

Percutane hartklep implantatie bij congenitale en ... - KCE
Percutane hartklep implantatie bij congenitale en ... - KCE
Percutane hartklep implantatie bij congenitale en ... - KCE

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
14 <strong>Percutane</strong>ous Heart Valves <strong>KCE</strong> Reports 95<br />
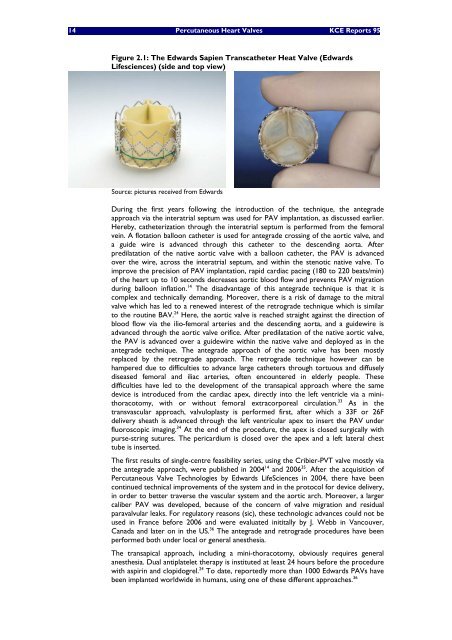
Figure 2.1: The Edwards Sapi<strong>en</strong> Transcatheter Heat Valve (Edwards<br />
Lifesci<strong>en</strong>ces) (side and top view)<br />
Source: pictures received from Edwards<br />
During the first years following the introduction of the technique, the antegrade<br />
approach via the interatrial septum was used for PAV implantation, as discussed earlier.<br />
Hereby, catheterization through the interatrial septum is performed from the femoral<br />
vein. A flotation balloon catheter is used for antegrade crossing of the aortic valve, and<br />
a guide wire is advanced through this catheter to the desc<strong>en</strong>ding aorta. After<br />
predilatation of the native aortic valve with a balloon catheter, the PAV is advanced<br />
over the wire, across the interatrial septum, and within the st<strong>en</strong>otic native valve. To<br />
improve the precision of PAV implantation, rapid cardiac pacing (180 to 220 beats/min)<br />
of the heart up to 10 seconds decreases aortic blood flow and prev<strong>en</strong>ts PAV migration<br />
during balloon inflation. 14 The disadvantage of this antegrade technique is that it is<br />
complex and technically demanding. Moreover, there is a risk of damage to the mitral<br />
valve which has led to a r<strong>en</strong>ewed interest of the retrograde technique which is similar<br />
to the routine BAV. 24 Here, the aortic valve is reached straight against the direction of<br />
blood flow via the ilio-femoral arteries and the desc<strong>en</strong>ding aorta, and a guidewire is<br />
advanced through the aortic valve orifice. After predilatation of the native aortic valve,<br />
the PAV is advanced over a guidewire within the native valve and deployed as in the<br />
antegrade technique. The antegrade approach of the aortic valve has be<strong>en</strong> mostly<br />
replaced by the retrograde approach. The retrograde technique however can be<br />
hampered due to difficulties to advance large catheters through tortuous and diffusely<br />
diseased femoral and iliac arteries, oft<strong>en</strong> <strong>en</strong>countered in elderly people. These<br />
difficulties have led to the developm<strong>en</strong>t of the transapical approach where the same<br />
device is introduced from the cardiac apex, directly into the left v<strong>en</strong>tricle via a minithoracotomy,<br />
with or without femoral extracorporeal circulation. 33 As in the<br />
transvascular approach, valvuloplasty is performed first, after which a 33F or 26F<br />
delivery sheath is advanced through the left v<strong>en</strong>tricular apex to insert the PAV under<br />
fluoroscopic imaging. 34 At the <strong>en</strong>d of the procedure, the apex is closed surgically with<br />
purse-string sutures. The pericardium is closed over the apex and a left lateral chest<br />
tube is inserted.<br />
The first results of single-c<strong>en</strong>tre feasibility series, using the Cribier-PVT valve mostly via<br />
the antegrade approach, were published in 2004 14 and 2006 35 . After the acquisition of<br />
<strong>Percutane</strong>ous Valve Technologies by Edwards LifeSci<strong>en</strong>ces in 2004, there have be<strong>en</strong><br />
continued technical improvem<strong>en</strong>ts of the system and in the protocol for device delivery,<br />
in order to better traverse the vascular system and the aortic arch. Moreover, a larger<br />
caliber PAV was developed, because of the concern of valve migration and residual<br />
paravalvular leaks. For regulatory reasons (sic), these technologic advances could not be<br />
used in France before 2006 and were evaluated inititally by J. Webb in Vancouver,<br />
Canada and later on in the US. 36 The antegrade and retrograde procedures have be<strong>en</strong><br />
performed both under local or g<strong>en</strong>eral anesthesia.<br />
The transapical approach, including a mini-thoracotomy, obviously requires g<strong>en</strong>eral<br />
anesthesia. Dual antiplatelet therapy is instituted at least 24 hours before the procedure<br />
with aspirin and clopidogrel. 24 To date, reportedly more than 1000 Edwards PAVs have<br />
be<strong>en</strong> implanted worldwide in humans, using one of these differ<strong>en</strong>t approaches. 36














