Facility Name Address Phone_____ - Nevada State Health Division
Facility Name Address Phone_____ - Nevada State Health Division
Facility Name Address Phone_____ - Nevada State Health Division

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
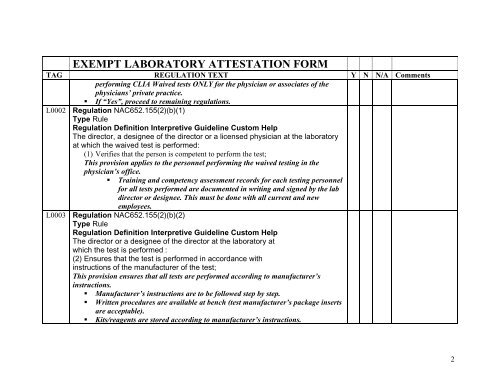
EXEMPT LABORATORY ATTESTATION FORM<br />
TAG REGULATION TEXT<br />
performing CLIA Waived tests ONLY for the physician or associates of the<br />
physicians’ private practice.<br />
Y N N/A Comments<br />
If “Yes”, proceed to remaining regulations.<br />
L0002 Regulation NAC652.155(2)(b)(1)<br />
Type Rule<br />
Regulation Definition Interpretive Guideline Custom Help<br />
The director, a designee of the director or a licensed physician at the laboratory<br />
at which the waived test is performed:<br />
(1) Verifies that the person is competent to perform the test;<br />
This provision applies to the personnel performing the waived testing in the<br />
physician’s office.<br />
Training and competency assessment records for each testing personnel<br />
for all tests performed are documented in writing and signed by the lab<br />
director or designee. This must be done with all current and new<br />
employees.<br />
L0003 Regulation NAC652.155(2)(b)(2)<br />
Type Rule<br />
Regulation Definition Interpretive Guideline Custom Help<br />
The director or a designee of the director at the laboratory at<br />
which the test is performed :<br />
(2) Ensures that the test is performed in accordance with<br />
instructions of the manufacturer of the test;<br />
This provision ensures that all tests are performed according to manufacturer’s<br />
instructions.<br />
Manufacturer’s instructions are to be followed step by step.<br />
Written procedures are available at bench (test manufacturer’s package inserts<br />
are acceptable).<br />
Kits/reagents are stored according to manufacturer’s instructions.<br />
2