

Medication use in rest and nursing homes in Belgium. - KCE
Medication use in rest and nursing homes in Belgium. - KCE
Medication use in rest and nursing homes in Belgium. - KCE

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
50 <strong>Medication</strong> <strong>use</strong> <strong>in</strong> Nurs<strong>in</strong>g Homes <strong>KCE</strong> reports 47<br />
Institution Level<br />
gradations 1, 2 <strong>and</strong> 3 (positive or negative) respectively reflected a small, moderate or<br />
serious impact on the quality of provided care. The <strong>in</strong>dividual doma<strong>in</strong> scores were<br />
summed to a total score for both the wards <strong>and</strong> the nurs<strong>in</strong>g home management. The<br />
total score, which is a sum-score of all the different doma<strong>in</strong> scores, reflects the quality<br />
of the medication process <strong>in</strong> the nurs<strong>in</strong>g home.<br />
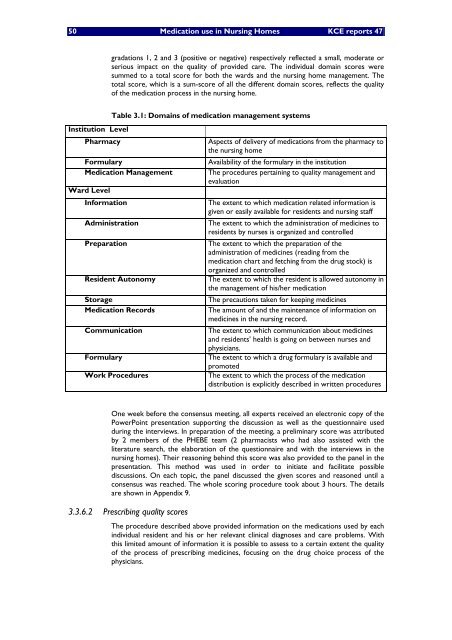
Table 3.1: Doma<strong>in</strong>s of medication management systems<br />
Pharmacy Aspects of delivery of medications from the pharmacy to<br />
the nurs<strong>in</strong>g home<br />
Formulary Availability of the formulary <strong>in</strong> the <strong>in</strong>stitution<br />
<strong>Medication</strong> Management The procedures perta<strong>in</strong><strong>in</strong>g to quality management <strong>and</strong><br />
evaluation<br />
Ward Level<br />
Information The extent to which medication related <strong>in</strong>formation is<br />
given or easily available for residents <strong>and</strong> nurs<strong>in</strong>g staff<br />
Adm<strong>in</strong>istration The extent to which the adm<strong>in</strong>istration of medic<strong>in</strong>es to<br />
residents by nurses is organized <strong>and</strong> controlled<br />
Preparation The extent to which the preparation of the<br />
adm<strong>in</strong>istration of medic<strong>in</strong>es (read<strong>in</strong>g from the<br />
medication chart <strong>and</strong> fetch<strong>in</strong>g from the drug stock) is<br />
organized <strong>and</strong> controlled<br />
Resident Autonomy The extent to which the resident is allowed autonomy <strong>in</strong><br />
the management of his/her medication<br />
Storage The precautions taken for keep<strong>in</strong>g medic<strong>in</strong>es<br />
<strong>Medication</strong> Records The amount of <strong>and</strong> the ma<strong>in</strong>tenance of <strong>in</strong>formation on<br />
medic<strong>in</strong>es <strong>in</strong> the nurs<strong>in</strong>g record.<br />
Communication The extent to which communication about medic<strong>in</strong>es<br />
<strong>and</strong> residents health is go<strong>in</strong>g on between nurses <strong>and</strong><br />
physicians.<br />
Formulary The extent to which a drug formulary is available <strong>and</strong><br />
promoted<br />
Work Procedures The extent to which the process of the medication<br />
distribution is explicitly described <strong>in</strong> written procedures<br />
One week before the consensus meet<strong>in</strong>g, all experts received an electronic copy of the<br />
PowerPo<strong>in</strong>t presentation support<strong>in</strong>g the discussion as well as the questionnaire <strong>use</strong>d<br />
dur<strong>in</strong>g the <strong>in</strong>terviews. In preparation of the meet<strong>in</strong>g, a prelim<strong>in</strong>ary score was attributed<br />
by 2 members of the PHEBE team (2 pharmacists who had also assisted with the<br />
literature search, the elaboration of the questionnaire <strong>and</strong> with the <strong>in</strong>terviews <strong>in</strong> the<br />
nurs<strong>in</strong>g <strong>homes</strong>). Their reason<strong>in</strong>g beh<strong>in</strong>d this score was also provided to the panel <strong>in</strong> the<br />
presentation. This method was <strong>use</strong>d <strong>in</strong> order to <strong>in</strong>itiate <strong>and</strong> facilitate possible<br />
discussions. On each topic, the panel discussed the given scores <strong>and</strong> reasoned until a<br />
consensus was reached. The whole scor<strong>in</strong>g procedure took about 3 hours. The details<br />
are shown <strong>in</strong> Appendix 9.<br />
3.3.6.2 Prescrib<strong>in</strong>g quality scores<br />
The procedure described above provided <strong>in</strong>formation on the medications <strong>use</strong>d by each<br />
<strong>in</strong>dividual resident <strong>and</strong> his or her relevant cl<strong>in</strong>ical diagnoses <strong>and</strong> care problems. With<br />
this limited amount of <strong>in</strong>formation it is possible to assess to a certa<strong>in</strong> extent the quality<br />
of the process of prescrib<strong>in</strong>g medic<strong>in</strong>es, focus<strong>in</strong>g on the drug choice process of the<br />
physicians.














