit exceeds the FMR, but cannot pay more than 40 percent <strong>of</strong> their<br />
income.<br />
Public housing authorities can also designate up to 15 percent <strong>of</strong> their vouchers to be project-based in new<br />
construction or rehabilitated housing. Project-based vouchers stay with a particular unit, so that incomeeligible<br />
tenants can come and go, but the unit stays affordable. Tenants cannot take the vouchers away from<br />
the unit for use elsewhere.<br />
<strong>Housing</strong> Choice Vouchers for People with Disabilities (Mainstream Program)<br />
http://www.hud.gov/<strong>of</strong>fices/pih/programs/hcv/pwd/mainstream.cfm<br />
In Fiscal Year 1997, HUD moved a portion <strong>of</strong> the funds originally earmarked for the Supportive <strong>Housing</strong> for<br />
Persons with Disabilities (Section 811) program to create this separate tenant-based program. The <strong>Housing</strong><br />
Choice Vouchers for People with Disabilities (Mainstream Program) provides vouchers to persons with<br />
disabilities to allow for more housing choice.<br />
Low Income <strong>Housing</strong> Tax Credits<br />
http://www.huduser.org/datasets/lihtc.html<br />
Created in 1986, the Low Income <strong>Housing</strong> Tax Credit allows qualified owners <strong>of</strong> or investors in eligible lowincome<br />
rental housing to reduce their federal income taxes on a dollar-for-dollar basis for a ten-year period,<br />
subject to compliance. Low-income housing developers use these credits to attract investors, who commit to<br />
funding a project in return for the tax credit.<br />
Available tax credit dollars are allocated to states based on population, equal to $1.75 per capita in 2002 and<br />
adjusted for inflation thereafter. <strong>State</strong>s administer their own competitive process for the credits. The Low<br />
Income <strong>Housing</strong> Tax Credit program has become the primary federal resource for developing low-income
A-54 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
housing. Tax credits funded approximately 1.3 million units through 2003, and contribute to the development<br />
<strong>of</strong> approximately 73,000 additional units per year. 2<br />
Human Resources <strong>Services</strong> Administration, Ryan White <strong>HIV</strong>/<strong>AIDS</strong> Treatment<br />
Modernization Act<br />
http://hab.hrsa.gov/treatmentmodernization<br />
The Ryan White <strong>HIV</strong>/<strong>AIDS</strong> Treatment Modernization Act (formerly known as the Comprehensive <strong>AIDS</strong><br />
Resources Emergency (CARE) Act) is federal legislation that addresses the unmet health needs <strong>of</strong> persons<br />
living with <strong>HIV</strong> disease by funding primary health care and support services. In fiscal year 2006, Congress<br />
reauthorized the CARE Act under its new name and appropriated $2.06 billion 3 for use under the Act, which<br />
serves more than 500,000 people each year. 4 The Act, which is administered by the <strong>HIV</strong>/<strong>AIDS</strong> Bureau<br />
(HAB) <strong>of</strong> the Health Resources and <strong>Services</strong> Administration (HRSA), U.S. Department <strong>of</strong> Health and<br />
Human <strong>Services</strong>, is split into titles with different focuses and eligibility. Several titles allow funding <strong>of</strong> some<br />
housing services, as described in the HRSA publication “<strong>Housing</strong> is Health Care” (2000), 5 though policy<br />
changes have been considered but not finalized since the 2006 reauthorizations.<br />
Part A (formerly Title I) <strong>of</strong> the CARE Act funds emergency services for people living with <strong>HIV</strong>/<strong>AIDS</strong> in<br />
metropolitan areas with populations <strong>of</strong> at least 500,000 and more than 2,000 reported <strong>AIDS</strong> cases in the<br />
previous five years. Part B (formerly Title II) funds are awarded to all states by formula and provide primary<br />
healthcare and support services that enhance access to care for people living with <strong>HIV</strong>/<strong>AIDS</strong> and their<br />
families. Part B/Title II also supports <strong>AIDS</strong> Drug Assistance Programs (ADAPs) and, at the local consortia<br />
level, can fund community needs assessments and the organization and delivery <strong>of</strong> <strong>HIV</strong> services. Part C/Title<br />
III funds early intervention <strong>HIV</strong> services in outpatient settings and Part D/Title IV supports coordination <strong>of</strong><br />
services to youth, women, and families living with <strong>HIV</strong>/<strong>AIDS</strong> through public and private nonpr<strong>of</strong>it groups.<br />
Two additional new components have been added to the CARE Act; Part E covers General Provisions<br />
(including audits, privacy protections, and the severity <strong>of</strong> need index), while Part F consolidates these CARE<br />
Act programs:<br />
• Special Projects <strong>of</strong> National Significance (SPNS), which fund innovative models <strong>of</strong> care and support<br />
the development <strong>of</strong> effective delivery systems for <strong>HIV</strong> care. The SPNS Program is considered the<br />
research and development arm <strong>of</strong> the CARE Act.<br />
• <strong>HIV</strong>/<strong>AIDS</strong> Education and Training Centers<br />
• Dental Reimbursement Program<br />
• Community-Based Dental Partnership Program<br />
2 The Danter Company, Statistical Overview <strong>of</strong> the LIHTC Program, 1987 to 2003. Available online:<br />
www.danter.com/taxcredit/stats/htm (Accessed: October 7, 2005).<br />
3 U.S. Department <strong>of</strong> Health and Human <strong>Services</strong>, Health Resources and <strong>Services</strong> Administration, <strong>HIV</strong>/<strong>AIDS</strong> Bureau, CARE Act<br />
Administration Fact Sheet. Available online: http://hab.hrsa.gov/programs/Administration/index.htm (Accessed: March 2, 2007).<br />
4 U.S. Department <strong>of</strong> Health and Human <strong>Services</strong>, Health Resources and <strong>Services</strong> Administration, Ryan White Comprehensive <strong>AIDS</strong><br />
Resources Emergency (CARE) Act Appropriations History: FY 1991 to FY 2005. Available online:<br />
ftp://ftp.hrsa.gov/hab/fundinghis04.xls (Accessed: May 31, 2005).<br />
5 U.S. Department <strong>of</strong> Health and Human <strong>Services</strong>, Health Resources and <strong>Services</strong> Administration, <strong>HIV</strong>/<strong>AIDS</strong> Bureau, <strong>Housing</strong> is<br />
Health Care (2001). Available online: http://hab.hrsa.gov/tools/guidance/housing.htm (accessed January 31, 2008).
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-55<br />
U.S. Department <strong>of</strong> Agriculture Rural Development, Rural <strong>Housing</strong> Service<br />
http://www.rurdev.usda.gov/rhs/<br />
The Rural <strong>Housing</strong> Service (RHS) <strong>of</strong> the United <strong>State</strong>s Department <strong>of</strong> Agriculture (USDA) Rural<br />
Development provides a number <strong>of</strong> home ownership and rental opportunities for rural Americans. These<br />
programs provide a wide range <strong>of</strong> assistance, from direct loans to very low-, low-, or moderate-income<br />
households to buy or renovate existing housing to funding organizations to provide technical assistance to<br />
low- and very low-income households seeking to build their own homes in rural areas. Organizations eligible<br />
to apply for RHS funds include local and state government entities, associations, non-pr<strong>of</strong>it groups, and<br />
federally recognized Native American groups. Funds are also available to communities for construction <strong>of</strong><br />
essential facilities, such as hospitals, vocational rehabilitation centers, and public transportation, and to<br />
organizations needing to prepare sites with infrastructure, such as roads and sewage facilities.<br />
U.S. Department <strong>of</strong> Veterans Affairs,<br />
Homeless Providers Grant and Per Diem Program<br />
http://www1.va.gov/homeless/page.cfm?pg=3<br />
The Department <strong>of</strong> Veterans Affairs (VA) Health Care for Homeless Veterans (HCHV) Programs provide<br />
funding to community agencies providing services to homeless veterans. The purpose is to promote the<br />
development and provision <strong>of</strong> supportive housing and/or supportive services with the goal <strong>of</strong> helping<br />
homeless veterans achieve residential stability, increase their skill levels and/or income, and obtain greater<br />
self-determination.<br />
In February 2007, the VA announced the largest one-time designation in its history programs benefiting<br />
homeless veterans: $24 million, including $10 million for seriously mentally ill veterans, terminally ill<br />
veterans, and similarly vulnerable groups, such as veterans living with <strong>HIV</strong>/<strong>AIDS</strong>. Non-pr<strong>of</strong>it organizations,<br />
state and local government agencies that wish to start new programs to provide supportive housing or<br />
supportive services for homeless veterans can apply for funding. Only programs with supportive housing (up<br />
to 24 months) or service centers (<strong>of</strong>fering services such as case management, education, crisis intervention,<br />
counseling, etc.), where at least 75 percent <strong>of</strong> the clients served are veterans, are eligible for these funds.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-57<br />
Appendix 5: Glossary <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong>- and <strong>Housing</strong>-<br />
Related Terms<br />
This glossary includes terms used in the plan and terms related to <strong>HIV</strong>/<strong>AIDS</strong> and housing.<br />
AFFORDABLE HOUSING <strong>Housing</strong> is generally defined by the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban<br />
Development as affordable when the occupant is paying no more than 30 percent <strong>of</strong> their adjusted gross<br />
income for housing costs, including utilities. Affordable housing may refer to subsidized or unsubsidized<br />
units.<br />
<strong>AIDS</strong> Acquired Immunodeficiency Syndrome. A person with <strong>HIV</strong> infection is diagnosed with <strong>AIDS</strong> when<br />
either a) they develop an opportunistic infection defined by the Centers for Disease Control and Prevention<br />
as an <strong>AIDS</strong> indication, or b) on the basis <strong>of</strong> certain blood tests related to the immune system.<br />
ASSISTED LIVING Group residences that <strong>of</strong>fer the delivery <strong>of</strong> pr<strong>of</strong>essionally managed personal and health<br />
care services, including meals, 24-hour attendant care, social activities, assistance with bathing, dressing and<br />
transferring, dispensing medication, and health monitoring. Assisted living is intended for those who need<br />
some assistance in performing the activities <strong>of</strong> daily living but who do not need the high level <strong>of</strong> medical<br />
supervision provided by a skilled nursing facility. Assisted living facilities may be <strong>HIV</strong>/<strong>AIDS</strong>-specific, or<br />
they may serve people with many needs.<br />
ASYMPTOMATIC <strong>HIV</strong> INFECTION Without symptoms. Usually used in the <strong>HIV</strong>/<strong>AIDS</strong> literature to describe a<br />
person who has a positive reaction to one <strong>of</strong> several tests for <strong>HIV</strong> antibodies but who shows no clinical<br />
symptoms <strong>of</strong> the disease.<br />
AT RISK OF BECOMING HOMELESS Being on the brink <strong>of</strong> becoming homeless due to one or more <strong>of</strong> the<br />
following: having inadequate income or paying too high a percentage <strong>of</strong> income on rent (typically 50 percent<br />
or more), living in housing that does not meet federal housing quality standards, or living in housing that is<br />
seriously overcrowded. Also see Homeless Person.<br />
BEDS The unit <strong>of</strong> measure when describing the overnight sleeping capacity or availability for shelters,<br />
skilled nursing facilities, hospices, board and care, adult family living, assisted living, and other such<br />
facilities.<br />
CDC The Centers for Disease Control and Prevention, the lead federal agency for protecting health and<br />
safety. CDC serves as a national focus for developing and applying disease prevention and control,<br />
environmental health, and health promotion and education activities.<br />
CASE MANAGEMENT One key component <strong>of</strong> <strong>HIV</strong>/<strong>AIDS</strong> care is case management. Case managers<br />
coordinate all the care a client receives from all providers in the community. Typically, case management<br />
services are provided by agencies separate from the housing providers. When a case management client<br />
resides in a residence, however, the residential staff members have the most frequent contact with the<br />
resident and <strong>of</strong>ten are responsible for the care coordination. Case management is also provided through other<br />
social service systems.<br />
COMMUNITY DEVELOPMENT BLOCK GRANT PROGRAM (CDBG) A federal grant program (and part <strong>of</strong> the<br />
Consolidated Plan process), administered by the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development,<br />
authorized under Title I <strong>of</strong> the <strong>Housing</strong> and Community Development Act <strong>of</strong> 1974 and administered by state
A-58 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
and local governments. CDBG funds may be used in various ways to support community development,<br />
including acquisition, construction, rehabilitation, and/or operation <strong>of</strong> public facilities and housing.<br />
CONSOLIDATED PLAN A document written by a state or local government and submitted annually to the<br />
U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development that serves as the planning document <strong>of</strong> the<br />
jurisdiction and an application for funding under any <strong>of</strong> the community planning development formula grant<br />
programs:<br />
• Community Development Block Grant (CDBG)<br />
• Emergency Shelter Grant (ESG)<br />
• HOME Investment Partnerships Program (HOME)<br />
• <strong>Housing</strong> Opportunities for Persons with <strong>AIDS</strong> (HOPWA)<br />
The document describes the housing needs <strong>of</strong> the low- and moderate-income residents <strong>of</strong> a jurisdiction,<br />
outlining strategies to meet the needs and listing all resources available to implement the strategies.<br />
CONTINUUM OF CARE Generally, an approach that helps communities plan for and provide a full range <strong>of</strong><br />
emergency, transitional, and permanent housing and service resources to address the various needs <strong>of</strong><br />
homeless persons. The approach is based on the understanding that homelessness is not caused merely by a<br />
lack <strong>of</strong> shelter, but involves a variety <strong>of</strong> underlying, unmet needs—physical, economic, and social. Designed<br />
to encourage localities to develop a coordinated and comprehensive long-term approach to homelessness, the<br />
Continuum <strong>of</strong> Care consolidates the planning, application, and reporting documents for the U.S. Department<br />
<strong>of</strong> <strong>Housing</strong> and Urban Development’s following programs:<br />
• Shelter Plus Care (S+C)<br />
• Section 8 Moderate Rehabilitation Single-Room Occupancy Dwellings (SRO)<br />
• Supportive <strong>Housing</strong> Program (SHP)<br />
DEVELOPMENTAL DISABILITY Any <strong>of</strong> a variety <strong>of</strong> disabilities which impact cognitive functioning and<br />
learning style. Sometimes referred to as mental retardation.<br />
DISCRIMINATION Treating a person differently because they belong to, or are perceived to belong to, an<br />
identifiable group. Often discrimination is due to a person’s being from a different race, country, or religion,<br />
or because he or she is female, has a family, is older, is disabled, or is gay or lesbian.<br />
DUALLY DIAGNOSED See Multiply Diagnosed.<br />
EMA OR EMSA Eligible metropolitan (statistical) area. Geographic area based on population and cumulative<br />
<strong>AIDS</strong> cases, to receive federal funds through the Ryan White CARE Act and <strong>Housing</strong> Opportunities for<br />
Persons with <strong>AIDS</strong> (HOPWA) Program.<br />
EMERGENCY HOUSING ASSISTANCE Emergency housing assistance is one-time or very short-term<br />
assistance provided to address an immediate housing crisis—<strong>of</strong>ten for people who are homeless or at<br />
imminent risk <strong>of</strong> becoming homeless. The primary goal <strong>of</strong> emergency assistance is to solve the immediate<br />
housing crisis. The assistance is usually one <strong>of</strong> the following: emergency rent, mortgage or utility payments<br />
to prevent loss <strong>of</strong> residence, motel vouchers, and/or emergency shelter.<br />
EMERGENCY SHELTER Any facility with overnight sleeping accommodations, the primary purpose <strong>of</strong> which<br />
is to provide temporary shelter for homeless people in general or for specific populations <strong>of</strong> homeless people.<br />
EMERGENCY SHELTER GRANT PROGRAM (ESG) Part <strong>of</strong> the Consolidated Plan process, this federal program<br />
administered by the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development provides funds to local<br />
governments to help provide additional emergency shelters or improve the quality <strong>of</strong> existing emergency<br />
shelters and helps meet operating costs <strong>of</strong> essential social services to homeless individuals. Funds are
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-59<br />
provided to grantees through both a formula-based process for eligible metropolitan areas and urban counties<br />
and through a national competition for non-formula-eligible counties.<br />
EXTREMELY LOW-INCOME An individual or family whose income is between 0 and 30 percent <strong>of</strong> the median<br />
income for the area, as determined by the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development. (See Low-<br />
Income)<br />
FAIR HOUSING ACT The Federal Fair <strong>Housing</strong> Act prohibits, among other things, the owners <strong>of</strong> rental<br />
housing from discriminating against potential tenants based on race, sex, national origin, disability, or family<br />
size.<br />
FAIR MARKET RENT (FMR) Rents set by the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development (HUD) for<br />
a state, county, or urban area that define maximum allowable rents for HUD-funded subsidy programs. HUD<br />
calculates FMR to be at the 40 th percentile <strong>of</strong> recent moves, excluding apartments built within the past two<br />
years, meaning that 40 percent <strong>of</strong> recent movers paid less, and 60 percent paid more.<br />
FAMILY For purposes <strong>of</strong> the plan and local policy interpretation, and in keeping with HOPWA regulations,<br />
the term “family” encompasses nontraditional households, including families made up <strong>of</strong> unmarried domestic<br />
partners. A family is a self-defined group <strong>of</strong> people who may live together on a regular basis and who have a<br />
close, long-term, committed relationship and share responsibility for the common necessities <strong>of</strong> life. Family<br />
members may include adult partners, dependent elders, or children, as well as other people related by blood<br />
or marriage.<br />
FEDERAL EMERGENCY MANAGEMENT ADMINISTRATION (FEMA) An independent agency reporting to the<br />
President and tasked with responding to, planning for, recovering from, and mitigating disaster. FEMA<br />
administers the Emergency Food and Shelter Program as mandated by Title III <strong>of</strong> the McKinney-Vento Act.<br />
Also see McKinney-Vento Act.<br />
GROUP HOUSING/SHARED LIVING Two or more single adults, or families with children, sharing living<br />
arrangements in a house or an apartment. Generally, individuals each have a bedroom and share a kitchen,<br />
bath, and housekeeping responsibilities. The group facility may provide a limited range <strong>of</strong> services and be<br />
licensed or unlicensed.<br />
HAART Highly Active Anti-Retroviral Therapy. The preferred term for potent anti-<strong>HIV</strong> treatment. This<br />
means a combination <strong>of</strong> drugs (usually three or more) to combat <strong>HIV</strong>. Usually more than one class <strong>of</strong> drug is<br />
included in a HAART regimen. Includes protease inhibitors, and is <strong>of</strong>ten referred to as combination therapy<br />
or the “cocktail.” While it can be complicated to comply with, compliance to this regimen has dramatically<br />
extended the lives <strong>of</strong> people living with <strong>HIV</strong>/<strong>AIDS</strong>.<br />
HARM REDUCTION A set <strong>of</strong> practical strategies that reduce negative consequences <strong>of</strong> drug use, incorporating<br />
a spectrum <strong>of</strong> strategies for safer use, from managed use to abstinence. Harm reduction strategies meet drug<br />
users “where they’re at,” addressing conditions <strong>of</strong> use along with the use itself.<br />
<strong>HIV</strong> Human Immunodeficiency Virus. The virus that causes <strong>AIDS</strong>. <strong>HIV</strong> disease is characterized by a gradual<br />
deterioration <strong>of</strong> immune functions. During the course <strong>of</strong> infection, crucial immune cells, called CD4 T cells,<br />
are disabled and killed, and their numbers progressively decline. People infected with <strong>HIV</strong> may or may not<br />
feel or look sick.<br />
HOME HOME Investment Partnerships Program. Part <strong>of</strong> the Consolidated Plan process, this program is<br />
administered by the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development, and provides grants for lowincome<br />
housing through rental assistance, housing rehabilitation, and new construction.
A-60 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
HOMELESS PERSON According to the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development, a homeless<br />
person is an individual or family who 1) lacks a fixed, regular, and adequate night-time residence, or 2) has a<br />
primary night-time residence that is a) a publicly supervised or privately operated shelter designed to provide<br />
temporary living accommodations (including welfare hotels, congregate shelters, and transitional housing for<br />
the mentally ill); b) an institution that provides a temporary residence for individuals intended to be<br />
institutionalized; c) a public or private place not designed for, or ordinarily used as, a regular sleeping<br />
accommodation for human beings. Individuals paying more than 50 percent <strong>of</strong> their income for housing are<br />
also considered at such high risk for homelessness that they are included in the definition <strong>of</strong> homeless for<br />
some federal programs. The term “homeless individual” does not include any individuals imprisoned or<br />
otherwise detained under an act <strong>of</strong> federal or state law.<br />
HOPE VI HOPE VI, or the Urban Revitalization Program, a program administered by the U.S. Department <strong>of</strong><br />
<strong>Housing</strong> and Urban Development, funds rehabilitation and/or replacement <strong>of</strong> distressed public housing units<br />
and support services.<br />
HOPWA <strong>Housing</strong> Opportunities for Persons with <strong>AIDS</strong>. A U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban<br />
Development program which pays for housing and support services for people living with <strong>HIV</strong>/<strong>AIDS</strong> and<br />
their families. Part <strong>of</strong> the Consolidated Plan process, HOPWA was created by an Act <strong>of</strong> Congress in 1990.<br />
HOSPICE A support and care facility for people in the last phases <strong>of</strong> a terminal illness so that they may live<br />
as fully and comfortably as possible. Hospice focuses on alleviating pain and discomfort, improving the<br />
quality <strong>of</strong> life, and preparing individuals mentally and spiritually for their eventual death.<br />
HOUSING CHOICE VOUCHER PROGRAM (Formerly Section 8) A federal program operated by local housing<br />
authorities providing rental assistance to low-income persons and administered by the U.S. Department <strong>of</strong><br />
<strong>Housing</strong> and Urban Development. Under the <strong>Housing</strong> Choice Voucher (HCV) program, the local housing<br />
authority determines a standard amount <strong>of</strong> rental assistance an individual or family will receive. The tenant<br />
would pay the difference between the amount <strong>of</strong> assistance and the actual rent, which may require the tenant<br />
to spend more than 30 percent <strong>of</strong> their income on rent. The HCV program is a tenant-based program,<br />
meaning the subsidy is specific to the tenant as opposed to the unit. The following are HCV programs:<br />
• <strong>Housing</strong> Opportunities for Persons with Disabilities (Mainstream Program)<br />
The Mainstream Program, created in 1997 and administered by the U.S. Department <strong>of</strong> <strong>Housing</strong> and<br />
Urban Development, utilizes up to 25 percent <strong>of</strong> the funds originally earmarked for Section 811 to a<br />
separate tenant-based rental assistance program for persons with disabilities. Also see Section 811.<br />
• Moderate Rehabilitation for Single-Room Occupancy Dwellings<br />
This program provides Section 8 rental assistance for moderate rehabilitation <strong>of</strong> buildings with SRO<br />
units (single-room occupancy dwellings). The program, administered by the U.S. Department <strong>of</strong><br />
<strong>Housing</strong> and Urban Development, is designed for the use <strong>of</strong> an individual person. Units <strong>of</strong>ten do not<br />
contain food preparation or sanitary facilities. A public housing authority makes Section 8 rental<br />
assistance payments to the landlords for the homeless people who rent the rehabilitated units.<br />
HOUSING COST BURDEN The extent to which gross housing costs, including utility costs, exceed 30 percent<br />
<strong>of</strong> gross income, based on data published by the U.S. Census Bureau.<br />
SEVERE HOUSING COST BURDEN The level <strong>of</strong> burden at which gross housing costs, including utility costs,<br />
exceed 50 percent <strong>of</strong> gross income, based on data published by the U.S. Census Bureau.<br />
HOUSING UNIT An occupied or vacant house, apartment, or a single room (SRO housing) that is intended as<br />
separate living quarters.
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-61<br />
HOUSING QUALITY STANDARDS (HQS) Standards set by the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban<br />
Development (HUD) to ensure that all housing receiving HUD financial assistance meets a certain level <strong>of</strong><br />
quality. HQS requires that recipients <strong>of</strong> HUD funding provide safe and sanitary housing that is in compliance<br />
with state and local housing codes, licensing requirements, and any other jurisdiction-specific housing<br />
requirements.<br />
HRSA Health Resources and <strong>Services</strong> Administration. HRSA is an agency <strong>of</strong> the U.S. Department <strong>of</strong> Health<br />
and Human <strong>Services</strong> that works toward providing health care to low-income, uninsured, isolated, vulnerable,<br />
and special needs populations through a number <strong>of</strong> programs including the Ryan White CARE Act, Rural<br />
Health Initiative, and other community-based health initiatives. (See Ryan White CARE Act)<br />
HUD U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development. HUD is a cabinet-level agency designed to<br />
advocate for the housing needs <strong>of</strong> people with low incomes through programs for public housing, special<br />
needs housing, and first time homebuyers.<br />
INFORMATION AND REFERRAL Non-monetary assistance to individuals who are having a difficult time<br />
finding and/or securing housing.<br />
LOW-INCOME FAMILY Family whose income does not exceed 50 percent <strong>of</strong> the median family income (MFI)<br />
for the area, as determined by the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development (HUD), with<br />
adjustments for smaller and larger families. HUD may establish income ceilings higher or lower than 50<br />
percent <strong>of</strong> the median for the area on the basis <strong>of</strong> findings that such variations are necessary because <strong>of</strong><br />
prevailing levels <strong>of</strong> construction costs or Fair Market Rents, or unusually high or low family incomes.<br />
LOW INCOME HOUSING TAX CREDIT PROGRAM Formula allotment <strong>of</strong> federal income tax credits<br />
administered by states and distributed to nonpr<strong>of</strong>it and for-pr<strong>of</strong>it developers <strong>of</strong> and investors in low-income<br />
rental housing to encourage capacity development. Since its creation in 1986 by the Tax Reform Act, more<br />
than a million units have been funded nationwide, utilizing the equivalent <strong>of</strong> more than $7.5 billion dollars in<br />
funding annually.<br />
MAINSTREAM PROGRAM See <strong>Housing</strong> Choice Voucher (HCV) Program.<br />
MASTER LEASING A housing strategy in which a sponsor agency leases housing units from private or<br />
nonpr<strong>of</strong>it housing landlords and subleases the units to individuals and families that meet the sponsor<br />
agency’s eligibility criteria. This housing option is used mainly as transitional housing. In a transitional<br />
housing master leasing scenario, subleases with individuals and families can include stipulations for duration<br />
<strong>of</strong> tenancy and responsibilities <strong>of</strong> tenancy, such as a requirement to participate in support services. Master<br />
Leasing can be an alternative for landlords, since the sponsor agency absorbs some portion <strong>of</strong> the risk and<br />
responsibility for hard-to-house clients.<br />
MCKINNEY-VENTO ACT The primary federal response targeted to assisting homeless individuals and<br />
families. The scope <strong>of</strong> the Act includes: outreach, emergency food and shelter, transitional and permanent<br />
housing, primary health care services, mental health, alcohol and drug abuse treatment, education, job<br />
training, and child care. There are nine titles under the McKinney-Vento Act that are administered by several<br />
different federal agencies, including the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development (HUD).<br />
McKinney-Vento Act Programs administered by HUD include: Emergency Shelter Grant Program,<br />
Supportive <strong>Housing</strong> Program, Section 8 Moderate Rehabilitation for Single-Room Occupancy Dwellings,<br />
Supplemental Assistance to Facilities to Assist the Homeless, and Single Family Property Disposition<br />
Initiative. Also see: Emergency Shelter Grants, Federal Emergency Management Administration, Shelter<br />
Plus Care, Section 8 Moderate Rehabilitation for Single-Room Occupancy Dwellings, and Supportive<br />
<strong>Housing</strong> Program.
A-62 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
MEDIAN FAMILY INCOME (MFI) The amount, as determined by HUD, which divides an area’s income<br />
distribution into two equal groups, one having incomes above this amount, one having incomes below. MFI<br />
is based on the most recent U.S. Census family income data and is adjusted annually for inflation. HUD and<br />
the U.S. Census Bureau consider a family to be a household comprised <strong>of</strong> related individuals. For example:<br />
A family is a group <strong>of</strong> two people or more (one <strong>of</strong> whom is the householder) related by birth, marriage, or<br />
adoption and residing together; all such people (including related subfamily members) are considered as<br />
members <strong>of</strong> one family. This differs from Median Household Income, which is the median income <strong>of</strong> the<br />
householder and all people living in the house over the age <strong>of</strong> 15, regardless <strong>of</strong> relation to the householder.<br />
MEDICAID A program jointly funded by the states and the federal government (U.S. Department <strong>of</strong> Health<br />
and Human <strong>Services</strong>) that provides medical insurance for people who are unable to afford medical care. The<br />
program focuses mainly on the needs <strong>of</strong> the elderly, people with disabilities, and children.<br />
MEDICARE A federal program under the Social Security Administration that provides health insurance to the<br />
elderly and disabled.<br />
MENTAL ILLNESS A serious and persistent mental or emotional impairment that significantly limits a<br />
person’s ability to live independently.<br />
MODERATE INCOME An individual or family whose income is between 50 percent and 80 percent <strong>of</strong> the<br />
median income for the area, as determined by the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development<br />
(HUD), with adjustments for smaller or larger families. HUD may establish income ceilings higher or lower<br />
than 80 percent <strong>of</strong> the median for the area if they find that such variations are necessary because <strong>of</strong> prevailing<br />
levels <strong>of</strong> construction costs or Fair Market Rents, or unusually high or low family incomes.<br />
MULTIPLY DIAGNOSED To be diagnosed with <strong>HIV</strong>/<strong>AIDS</strong> and also have histories <strong>of</strong> other disabilities. This<br />
term generally refers to people who are <strong>HIV</strong>-positive and have chronic alcohol and/or other drug use<br />
problems and/or a serious mental illness. The terms “dually diagnosed” and “triply diagnosed” are also used.<br />
OPERATING COSTS (in relation to housing) Distinct from capital costs and support services costs. Operating<br />
costs include property taxes, insurance, maintenance, and repair.<br />
PERMANENT HOUSING <strong>Housing</strong> which is intended to be the tenant’s home for as long as they choose. In the<br />
supportive housing model <strong>of</strong> permanent housing, services are available to the tenant, but accepting services<br />
cannot be required <strong>of</strong> tenants or in any way impact their tenancy. Tenants <strong>of</strong> permanent housing sign legal<br />
lease documents.<br />
PERSON WITH A DISABILITY HUD’s <strong>Housing</strong> Choice Voucher (formerly Section 8) program defines a<br />
“person with a disability” on the terms <strong>of</strong> the Social Security Administration: a person who is determined to:<br />
1) have a physical, mental, or emotional impairment that is expected to be <strong>of</strong> continued and indefinite<br />
duration, substantially impedes his or her ability to live independently, and is <strong>of</strong> such a nature that the ability<br />
could be improved by more suitable housing conditions; or 2) have a developmental disability, as defined in<br />
the Developmental Disabilities Assistance and Bill <strong>of</strong> Rights Act.<br />
PROTEASE INHIBITORS A group <strong>of</strong> anti-retroviral medications for people living with <strong>HIV</strong>/<strong>AIDS</strong>. Protease<br />
inhibitors act by preventing the replication <strong>of</strong> <strong>HIV</strong> in the body and are <strong>of</strong>ten prescribed in combination with<br />
other <strong>HIV</strong> medications. Also see HAART.<br />
RENTAL ASSISTANCE Cash subsidy for housing costs provided as either project-based rental assistance or<br />
tenant-based rental assistance. HOPWA short-term rental assistance is available for up to 21 weeks. HOPWA<br />
long-term rental assistance is provided for longer than 21 weeks. Due to HOPWA regulations, rental<br />
assistance cannot be guaranteed for longer than three years. Ryan White funds can be used for short-term,
<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan—Appendices A-63<br />
transitional, or emergency housing defined as necessary to gain or maintain access to medical care. The<br />
following are the various types <strong>of</strong> rental assistance:<br />
• Project-based Rental Assistance<br />
Rental assistance that is tied to a specific unit <strong>of</strong> housing, not a specific tenant. Tenants receiving<br />
project-based rental assistance give up the right to that assistance upon moving from the unit. Also<br />
see Rental Assistance, Shallow Rent Subsidy, and Tenant-based Rental Assistance.<br />
• Tenant-based Rental Assistance<br />
A form <strong>of</strong> rental assistance in which the assisted tenant may move to a different housing unit while<br />
maintaining their assistance. The assistance is provided for the tenant, not a specific housing unit.<br />
Also see Project-based Rental Assistance, Rental Assistance, and Shallow Rent Subsidy.<br />
• Shallow Rent Subsidy<br />
Short-term or ongoing cash subsidy for housing costs provided as either project-based rental<br />
assistance or tenant-based rental assistance. Typically, shallow subsidies are for a set amount and are<br />
not related to the percentage <strong>of</strong> income paid to rent. Shallow rent subsidies are not an eligible<br />
HOPWA component unless approved within a competitive application. Also see Project-based<br />
Rental Assistance, Rental Assistance, and Tenant-based Rental Assistance.<br />
RYAN WHITE CARE ACT Ryan White Comprehensive <strong>AIDS</strong> Resources Emergency (CARE) Act. A program<br />
<strong>of</strong> the Health Resources and <strong>Services</strong> Administration (HRSA) providing funds for health care and supportive<br />
services for people living with <strong>AIDS</strong>, including emergency housing. Created by an Act <strong>of</strong> Congress in 1990.<br />
Also see HRSA.<br />
SCATTERED-SITE HOUSING Individual units scattered throughout an area, such as condominiums and single<br />
family homes in different complexes or neighborhoods, creating dispersed and integrated housing options.<br />
SECTION 8 See <strong>Housing</strong> Choice Voucher program.<br />
SECTION 811 Provides grants to nonpr<strong>of</strong>it organizations for acquisitions, new construction, and/or<br />
rehabilitation <strong>of</strong> rental housing with support services for very low-income persons with disabilities. The<br />
program is administered by the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development and includes a capital<br />
advance and project-based rental assistance payments. (See <strong>Housing</strong> Choice Voucher Mainstream Program)<br />
SHELTER PLUS CARE A national grant program administered by the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban<br />
Development providing rental assistance, linked with support services, to homeless individuals who have<br />
disabilities (primarily serious mental illness, chronic substance abuse, and disabilities resulting from<br />
<strong>HIV</strong>/<strong>AIDS</strong>) and their families.<br />
SKILLED NURSING FACILITY A nursing home or facility providing 24-hour care from nurses and aides.<br />
SRO Single-Room Occupancy. Refers to studio apartments which provide very limited cooking facilities and<br />
typically have shared bathrooms. They are <strong>of</strong>ten in rehabilitated hotels, and can be used for emergency,<br />
transitional, or permanent housing. (See <strong>Housing</strong> Choice Voucher Program)<br />
SOCIAL SECURITY DISABILITY INSURANCE (SSDI) A federal government benefit for individuals who are<br />
medically disabled and have worked for enough years to be covered under Social Security. (See Medicare,<br />
SSI)<br />
SPECIAL NEEDS HOUSING <strong>Housing</strong> for people who require specific accommodations and/or support to<br />
access and maintain housing. Special needs housing may target the elderly; people with disabilities,<br />
including <strong>HIV</strong>/<strong>AIDS</strong>; and people with histories <strong>of</strong> homelessness, mental illness, and/or substance use issues.
A-64 Appendices—<strong>Oregon</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Housing</strong> and <strong>Services</strong> <strong>Systems</strong> Integration Plan<br />
SUBSIDIZED RENTAL HOUSING Assisted housing that receives or has received project-based governmental<br />
assistance and is rented to low- or moderate-income households. Subsidized rental housing does not include<br />
owner-occupied units, nor does it include HCV holders in market-rate housing.<br />
SUBSTANCE USE ISSUES The problems resulting from a pattern <strong>of</strong> using substances such as alcohol and<br />
drugs. Problems can include: a failure to fulfill major responsibilities and/or using substances in spite <strong>of</strong><br />
physical, legal, social, and interpersonal problems and risks.<br />
SUPPLEMENTAL SECURITY INCOME (SSI) SSI is a federal government benefit for individuals who are 65 or<br />
older, or blind, or have a disability and earn a low income. (See Medicaid, SSDI)<br />
SUPPORTIVE HOUSING <strong>Housing</strong>, including housing units and group quarters, which include on- and <strong>of</strong>f-site<br />
support services. (See Permanent <strong>Housing</strong>, <strong>Housing</strong> First)<br />
SUPPORTIVE HOUSING PROGRAM (SHP) Provides grants to develop housing and related support services for<br />
people moving from homelessness to independent living. Program funds help homeless people live in a<br />
stable place, increase their skills or income, and gain more control over the decisions that affect their lives.<br />
Funding may be used for capital costs, facility operations, and/or support services. (See Continuum <strong>of</strong> Care)<br />
SUPPORT SERVICES <strong>Services</strong> provided to individuals to assist them to achieve and/or maintain stability,<br />
health, and improved quality <strong>of</strong> life. Some examples are case management, medical or psychological<br />
counseling and supervision, child care, transportation, and job training.<br />
SYMPTOMATIC <strong>HIV</strong> INFECTION Any perceptible, subjective change in the body or its functions that indicates<br />
disease or phases <strong>of</strong> disease, as reported by the patient. When referring to a person who is <strong>HIV</strong>-positive, this<br />
indicates a person who is sick and/or shows medical symptoms <strong>of</strong> the disease, but does not have an <strong>AIDS</strong><br />
diagnosis.<br />
TANF Temporary Assistance for Needy Families, a program administered by the U.S. Department <strong>of</strong> Health<br />
and Human <strong>Services</strong>. TANF, which replaced and is sometimes referred to as welfare, provides assistance and<br />
work opportunities to families with low incomes by granting states the federal funds and guidelines to<br />
administer their own welfare programs.<br />
TRANSGENDER Individuals whose sense <strong>of</strong> gender identity does not match their physiological sex, including<br />
those who have changed or are in the process <strong>of</strong> changing their sex from male to female or female to male.<br />
TRANSITIONAL HOUSING A project that is designed to provide housing and appropriate support services to<br />
homeless persons to facilitate movement to independent living within 24 months, or a longer period<br />
approved by the U.S. Department <strong>of</strong> <strong>Housing</strong> and Urban Development (HUD). (For purposes <strong>of</strong> the HOME<br />
program, there is not a HUD-approved time period for moving to independent living.)