Management of Labor
Management of Labor
Management of Labor

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
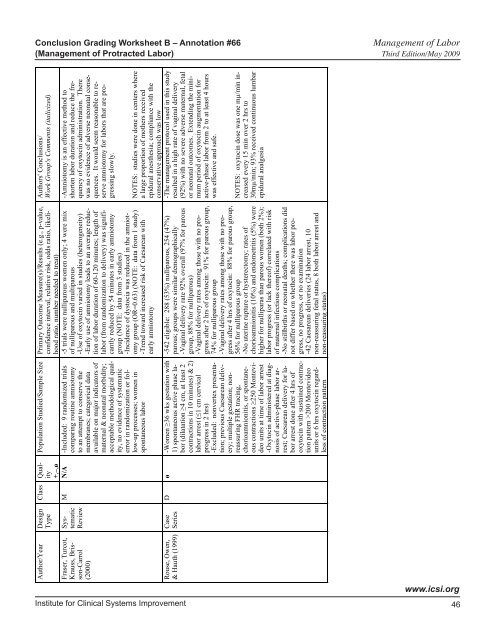
Conclusion Grading Worksheet B – Annotation #66 <strong>Management</strong> <strong>of</strong> <strong>Labor</strong><br />
(<strong>Management</strong> <strong>of</strong> Protracted <strong>Labor</strong>) Third Edition/May 2009<br />
Authors' Conclusions/<br />
Work Group's Comments (italicized)<br />
Population Studied/Sample Size Primary Outcome Measure(s)/Results (e.g., p-value,<br />
confidence interval, relative risk, odds ratio, likelihood<br />
ratio, number needed to treat)<br />
-5 trials were nulliparous women only; 4 were mix<br />
comparing routine amniotomy <strong>of</strong> nulliparous and multiparous<br />
to an attempt to conserve the -Use <strong>of</strong> oxytocin varied in studies (heterogeneity)<br />
membranes; categorical data -Early use <strong>of</strong> amniotomy leads to an average reduc-<br />
available on major indicators <strong>of</strong> tion <strong>of</strong> labor duration <strong>of</strong> 60-120 minutes; length <strong>of</strong><br />
maternal & neonatal morbidity; labor (from randomization to delivery) was signifi-<br />
acceptable methodological qualcantly reduced by 54 minutes in early amniotomy<br />
ity, no evidence <strong>of</strong> systematic group (NOTE: data from 3 studies)<br />
error in randomization or fol- -Incidence <strong>of</strong> dystocia was reduced in the amniotlow-up<br />
processes; women in omy group (OR=0.63) (NOTE: data from 1 study)<br />
spontaneous labor<br />
-Trend toward increased risk <strong>of</strong> Caesarean with<br />
early amniotomy<br />
Class Quality<br />
+,–,ø<br />
Author/Year Design<br />
Type<br />
-Amniotomy is an effective method to<br />
shorten labor duration and reduce the frequency<br />
<strong>of</strong> oxytocin administration. There<br />
was no evidence <strong>of</strong> adverse neonatal consequences.<br />
It would seem reasonable to reserve<br />
amniotomy for labors that are progressing<br />
slowly.<br />
M N/A -Included: 9 randomized trials<br />
Systematic<br />
Review<br />
Fraser, Turcot,<br />
Krauss, Brisson-Carrol<br />
(2000)<br />
NOTES: studies were done in centers where<br />
a large proportion <strong>of</strong> mothers received<br />
epidural anesthesia; compliance with the<br />
conservative approach was low<br />
-The management protocol used in this study<br />
resulted in a high rate <strong>of</strong> vaginal delivery<br />
(92%) with no severe adverse maternal, fetal<br />
or neonatal outcomes. Extending the minimum<br />
period <strong>of</strong> oxytocin augmentation for<br />
active-phase labor from 2 to at least 4 hours<br />
was effective and safe.<br />
Case<br />
Series<br />
Rouse, Owen,<br />
& Hauth (1999)<br />
Institute for Clinical Systems Improvement<br />
NOTES: oxytocin dose was one m#/min increased<br />
every 15 min over 2 hrs to<br />
30m#/min; 93% received continuous lumbar<br />
epidural analgesia<br />
-542 eligible: 288 (53%) nulliparous, 254 (47%)<br />
parous; groups were similar demographically<br />
-Vaginal delivery rate 92% overall (97% for parous<br />
group, 88% for nulliparous)<br />
-Vaginal delivery rates among those with no progress<br />
after 2 hrs <strong>of</strong> oxytocin: 91% for parous group,<br />
74% for nulliparous group<br />
-Vaginal delivery rates among those with no progress<br />
after 4 hrs <strong>of</strong> oxytocin: 88% for parous group,<br />
56% for nulliparous group<br />
-No uterine rupture or hysterectomy; rates <strong>of</strong><br />
chorioamnionitis (10%) and endometritis (5%) were<br />
higher for nulliparas than parous women (both 2%);<br />
labor progress (or lack there<strong>of</strong>) correlated with risk<br />
<strong>of</strong> maternal infectious complications<br />
-No stillbirths or neonatal deaths; complications did<br />
not differ based on whether there was labor progress,<br />
no progress, or no examination<br />
-42 Caesarean deliveries (24 labor arrest, 10<br />
non-reassuring fetal status, 8 both labor arrest and<br />
non-reassuring status)<br />
D ø -Women !36 wks gestation with<br />
1) spontaneous active phase labor<br />
(dilatation !4 cm, at least 2<br />
contractions in 10 minutes) & 2)<br />
labor arrest ("1 cm cervical<br />
progress in 2 hrs)<br />
-Excluded: nonvertex presentation;<br />
previous Caesarean delivery;<br />
multiple gestation; nonreassuring<br />
FHR tracing,<br />
chorioamnionitis, or spontaneous<br />
contractions !250 Montevideo<br />
units at time <strong>of</strong> labor arrest<br />
-Oxytocin administered at diagnosis<br />
<strong>of</strong> active-phase labor arrest;<br />
Caesarean delivery for labor<br />
arrest done after 4 hrs <strong>of</strong><br />
oxytocin with sustained contraction<br />
pattern >200 Montevideo<br />
units or 6 hrs oxytocin regardless<br />
<strong>of</strong> contraction pattern<br />
www.icsi.org<br />
46