Preparing the Wound Bed – Debridement, Bacterial Balance, and ...
Preparing the Wound Bed – Debridement, Bacterial Balance, and ...
Preparing the Wound Bed – Debridement, Bacterial Balance, and ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Preparing</strong> <strong>the</strong> <strong>Wound</strong> <strong>Bed</strong> <strong>–</strong><br />
<strong>Debridement</strong>, <strong>Bacterial</strong><br />
<strong>Balance</strong>, <strong>and</strong> Moisture <strong>Balance</strong><br />
<strong>–</strong> R. Gary Sibbald, MD, FRCPC; Diane Williamson, MB, MRCP(UK); Hea<strong>the</strong>r L. Orsted, RN, BN, ET; Karen<br />
Campbell, RN, MScN; David Keast, MD, CCFP; Diane Krasner, PhD, RN, CWOCN, CWS, FAAN; <strong>and</strong> Debra<br />
Sibbald, BScPhm<br />
ABSTRACT<br />
Successful diagnosis <strong>and</strong> treatment of patients with chronic wounds<br />
involve holistic care <strong>and</strong> a team approach. The integration of <strong>the</strong><br />
work of an interdisciplinary care team that includes doctors, nurses,<br />
<strong>and</strong> allied health professionals with <strong>the</strong> patient, family, significant<br />
o<strong>the</strong>rs, <strong>and</strong> caregivers offers an optimal formula for achieving<br />
wound resolution. Such an approach challenges practitioners <strong>and</strong><br />
everyone participating in wound care to integrate data <strong>and</strong> information<br />
that arise from a number of sources <strong>and</strong> mitigating factors.<br />
In this article, <strong>the</strong> authors define <strong>the</strong> changing paradigm that links<br />
treatment of <strong>the</strong> cause <strong>and</strong> focuses on three components of local<br />
wound care: debridement, wound-friendly moist interactive dressings,<br />
<strong>and</strong> bacterial balance. The authors demonstrate that <strong>the</strong><br />
treatment of chronic wounds can be accomplished through a series<br />
of recommendations <strong>and</strong> rationales based on <strong>the</strong> literature <strong>and</strong><br />
<strong>the</strong>ir experience. These recommendations lay <strong>the</strong> groundwork for<br />
thorough assessment <strong>and</strong> evaluation of <strong>the</strong> wound.<br />
Ostomy/<strong>Wound</strong> Management 2000;46(11):14<strong>–</strong>35<br />
Achronic wound is one in which <strong>the</strong> orderly<br />
sequence of repair is disrupted at one or several<br />
points of <strong>the</strong> inflammatory, proliferative, re-epi<strong>the</strong>lization,<br />
<strong>and</strong> remodeling stages. 1 Key articles of Winter in<br />
<strong>the</strong> 1960s 2<strong>–</strong>3 demonstrated <strong>the</strong> benefits of moist interactive<br />
healing. Unfortunately, clinical practices have not always<br />
14 Ostomy<strong>Wound</strong> Management<br />
kept pace with <strong>the</strong> evidence base. The chronic wound must<br />
be directed back to this orderly nexus of events. Despite<br />
treating <strong>the</strong> cause, providing appropriate local wound care,<br />
<strong>and</strong> attending to patient-centered concerns, a certain percentage<br />
of wounds do not heal with best practices. Three<br />
components involved in healing <strong>the</strong> wound that must be<br />
considered by <strong>the</strong> healthcare professional include: treating<br />
<strong>the</strong> cause, providing local wound care, <strong>and</strong> addressing<br />
patient-centered concerns (see Figure 1). This paper focuses<br />
on local wound care involving preparation of <strong>the</strong> wound.<br />
The recommendations to follow can be used as a guide for<br />
multidisciplinary teams to consider in order to obtain optimal<br />
healing (see Table 1).<br />
Recommendation 1<br />
Assess <strong>the</strong> Patient for Adequate Blood Supply <strong>and</strong><br />
Host Factors for Healability<br />
The local wound must be considered with underlying<br />
causes, <strong>the</strong> patient’s physical condition, <strong>and</strong> related extenuating<br />
<strong>and</strong> mitigating circumstances. One important consideration<br />
is to ensure that <strong>the</strong> wound has enough blood supply to<br />
heal prior to initiating wound management. 4 This is an<br />
especially important principle for wounds of <strong>the</strong> lower<br />
extremity. If a palpable dorsalis pedis or posterior tibial pulse<br />
is present, <strong>the</strong> systolic pressure is approximately 80 mm Hg<br />
or greater. The Doppler ankle brachial pressure index<br />
(ABPI) is often used to diagnose arterial disease. 5 A systolic<br />
Dr. Sibbald is Associate Professor of Medicine at <strong>the</strong> University of Toronto. Ms. Williamson is a Fellow in <strong>Wound</strong> Care at <strong>the</strong> Women’s College<br />
Campus, Sunnybrook <strong>and</strong> Women’s College Health Sciences Centre, Toronto. Ms. Orsted is a Clinical Specialist, Skin <strong>and</strong> <strong>Wound</strong> Management,<br />
with Calgary <strong>Wound</strong> Care, Calgary, Alberta. Ms. Campbell is a Clinical Nurse Specialist at Parkwood Hospital, University of Western Ontario,<br />
London, Ontario. Dr. Keast is a physician specializing in family medicine at Parkwood Hospital. Dr. Krasner is a <strong>Wound</strong> Care Consultant <strong>and</strong><br />
Adjunct Associate Professor, Johns Hopkins University School of Nursing, Baltimore, Md. Ms. Sibbald is Senior Lecturer, Faculty of Pharmacy,<br />
University of Toronto. Address correspondence to: R. Gary Sibbald, MD, FRCPC, Women’s College Campus, SWCHSC, 76 Grenville Street,<br />
Toronto, Ontario, Canada.
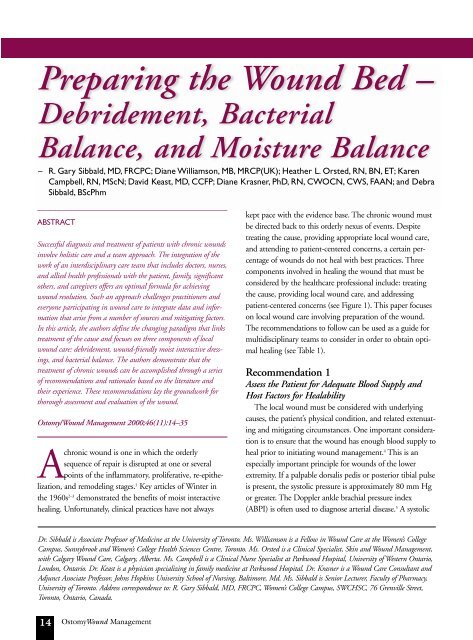
This necrotic heel ulcer was caused by perioperative pressure.<br />
Black eschar can be seen over <strong>the</strong> ulcer. A pulse is present<br />
(> 80 mm Hg), indicating enough blood supply to heal.<br />
For sharp surgical debridement, a scalpel <strong>and</strong> scissors have<br />
been used to lift <strong>the</strong> eschar, revealing <strong>the</strong> underlying healthy,<br />
viable tissue.<br />
In this unhealthy wound bed, fronds of bright red, friable<br />
granulation tissue, increased wound exudate, <strong>and</strong> a white<br />
macerated wound margin were all signs of an increased bacterial<br />
burden.<br />
Autolytic debridement of a necrotic heel ulcer. Cross-hatching<br />
<strong>the</strong> wound can be used to facilitate autolytic debridement<br />
with moist interactive dressings.<br />
This leg ulcer has a base of loose slough <strong>and</strong> debris. The devitalized<br />
tissue is an excellent bacterial culture media with <strong>the</strong><br />
green discoloration indicating <strong>the</strong> presence of pseudomonas.<br />
In this wound, a healthy pink granulation base is surrounded<br />
by a thin rim of a new purple epi<strong>the</strong>lium.<br />
November 2000 Vol. 46 Issue 11 15
pressure ratio of 0.8 (eg, ankle systolic 80 mm Hg, brachial<br />
systolic 100 mm Hg) <strong>and</strong> higher indicates <strong>the</strong> absence of<br />
significant arterial disease, but a ratio below 0.5 suggests<br />
severe arterial compromise <strong>and</strong> a low probability of healing.<br />
The introduction of <strong>the</strong> h<strong>and</strong>held Doppler into clinics <strong>and</strong><br />
homecare settings 6 has allowed practitioners to help identify<br />
patients with arterial disease.<br />
Patients with diabetes often have calcification of larger<br />
vessels, which leads to <strong>the</strong>ir noncompressibility. This will<br />
result in a falsely high ABPI value <strong>and</strong> healability should be<br />
assessed with transcutaneous partial oxygen saturation of<br />
>30% or toe arterial pressures (taken by photophlethysmography)<br />
of >40 mm Hg. Patients with symptoms of intermittent<br />
claudication at rest also should be assessed for surgery.<br />
Not all patients are c<strong>and</strong>idates for vascular procedures,<br />
<strong>and</strong> if extensive <strong>and</strong> diffuse distal dis-<br />
ease is present, <strong>the</strong>se procedures will not be beneficial.<br />
If nonhealability is established, <strong>the</strong>n<br />
moist interactive local wound care is contraindicated.<br />
Topical antiseptics to dry <strong>the</strong> wound <strong>and</strong><br />
prevent proximal bacterial invasion of viable tissue<br />
are recommended (see Recommendation 6).<br />
Recommendation 2<br />
Assess <strong>and</strong> Monitor <strong>the</strong> <strong>Wound</strong> History<br />
<strong>and</strong> Physical Characteristics (location,<br />
size, base, exudate, <strong>the</strong> condition of surrounding<br />
skin, staging, <strong>and</strong> pain)<br />
16 Ostomy<strong>Wound</strong> Management<br />
Chronic <strong>Wound</strong><br />
Diagnosis<br />
Treat Cause Local <strong>Wound</strong> Care Patient-Centered<br />
Concerns<br />
<strong>Debridement</strong><br />
<strong>Bacterial</strong> <strong>Balance</strong><br />
Non-healing <strong>Wound</strong><br />
Biological Agents<br />
•Growth Factors<br />
•Cells <strong>–</strong> skin substitutes<br />
•Acellular matrix<br />
Figure 1<br />
This algorithm demonstrates an approach to <strong>the</strong> treatment of chronic wounds.<br />
Moist Interactive<br />
Healing<br />
Chronic wound care must<br />
include ongoing, consistent documentation<br />
of wound characteristics<br />
as part of continuous<br />
monitoring for complications<br />
<strong>and</strong> appropriate management.<br />
<strong>Wound</strong> history. Patients<br />
should be asked about <strong>the</strong> duration<br />
of <strong>the</strong> current ulcer <strong>and</strong> if<br />
he or she has had an ulcer previously<br />
<strong>and</strong> what, if any, treatment<br />
has been provided. The<br />
more chronic an ulcer becomes,<br />
<strong>the</strong> more difficult it is to heal. If<br />
it is recurrent, issues of prevention<br />
may not have been adequately<br />
addressed.<br />
<strong>Wound</strong> location <strong>and</strong> size.<br />
The precise location of <strong>the</strong><br />
wound should be noted <strong>and</strong> can<br />
often be outlined on a body map or diagram. Measuring <strong>the</strong><br />
length (usually <strong>the</strong> longest diameter) <strong>and</strong> <strong>the</strong> maximum<br />
width at right angles to <strong>the</strong> diameter is important. This is<br />
usually documented in centimeters. 7 <strong>Wound</strong> circumference<br />
can be traced onto a transparency or plastic page protector.<br />
Use disposable plastic wrap next to <strong>the</strong> skin to avoid bacterial<br />
contamination. A maximum depth should be measured<br />
with a probe (sterile metal surgical instrument, sterile plastic<br />
depth guide, or even a sterile cotton-tipped applicator or<br />
sterile swab). Place <strong>the</strong> depth gauge in <strong>the</strong> deepest part of<br />
<strong>the</strong> wound <strong>and</strong> use a gloved finger or a pen mark at <strong>the</strong> surface<br />
to determine <strong>the</strong> depth that can be measured with a<br />
ruler. The wound base also should be probed with caution<br />
Ostomy/<strong>Wound</strong> Management 2000;46(11):14<strong>–</strong>35<br />
L<br />
KEY POINTS<br />
❏ The provision of optimal local wound care involves a myriad of<br />
patient <strong>and</strong> wound assessment variables, environmental considerations,<br />
<strong>and</strong> treatment option decisions.<br />
❏ Using a holistic approach, <strong>the</strong> authors developed 13 general wound<br />
care recommendations while providing sufficient background information<br />
to tailor each of <strong>the</strong>ir recommendations to <strong>the</strong> needs of <strong>the</strong><br />
individual patient.<br />
❏ As <strong>the</strong> number of wound treatment choices continues to increase,<br />
it is important to remember, <strong>and</strong> start with, <strong>the</strong> basic principles of<br />
good wound care (debridement, bacterial balance, <strong>and</strong> moist<br />
interacive healing).<br />
3
TABLE 1<br />
QUICK REFERENCE GUIDE TO THE 13<br />
RECOMMENDATIONS FOR PRACTICE:<br />
PREPARING THE WOUND BED<br />
1. Assess <strong>the</strong> patient for adequate blood supply <strong>and</strong> host factors<br />
for healability.<br />
2. Assess <strong>and</strong> monitor <strong>the</strong> wound history <strong>and</strong> physical characteristics<br />
(location, size, base, exudate, <strong>the</strong> surrounding skin,<br />
staging, <strong>and</strong> pain).<br />
3. Correct treatable causes of tissue damage.<br />
4. Provide education <strong>and</strong> support for patient-centered care to<br />
increase compliance.<br />
5. Debride healable wounds, removing necrotic <strong>and</strong> nonviable<br />
tissue.<br />
6. Assess <strong>the</strong> wound for bacterial balance <strong>and</strong> infection.<br />
7. Cleanse wounds with normal saline or water.The use of<br />
topical antiseptics should be reserved for wounds that are<br />
nonhealable or those in which <strong>the</strong> local bacterial burden is a<br />
greater concern than <strong>the</strong> stimulation of healing.<br />
8. If MRSA is present, assess <strong>the</strong> patient for colonization or<br />
infection. Select appropriate topical <strong>and</strong>/or systemic agent<br />
for treatment.<br />
9. Use only nonsensitizing topical antibacterial agents for local<br />
symptoms <strong>and</strong> signs of infection or increased bacterial burden.<br />
10. Use systemic antibiotics if symptoms or signs of infection<br />
extend beyond wound margin or <strong>the</strong> ulcer probes to bone.<br />
11. Select appropriate dressings for local moisture balance to<br />
stimulate granulation tissue <strong>and</strong> re-epi<strong>the</strong>lialization.<br />
12. Evaluate expected rate of wound healing to determine if<br />
treatment is optimal.<br />
13. Use biological agents when o<strong>the</strong>r factors have been corrected<br />
<strong>and</strong> healing does not progress at <strong>the</strong> expected rate.<br />
for bone, sinuses, or undermining. One of <strong>the</strong> best ways to<br />
document wound characteristics is to use a flow chart. In<br />
<strong>the</strong> future, digital photography with color printouts may<br />
become <strong>the</strong> norm in everyday practice.<br />
<strong>Wound</strong> base. It is helpful to think of <strong>the</strong> wound in four<br />
major colors: black (necrotic), yellow (fibrous), red-pink<br />
(granulation tissue), pink-purple (re-epi<strong>the</strong>lialization), or a<br />
combination of <strong>the</strong>se colors. Black eschar represents devitalized<br />
tissue that may be soft or firm. If healability has been<br />
established, <strong>the</strong>n eschar needs to be removed to promote<br />
healing. A yellow fibrous base may be firm or sloughy. A<br />
firm, yellow base represents underlying deep structures such<br />
as fascia or subcutaneous fat or <strong>the</strong> fibrin base for subsequent<br />
granulation tissue <strong>and</strong> does not need to be removed.<br />
Soft sloughy yellow material may indicate infection or<br />
degraded fibrin that needs to be removed.<br />
Granulation tissue is usually a salmon red-pink<br />
color, firm <strong>and</strong> moist. With increased bacterial<br />
load, this granulation tissue may become darker,<br />
exuberant, friable, <strong>and</strong> malodorous. Hypergranulation<br />
should be documented because it<br />
may require removal to facilitate re-epi<strong>the</strong>lialization.<br />
Newly formed epi<strong>the</strong>lialization is a<br />
pink-purple color that usually appears at <strong>the</strong><br />
flush edges of <strong>the</strong> wound, but may occur in<br />
<strong>the</strong> center around <strong>the</strong> underlying hair follicle<br />
structures.<br />
Exudate. Exudate is usually described by its<br />
quantity (scant, moderate, <strong>and</strong> copious); characteristics<br />
(serous-serum, sanguinous-blood,<br />
purulent-infection, or a combination of <strong>the</strong>se);<br />
<strong>and</strong> odor (presence or absence). In general,<br />
heavy exudates, even when clear fluid, should<br />
alert clinicians to problems related to <strong>the</strong><br />
underlying cause (uncontrolled edema) or an<br />
early sign that <strong>the</strong>re may be increased bacterial<br />
burden or infection.<br />
<strong>Wound</strong> margin <strong>and</strong> surrounding skin.<br />
The wound margin should be checked for callus<br />
formation, excess moisture in <strong>the</strong> form of<br />
maceration, edema, or ery<strong>the</strong>ma.<br />
Hyperkeratotic (thick) callus, especially in persons<br />
with diabetes on <strong>the</strong> plantar aspect of <strong>the</strong><br />
foot, can lead to increased local pressure. 8<br />
Removing this type of callus is important. If<br />
<strong>the</strong> callus continues to form, pressure offloading<br />
is not optimal <strong>and</strong> <strong>the</strong> patient will require<br />
reassessment. Maceration of <strong>the</strong> surrounding skin usually<br />
presents with white hyperkeratosis <strong>and</strong> a wet surface. This<br />
indicates increased hydration of <strong>the</strong> keratin, <strong>and</strong> may be a<br />
reflection of a local dressing that is keeping <strong>the</strong> ulcer too<br />
moist or not absorbing exudate, an uncorrected cause (eg,<br />
limb edema or uncorrected pressure), or a sign of infection.<br />
The presence of ery<strong>the</strong>ma locally is a sign of inflammation<br />
or infection. If this ery<strong>the</strong>ma is warm, hot, <strong>and</strong> tender,<br />
infection is most likely. Discreet ery<strong>the</strong>ma with well demarcated<br />
margins that follow <strong>the</strong> outlines of applied dressings or<br />
topical treatments may indicate a contact allergic dermatitis.<br />
Common allergens, such as neomycin, lanolin, <strong>and</strong> perfumes<br />
must be avoided at all times. Chronic wounds allow<br />
optimal penetration of <strong>the</strong>se substances <strong>and</strong> systemic processing<br />
by <strong>the</strong> immune system.<br />
November 2000 Vol. 46 Issue 11 17
Nociceptive Pain<br />
(normal nerve<br />
function)<br />
Contact irritant dermatitis also can occur <strong>and</strong> is less specific.<br />
There is an absence of <strong>the</strong> clear outline at <strong>the</strong> edges of<br />
<strong>the</strong> irritation, although ery<strong>the</strong>ma, scaling, <strong>and</strong> some maceration<br />
may also occur. Chronic irritant dermatitis is best treated<br />
with protectants such as petrolatum, zinc oxide ointment,<br />
or commercial barrier preparations around <strong>the</strong> wound<br />
margins. Thick materials often can be applied with a tongue<br />
depressor to decrease frictional resistance.<br />
Staging of <strong>the</strong> wound. General <strong>and</strong> disease-specific tools<br />
can be used to grade or stage chronic wounds. However, all<br />
wounds can be classified as partial or full thickness. 9 The<br />
National Pressure Ulcer Advisory Panel/Agency for Health<br />
Care Policy <strong>and</strong> Research (NPUAP/AHCPR) has a fourstage<br />
system for pressure ulcers, 9 <strong>and</strong> alternative systems<br />
should be used for leg <strong>and</strong> o<strong>the</strong>r ulcers. In general, this system<br />
applies to Stage I for persistent ery<strong>the</strong>ma but intact<br />
skin. Stage II represents an erosion (epidermal base) or<br />
superficial ulceration (dermal base). Stage III wounds have a<br />
subcutaneous fat base, <strong>and</strong> Stage IV wounds have a deeper<br />
muscle, tendon, bone, or joint base. Staging an ulcer <strong>and</strong><br />
documenting <strong>the</strong> initial assessment of wounding is important.<br />
O<strong>the</strong>r descriptors have been recommended for <strong>the</strong><br />
healing process 10 (see Recommendation 8 of Best Practices for<br />
<strong>the</strong> Prevention <strong>and</strong> Treatment of Pressure Ulcers by Dolynchuk<br />
et al on page 45). For diabetic foot ulcers, <strong>the</strong> University of<br />
Texas treatment based classification system addresses neuropathy,<br />
deformity, vascularity <strong>and</strong> infection. 11,12 (See<br />
Recommendation 4 of Best Practices for <strong>the</strong> Prevention,<br />
Diagnosis, <strong>and</strong> Treatment of Diabetic Foot Ulcers by Inlow et<br />
al on page 59.)<br />
18 Ostomy<strong>Wound</strong> Management<br />
TABLE 2<br />
AN APPROACH TO PAIN MANAGEMENT<br />
Type of Pain/Symptoms Treatment<br />
Aching, throbbing,<br />
sharp, easily localized<br />
Neuropathic pain<br />
Shooting, stabbing<br />
Mild<br />
Moderate<br />
Severe<br />
Nerve irritation<br />
(burning)<br />
Nerve damage<br />
(shooting, stabbing)<br />
Acetominophen, aspirin or nonsteroidal anti-inflammatory,<br />
plus a co-analgesic<br />
Codeine, oxycodone, or o<strong>the</strong>r mild opiod plus<br />
acetominophen or aspirin plus co-analgesic<br />
Morphine, hydromorphone, fentanyl, diacetyl morphine<br />
plus co-analgesic<br />
Tricyclic antidepressants, gabapentin<br />
Gabapentin<br />
Pain. Pain also may be an important indicator of untreated<br />
disease. Krasner’s 13 model of chronic wound pain divides<br />
stimuli into incident pain, recurrent episodic pain, <strong>and</strong> continuous<br />
pain. Incident pain occurs with debridement or<br />
major trauma. This type of pain can be relieved with topical<br />
analgesia, interlesional analgesia, or presedation with agents<br />
following <strong>the</strong> World Health Organization pain ladder. 14<br />
Episodic pain often can occur with dressing changes. Pain<br />
control, both local <strong>and</strong> systemic, should be instituted at<br />
appropriate time periods before dressing changes for comfort<br />
(see Table 2). Continuous pain may reflect <strong>the</strong> lack of<br />
treatment of <strong>the</strong> underlying cause, local wound irritation, or<br />
infection. Careful assessment of continuous pain must be<br />
made to determine if its origin is in <strong>the</strong> local wound or <strong>the</strong><br />
surrounding anatomical region.<br />
<strong>Wound</strong> pain should be routinely assessed <strong>and</strong> documented<br />
using <strong>the</strong> patient’s self report. The 10-cm visual analog<br />
scale is <strong>the</strong> gold st<strong>and</strong>ard for quantitative pain assessment.<br />
Using this scale, patients grade <strong>the</strong>ir pain by placing a mark<br />
on <strong>the</strong> 10-cm line where 0 indicates no pain <strong>and</strong> 10 indicates<br />
<strong>the</strong> worst pain ever experienced. The presence of new<br />
or increasing pain in <strong>the</strong> chronic wound patient often signals<br />
complications such as infection, a Charcot arthopathy,<br />
or vascular compromise.<br />
Recommendation 3<br />
Correct Treatable Causes of Tissue Damage<br />
It is important to always treat <strong>the</strong> underlying cause of a<br />
wound. In o<strong>the</strong>r articles in this series, <strong>the</strong> literature addresses<br />
<strong>the</strong> importance of correcting factors associated with venous
leg ulcers, pressure ulcers, <strong>and</strong> foot ulcers (diabetic <strong>and</strong> o<strong>the</strong>rs).<br />
Regarding venous leg ulcers, Fletcher et al 15 reviewed six<br />
studies that compared compression versus local ulcer treatment<br />
alone without compression (eg, hydrocolloid, 16<br />
polyurethane foam, 17 <strong>and</strong> film dressing 18 ). A higher proportion<br />
of patients demonstrated healing in <strong>the</strong> six studies using<br />
compression compared to local treatments alone, <strong>and</strong> five of<br />
<strong>the</strong>se studies revealed statistical significance.<br />
Nutrition. In addition to ulcer-specific causes, <strong>the</strong><br />
patient as a whole must be examined. One factor <strong>the</strong> practitioner<br />
must consider is to determine that nutrition is adequate<br />
to produce sufficient protein to support <strong>the</strong> manufacture<br />
of granulation tissue. The patient’s weight is a good<br />
starting point. Being over- or underweight can impinge on<br />
wound healing. Patients should be as close to ideal body<br />
weight as possible. In addition to weight, protein intake also<br />
must be considered. A good intake screen for recent (<strong>the</strong><br />
past few weeks) protein consumption is pre-albumin, <strong>and</strong><br />
for more long-term protein consumption, serum albumin.<br />
An albumin of higher than 3.0 g/L is normal, but albumin<br />
levels between 2.0 g/L <strong>and</strong> 3.0 g/L may cause some delay in<br />
healing. Below 2.0 g/L, patients are malnourished <strong>and</strong> will<br />
have difficulty healing.<br />
Medications, including medical history. Ano<strong>the</strong>r factor<br />
that cannot be overemphasized is <strong>the</strong> importance of <strong>the</strong> general<br />
medical history, including a medication record. A number<br />
of medications may interfere with wound healing,<br />
including systemic steroids, immunosuppressive drugs, <strong>and</strong><br />
nonsteroidal anti-inflammatories. The presence of a major<br />
illness or systemic disease also is detrimental to healing.<br />
Rheumatoid arthritis <strong>and</strong> o<strong>the</strong>r autoimmune diseases such<br />
as systemic lupus, uncontrolled vasculitis, or pyoderma gangrenosum<br />
can all deter <strong>the</strong> wound healing process. In <strong>the</strong>se<br />
disorders, <strong>the</strong> paradox of using systemic steroids or<br />
immunosuppressive agents to control <strong>the</strong> underlying process<br />
is absolutely essential before optimal local wound healing<br />
can occur. These patients have stimulated immune systems<br />
that react against <strong>the</strong>ir own skin, <strong>and</strong> this response must be<br />
curtailed so that an orderly process of healing can occur.<br />
Recommendation 4<br />
Provide Education <strong>and</strong> Support for Patient-<br />
Centered Care to Increase Compliance/Adherence<br />
<strong>Wound</strong> care must be a partnership between healthcare<br />
professionals, patients, families, <strong>and</strong> caregivers. Patients must<br />
underst<strong>and</strong> decisions that are being made about <strong>the</strong>ir care,<br />
<strong>and</strong> <strong>the</strong>y must be part of <strong>the</strong> decisions as well. The more <strong>the</strong><br />
patient underst<strong>and</strong>s <strong>the</strong> principles involved in treatment, <strong>the</strong><br />
more likely he/she is to be compliant. Compliance should<br />
include compression b<strong>and</strong>aging for healing in patients with<br />
venous ulcers, followed by support stockings for life; <strong>the</strong><br />
patient should comprehend why this is necessary. A neurotropic<br />
foot ulcer or pressure ulcer patient who requires<br />
pressure offloading with regular monitoring <strong>and</strong> underst<strong>and</strong>s<br />
why this enhances ra<strong>the</strong>r than interferes with quality<br />
of life will have a far better approach to his/her care.<br />
Ano<strong>the</strong>r component of compliance includes selecting a<br />
treatment program that is reasonable <strong>and</strong> affordable <strong>and</strong> will<br />
facilitate an acceptable quality of life. The integration of <strong>the</strong><br />
interdisciplinary team with <strong>the</strong> patient, family, significant<br />
o<strong>the</strong>rs, <strong>and</strong> caregivers creates an optimal formula for success.<br />
Recommendation 5<br />
Debride Healable <strong>Wound</strong>s, Removing Necrotic <strong>and</strong><br />
Nonviable Tissue<br />
<strong>Debridement</strong> involves <strong>the</strong> removal of dead, devitalized, or<br />
contaminated tissue <strong>and</strong> foreign material from a wound. In<br />
chronic wounds, slough <strong>and</strong> eschar often accumulate <strong>and</strong><br />
impair healing. Natural mechanisms exist to facilitate<br />
debridement; however, studies have shown that if this<br />
process is accelerated, more rapid wound healing occurs. 19<br />
<strong>Debridement</strong> reduces wound contamination as well as<br />
removes wound debris; <strong>the</strong>reby, potentially reducing tissue<br />
destruction. Any loculated dead spaces that might o<strong>the</strong>rwise<br />
harbor bacteria <strong>and</strong> provoke frank infection need to be<br />
exposed during debridement.<br />
Several modes of debridement exist: surgical, autolytic,<br />
enzymatic, <strong>and</strong> mechanical (see Figure 2). Once a decision<br />
has been made to debride, several factors influence <strong>the</strong><br />
choice of debridement method. The use of more than one<br />
debridement method may be appropriate as outlined below<br />
(see Table 3).<br />
Surgical debridement. Surgical debridement is <strong>the</strong><br />
fastest <strong>and</strong> most effective way to remove debris <strong>and</strong> necrotic<br />
tissue. It is highly suitable in wounds with large areas of<br />
necrosis, high degrees of contamination, or frank infection.<br />
Therefore, <strong>the</strong> majority of surgical debridement tends to be<br />
performed in diabetic foot ulcers <strong>and</strong> pressure ulcers where<br />
<strong>the</strong>se criteria are commonly fulfilled. All wounds should be<br />
appropriately cleansed before debridement. Sharp, sterile<br />
surgical debridement to a bleeding base has been demonstrated<br />
by Steed et al 19 to increase <strong>the</strong> healing rate of diabetic<br />
neurotropic foot ulcers (DNFUs). This procedure not only<br />
converts a chronic, nonhealing wound into an acute wound,<br />
November 2000 Vol. 46 Issue 11 19
Non-Healable <strong>Wound</strong>s<br />
Active debridement <strong>and</strong><br />
moist interactive healing<br />
contraindicated<br />
Yes + neuropathic<br />
(especially in diabetic feet)<br />
• Level of expertise/setting<br />
• Institution/home<br />
Figure 2<br />
Debriding a wound - feedback loop for improved outcomes.<br />
but also decreases <strong>the</strong> surface bacterial burden. Before<br />
debridement, pain control may be achieved with topical,<br />
intralesional, oral, or intravenous agents. Topical EMLA 20,21<br />
(Astra-Zeneca, Wayne, Pa) can be applied in a thick coat<br />
(like icing a cake) <strong>and</strong> occluded with a transparent film<br />
dressing for 30 to 60 minutes prior to <strong>the</strong> procedure<br />
(EMLA is approved for this indication in Canada, but not<br />
in <strong>the</strong> United States). Intralesional xylocaine (with adrenaline<br />
to stop bleeding, except on distal extremities) can be<br />
20 Ostomy<strong>Wound</strong> Management<br />
Color of wound<br />
(Black or loose,<br />
yellow) or friable<br />
No<br />
No<br />
healability<br />
Patient/wound assessment<br />
• General medical status<br />
• Healability of wound, etc.<br />
Healable<br />
<strong>Wound</strong><br />
<strong>Debridement</strong><br />
Yes/No<br />
Type of debridement<br />
• Surgical<br />
• Autolytic<br />
• Enzymatic<br />
• Mechanical<br />
• <strong>Debridement</strong> not<br />
necessary<br />
• Moist interactive<br />
healing<br />
• Maintain bacterial<br />
balance<br />
Yes<br />
• Cost<br />
• Speed<br />
• Allergy<br />
• Availability<br />
• Pain<br />
Surgical preferred<br />
Reassess at regular<br />
intervals<br />
Not healing<br />
Continued healing<br />
Yes/No<br />
Healed<br />
Yes<br />
Yes<br />
No<br />
placed around <strong>the</strong> periphery of <strong>the</strong> lesion if EMLA is not<br />
available or if deeper anes<strong>the</strong>tic is required. However,<br />
surgery cannot be employed in all patients, nor can it be<br />
used in all settings (see Table 4). Blood clotting must be<br />
normal <strong>and</strong> in non-neuropathic wounds, anes<strong>the</strong>tic is often<br />
required. These factors almost dictate that significant surgical<br />
debridement, o<strong>the</strong>r than removal of devitalized tissue<br />
should be performed by a trained individual, often in a hospital<br />
or clinic setting, where facilities for achieving home-
Speed<br />
Tissue selectivity<br />
Painful wound<br />
Exudate<br />
Infection<br />
Cost<br />
TABLE 3<br />
KEY FACTORS IN DECIDING<br />
METHOD OF DEBRIDEMENT<br />
ostasis are available. Removal of devitalized tissue may only<br />
be performed by trained healthcare professionals in<br />
approved care settings.<br />
Autolytic debridement. Moist interactive dressings <strong>–</strong><br />
especially hydrogels, hydrocolloids, transparent films, <strong>and</strong><br />
alginates <strong>–</strong> can provide autolytic debridement. These dressings<br />
create an environment capable of liquifying slough <strong>and</strong><br />
promoting granulation tissue at <strong>the</strong> same time. 22,23 If tissue<br />
autolysis is not apparent in 24 to 72 hours, ano<strong>the</strong>r form of<br />
debridement should be used. The eschar surface can be<br />
scored with a scalpal blade, making superficial parallel<br />
grooves on <strong>the</strong> hard eschar surface in a grid pattern. The<br />
grooves are not intended to penetrate viable tissue, <strong>and</strong><br />
bleeding should be minimal or absent.<br />
Enzymatic debridement. The most selective mode of<br />
debridement <strong>–</strong> enzymatic debridement <strong>–</strong> relies on<br />
naturally occurring enzymes applied exogenously to<br />
<strong>the</strong> wound surface to degrade debris. In Canada, <strong>the</strong><br />
only licensed enzymatic product is collagenase, isolated<br />
from Clostridium histolyticum. Collagenase exists in<br />
wounds naturally as a matrix metalloproteinase, where<br />
it has been shown to degrade immature collagen in<br />
<strong>the</strong> wound matrix. Early debridement is promoted<br />
because collagenase acts as <strong>the</strong> rate-determining<br />
enzyme in collagen degradation, catalyzing cleavage of<br />
glycine in <strong>the</strong> native collagen triple helix. It is highly<br />
specific for collagen <strong>and</strong> is thought to promote<br />
debridement by digesting collagen bundles that bind<br />
nonviable tissue to <strong>the</strong> wound bed. Some small trials<br />
report faster debridement with collagenase compared<br />
to placebo. 24,25 Future trials are needed to confirm if<br />
this agent has a role promoting later stages to stimulate<br />
granulation tissue <strong>and</strong> re-epi<strong>the</strong>lialization. 26<br />
22 Ostomy<strong>Wound</strong> Management<br />
Surgical Enzymatic Autolytic Mechanical<br />
1*<br />
2<br />
4<br />
1<br />
1<br />
4<br />
* 1 is usually most desirable, <strong>and</strong> 4 is usually least desirable.<br />
2<br />
1<br />
2<br />
4<br />
3<br />
2<br />
4<br />
3<br />
1<br />
3<br />
4<br />
1<br />
3<br />
4<br />
3<br />
2<br />
2<br />
3<br />
Collagenase is inactivated by heavy metals<br />
(silver, zinc) <strong>and</strong> detergents. In <strong>the</strong> Unites<br />
States, papain <strong>and</strong> papain-urea products<br />
are also available. 27<br />
Enzymatic debridement appears to be<br />
most useful in <strong>the</strong> removal of eschar from<br />
large wounds when surgical techniques<br />
cannot be utilized. <strong>Debridement</strong> can be<br />
facilitated by cross-hatching or scoring<br />
hard eschar prior to application of <strong>the</strong><br />
enzyme. Problems arising from enzymatic<br />
debridement relate to <strong>the</strong> production of<br />
excessive amounts of exudate with <strong>the</strong>se<br />
agents, local irritation to surrounding<br />
skin, <strong>and</strong> possible infection.<br />
Mechanical debridement. Mechanical debridement<br />
physically removes debris from <strong>the</strong> wound. It may be used<br />
in <strong>the</strong> management of surgical wounds along with pressure,<br />
ischemic, <strong>and</strong> venous leg ulcers. The simplest form of<br />
mechanical debridement is wet-to-dry gauze, but this technique<br />
is nursing time-intensive <strong>and</strong> costly. This often causes<br />
bleeding <strong>and</strong> pain with removal, leading to nonselective<br />
trauma to <strong>the</strong> wound. O<strong>the</strong>r methods include irrigation,<br />
pulsatile lavage, <strong>and</strong> whirlpool <strong>the</strong>rapy. 27,28 In <strong>the</strong> whirlpool<br />
or o<strong>the</strong>r foot-soaking procedures, <strong>the</strong> entire foot is<br />
immersed, causing <strong>the</strong> maceration <strong>and</strong> bacterial seeding<br />
(bacterial soup) of susceptible areas such as <strong>the</strong> toe webs,<br />
nail folds, <strong>and</strong> tiny cracks in <strong>the</strong> skin (fissures). (See<br />
Recommendation 9 of Best Practices for <strong>the</strong> Prevention <strong>and</strong><br />
Treatment of Pressure Ulcers by Dolynchuk et al on page 46.)<br />
TABLE 4<br />
CONTRAINDICATIONS FOR SURGICAL<br />
DEBRIDEMENT OF VIABLE TISSUE<br />
Absolute Contraindications<br />
• Lack of expertise in procedure<br />
• Nonhealable ulcer (ie, insufficient vascular supply to<br />
allow healing)<br />
• Septicemia in <strong>the</strong> absence of systemic antibacterial<br />
coverage<br />
• Medically unfit patient<br />
Relative Contraindications<br />
• Patient on anticoagulants (dependent on INR [international<br />
normal ratio]/PTT [activated partial prothrombin<br />
time] etc.)<br />
• Home care setting
Recommendation 6<br />
Assess <strong>the</strong> <strong>Wound</strong> for <strong>Bacterial</strong> <strong>Balance</strong> <strong>and</strong><br />
Infection<br />
The presence of wound-associated bacteria alone does not<br />
indicate infection or impaired wound healing. Indeed, some<br />
authors have suggested that a small amount of a certain bacteria<br />
species in a chronic wound facilitates healing. 29,30 In<br />
clinical practice, assessing when a wound has moved from a<br />
symbiotic bacterial load that does not cause tissue damage to<br />
an increased bioburden causing impairment of wound healing<br />
can be difficult. The following equation demonstrates<br />
that although bacterial quantity <strong>and</strong> virulence are significant<br />
in assessing a wound for infection, host factors are of overriding<br />
importance.<br />
Risk of wound infection 31 = <strong>Bacterial</strong> dose x virulence<br />
Host resistance<br />
Factors such as immunosuppression, diabetes, <strong>and</strong> medication<br />
all can influence whe<strong>the</strong>r any bacteria present will<br />
impair wound healing. Fur<strong>the</strong>rmore, <strong>the</strong>se factors can act to<br />
mask classical signs of infection such as ery<strong>the</strong>ma, increased<br />
temperature, pain, <strong>and</strong> edema.<br />
Swab technique is important to obtain meaningful<br />
results. 32 The wound should be cleansed with saline or water<br />
<strong>and</strong> all debris should be removed. The healthy appearing<br />
granulation is swabbed in a zigzag pattern, gently rotating<br />
<strong>the</strong> tip of <strong>the</strong> swab (swabs are only recommended if clinically<br />
indicated). If <strong>the</strong> wound is relatively dry, <strong>the</strong> swab may be<br />
moistened with <strong>the</strong> transport media prior to swabbing. A<br />
semiquantitative swab is <strong>the</strong>n inoculated on st<strong>and</strong>ard media<br />
in <strong>the</strong> lab <strong>and</strong> streaked in four quadrants. Results will indicate<br />
no growth to 1 to 4+ growth of an organism, depending<br />
on <strong>the</strong> number of streaked quadrants that support bacterial<br />
growth. These swabs are quick <strong>and</strong> inexpensive. The<br />
semiquantitative swab correlates well to <strong>the</strong> gold st<strong>and</strong>ard<br />
quantitative biopsy results, 33 but <strong>the</strong>re is some loss of specificity.<br />
Despite <strong>the</strong> fact this is <strong>the</strong> procedure of choice in<br />
most centers, inadequate wound bed preparation will result<br />
in an excess number of confusing, nonsignificant wound<br />
surface colonies appearing on <strong>the</strong> agar plates in <strong>the</strong> lab. The<br />
clinical assessment of wound bioburden <strong>and</strong> <strong>the</strong> choice <strong>and</strong><br />
route of antibacterial agents should be based on host <strong>and</strong><br />
wound factors in association with wound swab results.<br />
The concepts of bacterial contamination, colonization,<br />
critical colonization, <strong>and</strong> local <strong>and</strong> systemic infection lend<br />
<strong>the</strong>mselves to guidance with regard to when to use antimicrobial<br />
agents in wound care (see Table 5).<br />
Most wounds are contaminated <strong>and</strong> contain nonreplicat-<br />
24 Ostomy<strong>Wound</strong> Management<br />
ing organisms. Colonization occurs when organisms are<br />
replicating but not causing host injury. Skin commensals<br />
such as Staphylococcus epidermidis <strong>and</strong> Corynebacterium<br />
species are <strong>the</strong> most common colonizers. Nei<strong>the</strong>r contaminated<br />
nor colonized wounds show signs of infection, <strong>and</strong><br />
impairment of wound healing is unlikely. The concept of<br />
critical colonization (increased bacterial burden) has recently<br />
been introduced to describe wounds moving between <strong>the</strong><br />
spectrums of colonization (where <strong>the</strong> host is unaffected) <strong>and</strong><br />
local infection (in which host injury occurs). It has been<br />
suggested that during critical colonization, subtle clinical<br />
signs of infection such as increasing pain/tenderness, increasing<br />
serous exudate <strong>and</strong> friable granulation tissue, or failure<br />
to heal may be present prior to <strong>the</strong> classical signs of foul<br />
odor, frank pus, surrounding ery<strong>the</strong>ma, increased temperature,<br />
pain, <strong>and</strong> swelling associated with infection. 34 It is<br />
important to emphasize that many people with chronic<br />
wounds, in particular people with diabetes, have an<br />
impaired host response. These patients may <strong>the</strong>refore exhibit<br />
only subtle signs, or even have a complete absence of signs<br />
of infection (ie, no elevation in temperature) when bacteria<br />
are damaging <strong>the</strong> skin <strong>and</strong> delaying healing. 35 A semiquantitative<br />
swab with 4+ growth of a significant pathogen or a<br />
quantitative biopsy with ≥ 1.0 x 10 6 cfu/g (cfu = colony<br />
forming unit) of tissue in <strong>the</strong> presence of nonhealing may be<br />
an indication for systemic antibacterial <strong>the</strong>rapy. Therefore,<br />
host monitoring is a vital part of assessment, with factors<br />
such as raised blood sugar levels in people with diabetes<br />
often being a helpful indicator of local or systemic infection.<br />
Recommendation 7<br />
Cleanse <strong>Wound</strong>s with Normal Saline or Water. The<br />
Use of Topical Antiseptics Should be Reserved for<br />
<strong>Wound</strong>s that are Nonhealable or <strong>the</strong> Local <strong>Bacterial</strong><br />
Burden is a Greater Concern than <strong>the</strong> Stimulation<br />
of Healing<br />
Cleansing <strong>and</strong> irrigation are used to eliminate exudate<br />
<strong>and</strong> surface debris from wounds. Not only does this process<br />
facilitate healing, but it also decreases bacterial burden by<br />
removing heavily contaminated surface slough <strong>and</strong> debris.<br />
Saline or sterile water are agents of choice for most<br />
wounds. Tap water should not be used for immunosuppressed<br />
patients <strong>and</strong> <strong>the</strong> water source should be reliably<br />
clean before advocating it as treatment in o<strong>the</strong>r chronic<br />
wounds. 36<br />
Rodeheaver 28 studied wound cleansers in vitro to assess<br />
cellular toxicity. He concluded that nonionic agents are best,
<strong>Bacterial</strong> burden<br />
<strong>Wound</strong> clinical symptoms<br />
<strong>and</strong> signs<br />
<strong>Bacterial</strong> C & S*<br />
Topical<br />
antibiotic/antibacterial<br />
Systemic<br />
antibiotic/antibacterial<br />
Enzymatic<br />
debridement<br />
Surgical debridement<br />
* Culture <strong>and</strong> sensitivity<br />
TABLE 5<br />
ASSESSMENT OF AND INTENTION TO TREAT INFECTION<br />
IN CHRONIC WOUNDS<br />
Contaminated<br />
<strong>Wound</strong><br />
progressing<br />
Host stable<br />
but <strong>the</strong>ir toxicity index is still greater than saline. There are<br />
four main methods of cleansing. Healthcare practitioners<br />
who cleanse wounds can a) use a saline moist gauze to soak<br />
or compress a wound; b) gently pour a solution over a<br />
wound; c) irrigate <strong>the</strong> wound with a piston or bulb syringe<br />
<strong>–</strong> 5 to 8 pounds per square inch (psi) for cleansing with a<br />
bulb syringe or 5 to 15 psi to remove slough or eschar with<br />
an 18- to 20-gauge angiocath (venous access device) <strong>and</strong> 30cc<br />
syringe held 4 to 6 inches from <strong>the</strong> wound; <strong>and</strong> d) use an<br />
appropriate commercially prepared spray cleanser with predetermined<br />
average psi. When higher pressures are used,<br />
splash back commonly occurs <strong>and</strong> healthcare providers<br />
should take appropriate precautions.<br />
Antiseptic agents are used primarily to decrease bacterial<br />
growth on inanimate objects. When <strong>the</strong>y are used in<br />
wounds, <strong>the</strong>y have antibacterial properties, but <strong>the</strong>y also<br />
inhibit healing (cytotoxic properties. See Table 6).<br />
If a wound does not have enough blood supply to heal, a<br />
patient is immunosuppressed, or in negative protein balance,<br />
<strong>the</strong> prime objective may be to reduce bacterial burden.<br />
Tissue toxicity is not <strong>the</strong> prime concern. Antiseptics would<br />
<strong>the</strong>n be indicated with <strong>the</strong> precautions outlined in Table 6.<br />
Providone/iodine or chlorhexidine would be <strong>the</strong> agent of<br />
first choice for most nonhealing wounds (to dry <strong>the</strong> surface,<br />
decrease surface bacteria).<br />
No<br />
No<br />
No<br />
No<br />
+/-<br />
Colonized<br />
+/- early signs of<br />
local infection<br />
+/-C & S wound<br />
+/-<br />
No<br />
+/-<br />
+/-<br />
Critically colonized<br />
No/subtle signs <strong>and</strong><br />
symptoms of<br />
infection<br />
C & S wound<br />
Yes<br />
+/-<br />
+/-<br />
+/-<br />
Local infection<br />
Local signs <strong>and</strong><br />
symptoms of<br />
infection<br />
C & S wound<br />
Yes<br />
+/-<br />
No<br />
Yes<br />
Systemic infection<br />
Constitutional signs<br />
<strong>and</strong> symptoms of<br />
infection<br />
C & S wound<br />
Blood culture<br />
Yes<br />
Recommendation 8<br />
If Methicillin Resistant Staphylococcus Aureus is<br />
Present, Assess <strong>the</strong> Patient for Colonization or<br />
Infection. Select Appropriate Topical <strong>and</strong>/or Systemic<br />
Agents for Treatment<br />
With <strong>the</strong> development of increasing bacterial resistance,<br />
it is important to restrict <strong>the</strong> use of antibiotics to<br />
situations where <strong>the</strong>y are definitely indicated <strong>and</strong> fur<strong>the</strong>rmore,<br />
to use <strong>the</strong> narrowest spectrum of antibiotic<br />
possible.<br />
Methicillan-resistant Staphylococcus aureus (MRSA) is a<br />
very common cause of hospital-acquired infections.<br />
Unfortunately, <strong>the</strong>se bacteria can commonly develop<br />
resistance to antibiotics. The most important of <strong>the</strong>se is<br />
MRSA. Bacteria develop resistance to methicillin <strong>and</strong> to<br />
o<strong>the</strong>r families of antibiotics. Some strains of MRSA can<br />
spread from patient to patient very readily <strong>and</strong> have been<br />
labeled epidemic MRSA.<br />
Methicillan-resistant Staphylococcus aureus is commonly<br />
found in ulcers, <strong>and</strong> although its presence in wounds rarely<br />
causes death, cross infection into immunocompromised<br />
hosts can be fatal. It is <strong>the</strong>refore <strong>the</strong> responsibility of healthcare<br />
professionals to try to minimize <strong>the</strong> risk of <strong>the</strong> development<br />
of resistant microorganisms <strong>and</strong> <strong>the</strong>ir subsequent<br />
spread.<br />
Yes<br />
No<br />
Yes<br />
November 2000 Vol. 46 Issue 11 25
The pathogenicity of MRSA may not be significantly different<br />
from traditional S. aureus infections, but <strong>the</strong>se infections<br />
may be difficult to control. The incidence of MRSA is<br />
on <strong>the</strong> increase in many countries. Unfortunately, healthcare<br />
providers, through direct contact with patients, may spread<br />
MRSA from nasal colonization (20% of people are persistent<br />
carriers, 60% intermittent carriers, <strong>and</strong> <strong>the</strong> remainder<br />
often never carry <strong>the</strong> organism). The treatment of MRSA<br />
may vary, depending upon whe<strong>the</strong>r it has colonized or<br />
infected <strong>the</strong> wound. For topical colonization, mupirocin has<br />
been <strong>the</strong> traditional agent of choice. However, with overuse<br />
of mupirocin, resistance in some centers has been documented.<br />
37 The use of mupirocin should be limited <strong>and</strong><br />
reserved predominantly for <strong>the</strong> treatment of MRSA. As<br />
alternatives to mupirocin in healable wounds, cadexomer<br />
iodine <strong>and</strong> new ionized silver technologies have been very<br />
successful in eliminating colonization. These nonantibiotic<br />
alternatives are effective against MRSA <strong>and</strong> can be used to<br />
minimize <strong>the</strong> risk of provoking resistance. Ionized silver <strong>and</strong><br />
cadexomer iodine depend on three separate antibacterial<br />
actions (cell membrane, cytoplasmic organelles, nucleic<br />
acid); <strong>the</strong>refore, resistance is highly unlikely to develop.<br />
Colonization also can be eliminated by <strong>the</strong> use of<br />
systemic antibiotics in combination. One protocol calls<br />
26 Ostomy<strong>Wound</strong> Management<br />
TABLE 6<br />
WOUND ANTISEPTIC AGENTS <strong>–</strong> ALL TOXIC TO HEALTHY<br />
GRANULATION TISSUE<br />
Hypochlorite solution<br />
Hydrogen peroxide<br />
Proflavine, mercuric chloride/crystal<br />
violet plus o<strong>the</strong>r analine dyes<br />
Cetrimide (quaternary ammonium)<br />
Chlorhexidine (plus cetrimide =<br />
Savalon TM [Astra-Zeneca,Wayne,<br />
Pa])<br />
Acetic acid 0.5% <strong>–</strong> 5.0%<br />
Providone/iodine (Agent of choice in<br />
most nonhealing wounds)<br />
Irritating to skin due to high pH. Buffered preparations<br />
- Dakins/ Eusol <strong>–</strong> often select out Gram<br />
negatives<br />
De-sloughing agent when effervescent (few seconds).<br />
It can harm healthy granulation <strong>and</strong> may<br />
form air emboli if packed in deep, closed spaces<br />
Bacteriostatic agents against Gram positives only<br />
Gram-positive <strong>and</strong> negative organisms <strong>–</strong> detergent<br />
effect <strong>–</strong> but high tissue toxicity<br />
Gram-positive <strong>and</strong> negative action with residual<br />
effect on tissue<br />
Low pH effective vs pseudomonas but may select out<br />
S. aureus<br />
Broad spectrum of activity (Gram-positive, Gramnegative,<br />
anaerobes, yeast), but this is decreased<br />
in <strong>the</strong> presence of pus or wound exudate. Iodine<br />
toxicity reported if use prolonged or over large<br />
areas<br />
for <strong>the</strong> use of rifampin with ei<strong>the</strong>r minocycline or clotrimoxazole.<br />
Infection may require intravenous treatment<br />
with vancomycin. Depending on individual sensitivities,<br />
o<strong>the</strong>r antibiotic combinations may work on<br />
some patients. Because MRSA is stored in <strong>the</strong> gut,<br />
recurrences are common, <strong>and</strong> it is important to monitor<br />
<strong>the</strong>se patients at regular intervals. The nosocomial<br />
spread of MRSA has been well documented in one<br />
author’s unit, <strong>and</strong> <strong>the</strong> use of double barriers such as<br />
h<strong>and</strong>washing <strong>and</strong> soapless cleansers should be encouraged<br />
for staff moving between patients with wounds.<br />
Documentation of MRSA on tape-measuring guides<br />
<strong>and</strong> o<strong>the</strong>r instruments that move from patient to<br />
patient also illustrates <strong>the</strong> importance of decontaminating<br />
<strong>the</strong> environment as well as implementing a rigorous<br />
h<strong>and</strong>washing routine.<br />
Patients with MRSA should have cultures from three<br />
sites (nares, rectum, <strong>and</strong> <strong>the</strong> wound). These cultures<br />
should be repeated at regular intervals until <strong>the</strong>y are<br />
negative on three occasions, <strong>the</strong>n long-term monitoring<br />
is indicated. A modified protocol from <strong>the</strong> Peel<br />
Interdisciplinary <strong>Wound</strong> Healing Committee has been<br />
reproduced with <strong>the</strong> permission of Caremark (see<br />
Figure 3).
Serious infection consult<br />
Hospitalization<br />
Recommendation 9<br />
Use Only Nonsensitizing Topical Antimicrobial<br />
Agents for Local Symptoms <strong>and</strong> Signs of Infection or<br />
Increased <strong>Bacterial</strong> Burden<br />
Once <strong>the</strong> decision to use topical antimicrobial agents has<br />
been made, <strong>the</strong> healthcare provider is faced with choosing<br />
an antimicrobial agent. The aim is to reduce bioburden, <strong>and</strong><br />
<strong>the</strong> principle factor influencing choice is <strong>the</strong> offending<br />
organism (see Table 7). This information is usually gained<br />
from bacteriology results; however, clinical judgment can<br />
often detect <strong>the</strong> presence of some organisms such as<br />
Pseudomonas. These can be recognized by <strong>the</strong>ir distinctive<br />
odor <strong>and</strong> a greenish tinge. Anaerobes can be assumed to be<br />
present in a wound with an accompanying putrid odor or a<br />
wound duration of longer than 1 month. 38<br />
MRSA Isolated Through Culture<br />
Infected Colonized<br />
Infectious diseases consult<br />
Treatment based on sensitivity<br />
results: may include IV vancomycin<br />
Less serious infection<br />
• Mupirocin anterior nares if positive.<br />
Topical treatment or systemic treatment<br />
to o<strong>the</strong>r sites<br />
• 2% chlorhexidine soap for all<br />
washing/bathing for duration of<br />
treatment<br />
Culture anterior nares, perianal<br />
<strong>and</strong> open wounds within 48<br />
hours of completed treatment<br />
Repeat cultures weekly x 3<br />
before labeling “cleared”<br />
Treatment options based on sensitivity<br />
results:<br />
• Oral fusidic acid <strong>and</strong> rifampin<br />
• Rifampin <strong>and</strong> one of minocycline<br />
or clotrimoxazole<br />
Positive culture<br />
Positive:<br />
• (Consider) infectious<br />
disease consult<br />
• Treatment options as<br />
per sensitivity results<br />
Consider decolonization <strong>the</strong>rapy<br />
(individual decision)<br />
• Mupirocin (Bactroban) ointment<br />
to anterior nares/wounds <strong>and</strong><br />
oral/topical agents for o<strong>the</strong>r sites if<br />
appropriate (see Table 7)<br />
• 2% chlorhexidine soap for all<br />
washing/bathing x 7<strong>–</strong>10 days<br />
Repeat culture of anterior nares,<br />
perianal <strong>and</strong> open wounds 48<br />
hours after treatment completed<br />
Treatment options based on<br />
sensitivity results:<br />
• Oral fusidic acid <strong>and</strong> rifampin<br />
• Rifampin <strong>and</strong> one of<br />
minocycline or clotrimoxazole<br />
Negative:<br />
Repeat cultures<br />
weekly x 3 before<br />
labeling “cleared”<br />
Negative culture<br />
Repeat cultures<br />
weekly x 3 before<br />
labeling “cleared”<br />
Figure 3.<br />
<strong>Wound</strong> management for patients infected or colonized with MRSA.Copyright 1998, Caremark Ltd. Adapted with permission.<br />
Hospital: repeat cultures<br />
once a month.<br />
Nursing homes <strong>and</strong><br />
community: repeat every<br />
3 to 6 months<br />
One o<strong>the</strong>r factor to consider when applying topical<br />
agents to an ulcer is <strong>the</strong> propensity to induce sensitization<br />
that can elicit an allergic contact dermatitis. Neomycin,<br />
lanolin, <strong>and</strong> perfumes, which can be present in topical<br />
antimicrobial vehicles, are common sensitizers <strong>and</strong> should<br />
be avoided. 39 Similarly, ointments ra<strong>the</strong>r than creams should<br />
be used to reduce exposure to preservatives that can also act<br />
as sensitizers.<br />
Two products listed in Table 7 combine antibacterial<br />
properties with moist interactive healing. Cadexomer iodine<br />
(Iodosorb ® , Iodoflex ® ; Healthpoint, Fort Worth, Tex./Smith<br />
<strong>and</strong> Nephew, Hall, U.K.) is composed of microspheres of<br />
starch crosslinked with e<strong>the</strong>r bridges <strong>and</strong> iodine. This product<br />
absorbs moisture up to seven times its weight in water<br />
<strong>and</strong> slowly releases iodine for antibacterial action that is not<br />
November 2000 Vol. 46 Issue 11 27
Safe <strong>and</strong> Effective<br />
Selected Use<br />
Caution<br />
Cadexomer iodine<br />
Ionized silver<br />
Silver sulphadiazine<br />
Polymyxin B sulphate<br />
<strong>–</strong> Bacitracin<br />
zinc<br />
Mupirocin<br />
Metronidazole<br />
Benzoyl peroxide<br />
Gentamicin<br />
Fucidin<br />
Polymyxin B sulphate<br />
<strong>–</strong> Bacitracin<br />
zinc neomycin<br />
+ = effective against bacteria<br />
strong enough for cytoxicity. It should be used with caution<br />
in patients with thyroid disease <strong>and</strong> iodine allergy. If cadexomer<br />
iodine is used on large areas or for long periods, monitoring<br />
of thyroid function is advised.<br />
Ionized silver dressing (Acticoat ; Westaim Biomedical,<br />
Exeter, NH, Fort Saskatchewan, Alberta, Canada) has a slow<br />
release of silver, combined with an absorptive polyester pad.<br />
The silver has a broad spectrum of antibacterial coverage<br />
<strong>and</strong> can be used very successfully to decrease friable exudative<br />
tissue on <strong>the</strong> wound surface. Acticoat must be used<br />
with sterile water because <strong>the</strong> chloride in saline precipitates<br />
<strong>the</strong> silver to inactive silver chloride. Acticoat contains no<br />
sulfa, which may be present in o<strong>the</strong>r silver preparations.<br />
Topical antibacterials will only treat <strong>the</strong> wound surface<br />
<strong>and</strong> not deeper infection. Their use should be re-evaluated<br />
after 2 weeks or if symptoms or signs of deeper infection<br />
occur. 40<br />
Recommendation 10<br />
Use Systemic Antibiotics if Symptoms or Signs of<br />
28 Ostomy<strong>Wound</strong> Management<br />
TABLE 7<br />
CHOOSING APPROPRIATE ANTIMICROBIALS<br />
Staphylococcus<br />
aureus<br />
+<br />
+<br />
+<br />
+<br />
Weak<br />
+<br />
+<br />
+<br />
MRSA Streptococcus Pseudomonas Anaerobes<br />
+<br />
+<br />
+<br />
+<br />
+<br />
Weak<br />
+<br />
+<br />
+<br />
+<br />
+<br />
Weak<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
Weak<br />
+<br />
Comments<br />
Good autolytic debridement;<br />
limited potential for bacterial<br />
resistance. Caution with<br />
thyroid disease<br />
Use with water, not saline.<br />
Limited potential for bacterial<br />
resistance<br />
Not for use in sulfa<strong>–</strong>sensitive<br />
patients<br />
Reserve for MRSA <strong>and</strong> o<strong>the</strong>r<br />
resistant Gram-positive<br />
organisms<br />
Reserve for anaerobes <strong>and</strong><br />
odor control<br />
For use on large wounds. Can<br />
cause irritation/allergies<br />
Reserve for oral/IV use<br />
Ointment contains lanolin,<br />
which can sensitize to cause<br />
allergic contact dermatitis<br />
Contains neomycin, which<br />
causes an allergic contact<br />
dermatitis, may cross sensitize<br />
to aminoglycosides<br />
Infection Extend Beyond <strong>Wound</strong> Margin or <strong>the</strong><br />
Ulcer Probes to Bone<br />
Systemic antibiotics should be used if infection extends<br />
beyond <strong>the</strong> ulcer margin. Ulcers of less than 1-month duration<br />
require primary Gram-positive coverage primarily for at<br />
least 2 weeks or until clinical symptoms <strong>and</strong> signs resolve. If<br />
immunosuppression is an issue, broad spectrum agents,<br />
including Gram-negatives <strong>and</strong> anaerobes, should be included.<br />
A semiquantitative swab is often helpful when patients<br />
fail to respond to <strong>the</strong> initial <strong>the</strong>rapy. In complex cases, an<br />
infectious disease consult is advised.<br />
If an ulcer probes to bone, osteomyelitis must be suspected.<br />
Antibiotics for longer periods are necessary, usually for at<br />
least 4 to 6 weeks. Treatment progress can be monitored<br />
with x-rays, erythrocyte sedimentation rate, C reactive protein,<br />
<strong>and</strong>, rarely, nuclear scans. Nonhealing ulcers may<br />
require surgical debridement. For a more detailed discussion<br />
on this topic, see Recommendation 8 of Best Practices for <strong>the</strong><br />
Prevention, Diagnosis, <strong>and</strong> Treatment of Diabetic Foot Ulcers<br />
by Inlow et al on page 63.
Recommendation 11<br />
Select Appropriate Dressing for Local Moisture<br />
<strong>Balance</strong> to Stimulate Granulation Tissue <strong>and</strong><br />
Re-epi<strong>the</strong>lialization<br />
Compared to dry wounds, a moist wound environment<br />
accelerates wound healing by as much as 50%, often with<br />
more rapid epi<strong>the</strong>lialization. 41 Using clinical judgment to<br />
select a type of moist wound dressing suitable for an ulcer is<br />
important. Seven dressing recommendations have been put<br />
forward since <strong>the</strong> Agency for Health Care Policy <strong>and</strong><br />
Research guidelines came out in 1994. 42 They were published<br />
in Ostomy/<strong>Wound</strong> Management by Liza Ovington in<br />
1999, 43 <strong>and</strong> are discussed below:<br />
1. Use a dressing that will keep <strong>the</strong> wound bed continuously<br />
moist. Wet-to-dry saline dressings are not considered continuously<br />
moist <strong>and</strong> should be used only for debridement.<br />
Kim 44 reported that occlusive hydrocolloid dressings for <strong>the</strong><br />
treatment of Stage I <strong>and</strong> II pressure ulcers were less timeconsuming<br />
<strong>and</strong> less expensive, compared to saline-soaked<br />
gauze dressings. Colwell’s trial showed that a hydrocolloid<br />
dressing increased healing rate <strong>and</strong> was less costly than moist<br />
gauze dressings. 45 If saline-soaked gauze is used, it must be<br />
moist with frequent dressing changes or harm may result.<br />
2. Use clinical judgment to select a type of moist wound<br />
dressing suitable for an ulcer. Studies of different types of<br />
moist wound dressings showed no differences in pressure<br />
ulcer healing outcomes. Mulder 46 looked at three types of<br />
dressings, all providing moist wound healing, <strong>and</strong> found no<br />
statistical differences with wound healing.<br />
3. Choose a dressing that keeps <strong>the</strong> surrounding peri-ulcer<br />
skin dry while keeping <strong>the</strong> ulcer bed moist.<br />
4. Choose a dressing that controls exudate but does not<br />
desiccate <strong>the</strong> ulcer bed. If <strong>the</strong> exudate is not controlled, it<br />
will come in contact with <strong>the</strong> surrounding peri-ulcer skin<br />
<strong>and</strong> cause maceration, which could lead to breakdown <strong>and</strong><br />
fur<strong>the</strong>r deterioration of <strong>the</strong> wound. There must be a balance<br />
in choosing a dressing to avoid drying of <strong>the</strong> wound surface.<br />
Continuous assessment of <strong>the</strong> wound <strong>and</strong> changes in <strong>the</strong><br />
dressing material used is needed to achieve optimal moisture<br />
balance. Maceration may be controlled by certain dressing<br />
materials that provide a vertical wicking <strong>and</strong> trap <strong>the</strong> wound<br />
fluid in <strong>the</strong> matrix of <strong>the</strong> dressing (ie, calcium alginate<br />
ropes, hydrofibers).<br />
5. Consider caregiver time when selecting a dressing. A<br />
dressing that is easier to apply <strong>and</strong> does not require frequent<br />
changes decreases <strong>the</strong> healthcare provider’s workload <strong>and</strong> <strong>the</strong><br />
financial burden to <strong>the</strong> patient, family, <strong>and</strong> society. 6.<br />
30 Ostomy<strong>Wound</strong> Management
Absorbent<br />
Membrane<br />
Dressing Category<br />
1. Foam<br />
2. Hydrofiber<br />
3. Crystalline<br />
NaCl gauze<br />
4. Calcium alginate<br />
5. Hydrocolloid<br />
6. Hydrogel<br />
7.Adhesive film<br />
8. Nonadhesive film<br />
9. Enzymes<br />
+ = usually appropriate<br />
++= appropriate<br />
+++= highly appropriate<br />
Eliminate wound dead space by loosely filling all cavities<br />
with dressing material. Avoid overpacking <strong>the</strong> wound.<br />
Stotts 47 reports that increased bacterial invasion <strong>and</strong><br />
impaired healing results from unfilled dead space. Tightly<br />
packing <strong>the</strong> wound causes pressure on <strong>the</strong> newly formed<br />
granulation tissue <strong>and</strong> may cause damage that will prevent<br />
or delay healing. Overpacking may decrease absorbent<br />
capacity of <strong>the</strong> dressing material by not allowing <strong>the</strong> dressing<br />
to absorb <strong>the</strong> wound fluid.<br />
7. Because <strong>the</strong>y are difficult to keep intact, monitor dressings<br />
applied near <strong>the</strong> anus. Day et al 48 found that choosing a<br />
dressing specifically designed for <strong>the</strong> sacral area improves<br />
wear time <strong>and</strong> healing rate on full-thickness pressure ulcers.<br />
Specifically, a triangular-shaped dressing will fit better with<br />
<strong>the</strong> tip toward <strong>the</strong> anus. Shearing <strong>and</strong> friction forces are<br />
tremendously high in <strong>the</strong> sacral area, causing rolling <strong>and</strong><br />
bunching of <strong>the</strong> dressing.<br />
To date, no one dressing will complete all <strong>the</strong> outlined<br />
requirements. The three absorbent dressing groups are foams,<br />
hydrofibers, <strong>and</strong> crystalline NaCl gauze (see Table 8).<br />
Foams 49,50 provide <strong>the</strong>rmal insulation, high absorbency, a<br />
moist environment, <strong>and</strong> are gas permeable. They are also<br />
nonadherent, easy to cut <strong>and</strong> shape, <strong>and</strong> do not shed fibers.<br />
Some foams have additional wound contact layers to avoid<br />
adherence when <strong>the</strong> wound is overly dry <strong>and</strong> a polyurethane<br />
TABLE 8<br />
CHOOSING APPROPRIATE DRESSINGS<br />
Appearance of <strong>Wound</strong> <strong>Bed</strong> Appearance of Granulation Tissue<br />
Black<br />
(Necrotic)<br />
+<br />
++<br />
+++<br />
Yellow<br />
(Dry)<br />
++<br />
+++<br />
+++<br />
Sloughy<br />
(Moist)<br />
++<br />
+++<br />
+++<br />
++<br />
+<br />
++<br />
++<br />
Red<br />
(Infected)<br />
++<br />
++<br />
+++<br />
+++<br />
+<br />
Red<br />
(Wet)<br />
+++<br />
+++<br />
++<br />
+++<br />
++<br />
Red<br />
(Bleeding)<br />
+<br />
+++<br />
+<br />
Pink/Purple<br />
(healthy granulation/<br />
re-epi<strong>the</strong>lialization)<br />
++<br />
+++<br />
+++<br />
+++<br />
backing to prevent excessive fluid loss. Crystalline sodium<br />
chloride gauze (pledgit or packing) is used for highly exudative<br />
wounds, mechanical debridement, <strong>and</strong> for its antibacterial<br />
properties. Hydrofibers have high absorbency, good tensile<br />
strength, <strong>and</strong> contain <strong>the</strong> fluid within <strong>the</strong> fiber. They do not<br />
provide a fluid equilibrium with <strong>the</strong> wound surface as would<br />
occur with foam dressing. Foams <strong>and</strong> hydrofibers have long<br />
wear times (up to 1 week) but crystalline sodium chloride<br />
gauze should be changed daily.<br />
Calcium alginates 51 are derived from brown seaweed<br />
(kelp). Some alginates have a high content of mannuronic<br />
acid (high gelling property for autolytic debridement) <strong>and</strong><br />
o<strong>the</strong>rs have a high galuronic acid content (high fiber integrity<br />
for packing sinuses). 52 Calcium alginates are marketed in<br />
ropes (vertical wicking best for hemostasis) <strong>and</strong> wafers (lateral<br />
wicking to remove surface exudate). The calcium alginates<br />
are excellent for hemostasis postdebridement. The calcium<br />
alginate donates calcium for ion exchange to <strong>the</strong> wound<br />
fluid to promote hemostasis <strong>and</strong> accepting sodium ion,<br />
causing <strong>the</strong> alginate to form a hydrogel for moist interactive<br />
healing. 53,54 No crust is formed, <strong>and</strong> <strong>the</strong> wound can progress<br />
from <strong>the</strong> inflammatory to <strong>the</strong> proliferative stage. If <strong>the</strong> fiber<br />
is intact with dressing change, <strong>the</strong>n <strong>the</strong> exudate is not sufficient.<br />
Ano<strong>the</strong>r dressing class should be chosen for subsequent<br />
dressings. Alginates are excellent for infected wounds,<br />
++<br />
November 2000 Vol. 46 Issue 11 31
ut systemic antibiotics are needed if deeper tissue symptoms<br />
<strong>and</strong> signs are present (see Recommendations 6 <strong>and</strong> 9).<br />
Hydrogels 53-56 provide a high concentration of water in<br />
insoluble polymers. They may be syn<strong>the</strong>tic or semisyn<strong>the</strong>tic<br />
with bases of propylene glycol, saline, or hydrocolloids.<br />
They are inert to normal biological processes <strong>and</strong> permeable<br />
to metabolites with some absorptive <strong>and</strong> water-donating<br />
properties. They are best in dry, sloughy wounds with low<br />
exudate levels. They require changing every 24 to 72 hours<br />
<strong>and</strong> have very little anti-infective properties. They are available<br />
in amorphous or sheet forms.<br />
Hydrocolloids 57 are occlusive dressings containing carboxymethylcellulose,<br />
o<strong>the</strong>r polysaccharides, <strong>and</strong> proteins.<br />
They have both dry (elastomers) <strong>and</strong> wet tack (adhesives),<br />
changing physical form by slowly reacting with wound fluid<br />
to form a linked matrix gel. Fibrinolytic activity is due to<br />
pectin <strong>and</strong> antibacterial properties, owing partly to a low<br />
pH. Occlusion is accomplished by a foam or film sheet<br />
backing. Hydrocolloids provide an anaerobic environment<br />
that can sometimes promote hypertropic granulation. They<br />
are best for autolytic debridement <strong>and</strong> mild to moderately<br />
exudating wounds. 58 They are relatively contraindicated with<br />
arterial insufficiency, vasculitis, <strong>and</strong> infection. They have a<br />
long wear time (2 to 7 days), but must be changed if <strong>the</strong><br />
wound fluid leaks through <strong>the</strong> edges. The hydrocolloid<br />
residue may be mistaken for infection <strong>and</strong> should be<br />
cleansed prior to wound bed assessment.<br />
Film dressings are best for <strong>the</strong> late stages of wound healing.<br />
Many are permeable to water vapor <strong>and</strong> oxygen, but<br />
impermeable to water <strong>and</strong> micro-organisms unless leakage<br />
channels develop from <strong>the</strong> periphery. They vary in <strong>the</strong>ir<br />
moisture-vapor permeability properties with Opsite ® (Smith<br />
& Nephew, Largo, Fla) (MVTR <strong>–</strong> 862 gm/m 2 /24 hrs) <strong>and</strong><br />
Tegaderm (3M Pharmaceuticals, London, Ontario, Canada,<br />
<strong>and</strong> Minneapolis, Minn.) (MVTR <strong>–</strong> 846 gm/m 2 /24 hrs) 59<br />
compared to IV 3000 (MVTR 3000, Smith <strong>and</strong> Nephew,<br />
Largo, Fla) designed to keep areas around cannulas dry, but<br />
this dressing would be too dehydrating for most chronic<br />
wounds. Film dressings come in adhesive <strong>and</strong> nonadhesive<br />
forms. They function best for superficial, nonexudative<br />
wounds. 60 They can be left in place for long periods or until<br />
<strong>the</strong>y fall off if <strong>the</strong> seal is intact. Removal by stretching <strong>the</strong><br />
edges will minimize superficial tears.<br />
Friable or bleeding wounds may benefit from <strong>the</strong> tack<br />
provided by fenestrated silicone surfaces (ie, Mepitel,<br />
Mepilex; Molnlycke, Oakville, Ontario, Canada) that can be<br />
left intact while secondary dressings are changed.<br />
32 Ostomy<strong>Wound</strong> Management<br />
Recommendation 12<br />
Evaluate <strong>the</strong> Expected Rate of <strong>Wound</strong> Healing to<br />
Determine if Treatment is Optimal<br />
An orderly sequence of healing should occur if <strong>the</strong> underlying<br />
cause has been treated, optimized local wound care<br />
implemented, <strong>and</strong> patient-centered concerns addressed. It is<br />
essential to have systematic wound documentation. Deep<br />
ulcers with significant depth (those progressing from Stage<br />
IV to Stage II) can be measured with alginate molds that are<br />
weighed <strong>and</strong> <strong>the</strong> weight related to volume or precise determinations.<br />
In most clinical settings, depth can be measured<br />
with a wooden stick in <strong>the</strong> deepest portion of an ulcer or an<br />
average of <strong>the</strong> deepest <strong>and</strong> most superficial portion used for<br />
documentation. Length <strong>and</strong> width are very accurate for<br />
superficial wounds with <strong>the</strong> widest width being measured at<br />
right angles to <strong>the</strong> longest length. 61 For precise determinations,<br />
tracings of superficial ulcers can be analyzed with<br />
computer planimetry. All sinuses <strong>and</strong> areas of undermining<br />
also should be documented. All ulcers will heal after <strong>the</strong><br />
removal of nonviable tissue through maturation of granulation<br />
base <strong>and</strong> filling <strong>the</strong> defect to re-epi<strong>the</strong>lialization.<br />
During <strong>the</strong> early debridement stage, a wound may actually<br />
increase in size before it contracts. Two studies have used<br />
a modified Gillman formula to demonstrate that healing<br />
rates of venous ulcers at 4 weeks can be used to accurately<br />
predict ulcers that will heal by week 12. 62,63 A wound that is<br />
not 30% smaller between weeks 0 <strong>and</strong> 4 is unlikely to heal<br />
by week 12. If an ulcer is not progressing in a measurable<br />
way, <strong>the</strong> treatment of <strong>the</strong> cause, local wound care, <strong>and</strong><br />
patient-related issues must be reassessed. If all <strong>the</strong>se factors<br />
are optimal, biological agents or adjunctive <strong>the</strong>rapies may be<br />
indicated.<br />
Recommendation 13<br />
Use Biological Agents When O<strong>the</strong>r Factors Have<br />
Been Corrected <strong>and</strong> Healing Does not Progress at <strong>the</strong><br />
Expected Rate<br />
Biological agents are expensive, but <strong>the</strong>y stimulate wound<br />
healing. To date, growth factors have been relatively disappointing<br />
because <strong>the</strong>y can be likened to a symphony orchestra,<br />
using only one player, such as <strong>the</strong> flute, without <strong>the</strong> rest<br />
of <strong>the</strong> orchestra. The single player does not allow for an<br />
orderly progression of healing. Despite <strong>the</strong>se limitations,<br />
however, platelet-derived growth factor in a hydrogel<br />
(Regranex ® ; Ortho-McNeil Pharmaceutical, Inc., Raritan,<br />
NJ) has been marketed for use in <strong>the</strong> treatment of diabetic<br />
neurotropic foot ulcers. Platelet-derived growth factor is very
important as a catalyst very early on in wound healing to<br />
promote cellular migration <strong>and</strong> collagen syn<strong>the</strong>sis. It is<br />
applied daily, <strong>and</strong> <strong>the</strong> study showed that with best clinical<br />
practices <strong>and</strong> Regranex ® , healing rate was increased by 15%<br />
in a 20-week trial from 35% in <strong>the</strong> control group to 50%<br />
having complete wound closure in diabetic neurotropic foot<br />
ulcers.<br />
Recent advances in tissue culture techniques (Reinwald<br />
<strong>and</strong> Green) 64 have made it possible to culture cells from<br />
human foreskin donors. Donated newborn foreskins are<br />
used to extract epidermal precursor cells <strong>and</strong> fibroblasts to<br />
master skin banks. Both cells <strong>and</strong> <strong>the</strong> mo<strong>the</strong>rs are extensively<br />
<strong>and</strong> repeatedly screened for possible infectious agents.<br />
From one piece of donated tissue, <strong>the</strong>se cells are transferred<br />
to working cell banks <strong>and</strong> can produce enough skin substitute<br />
to cover four to six football fields. Dermagraft <br />
(Advanced Tissue Sciences/Smith & Nephew Inc., La Jolla,<br />
Calif. <strong>and</strong> Largo, Fla.) is a human fibroblast-derived dermis<br />
consisting of bio-absorbable polygalactin mesh on which<br />
fibroblasts are seeded. The cells proliferate on <strong>the</strong> mesh in<br />
specialized bioreactors to form tissue that is cryopreserved<br />
<strong>and</strong> frozen for long-term storage.<br />
Dermagraft‚ in <strong>the</strong> <strong>the</strong>rapeutic range, increased <strong>the</strong> 12week<br />
healing of DNFU from 32% to 54% over best clinical<br />
practices. This difference in healing rate was maintained<br />
over <strong>the</strong> 32-week trial period demonstrating <strong>the</strong> potential<br />
long-term benefits of advanced <strong>the</strong>rapies. Apligraf ®<br />
(Organogenesis, Canton, Mass. <strong>and</strong> Novartis, East Hanover,<br />
NJ) consists of dermal fibroblasts <strong>and</strong> Type I bovine collagen<br />
matrix with an epidermis <strong>and</strong> differentiating stratum<br />
corneum. In a controlled trial, 63% of venous ulcers healed,<br />
compared with 48% of active control patients by week 24.<br />
A subanalysis of ulcers present for more than 1 year demonstrated<br />
complete healing of 47% of patients treated with<br />
Apligraf ®/ <strong>and</strong> compression compared to 19% treated with<br />
compression <strong>the</strong>rapy alone.<br />
Recently hyaluronic acid in a bipolymer has been made<br />
available for difficult to treat wounds. Hyaluronic acid is a<br />
major carbohydrate component of <strong>the</strong> extracellular matrix,<br />
inducing a prompt angiogenic response, promoting rapid<br />
formation of granulation tissue, assisting fibroblast growth<br />
<strong>and</strong> migration, <strong>and</strong> directing <strong>the</strong> organization of collagen<br />
disposition. 65 This agent has shown promise in case series,<br />
but no controlled trials have been published to date.<br />
Conclusion<br />
The wound care professional has an ever-exp<strong>and</strong>ing tool-<br />
box for ideal wound care. <strong>Debridement</strong>, bacterial balance,<br />
<strong>and</strong> moist interactive healing all must be optimized as integral<br />
parts of preparing <strong>the</strong> wound bed. If <strong>the</strong> underlying<br />
cause, patient-related factors, <strong>and</strong> <strong>the</strong> wound bed have all<br />
been appropriately treated, <strong>the</strong> new <strong>and</strong> exp<strong>and</strong>ing drawer<br />
of biologicals offers increased hope for some of our most difficult<br />
chronic wounds. - OWM<br />
Acknowledgment<br />
Some concepts presented in this paper were first developed<br />
through a series of articles by Diane Krasner <strong>and</strong> R.<br />
Gary Sibbald on wound care in Nursing Clinics of North<br />
America 27 ; Hyperbaric Medicine Practice, 2nd Edition 66 ; <strong>and</strong><br />
The Diabetic Foot, 6th Edition. 67 The local wound care paradigm<br />
(debridement, bacterial balance, <strong>and</strong> moisture balance)<br />
was presented by R. Gary Sibbald as part of a planning session<br />
at The Symposium on Advanced <strong>Wound</strong> Care <strong>and</strong><br />
Medical Research Forum on <strong>Wound</strong> Repair in Dallas, Texas,<br />
April 1<strong>–</strong>4, 2000. Concepts used in <strong>the</strong> charts have been<br />
modified from an educational retreat sponsored by an unrestricted<br />
educational grant from Smith & Nephew Canada<br />
<strong>and</strong> a 1998 Peel regional initiative <strong>and</strong> wound care guide,<br />
compiled by Caremark Ltd.<br />
References<br />
1. Lazarus GS, Cooper DM, Knighton DR, et al. Definitions<br />
<strong>and</strong> guidelines for assessment of wounds <strong>and</strong> evaluation of<br />
healing. Arch Dermatol. 1994;130(4):489<strong>–</strong>493.<br />
2. Winter GD. Formation of <strong>the</strong> scab <strong>and</strong> <strong>the</strong> rate of epi<strong>the</strong>lialization<br />
of superficial wounds in <strong>the</strong> skin of <strong>the</strong> young domestic<br />
pig. Nature. 1962;193:293-294.<br />
3. Winter GD. Epidermal regeneration studied in <strong>the</strong> domestic<br />
pig. In: Mailbesch HI, Rovee DT, eds. Epidermal <strong>Wound</strong><br />
Healing. Chicago, Ill: Year Book Medical Publishers;<br />
1972:71<strong>–</strong>112.<br />
4. Sykes MT, Godsey JB. Vascular evaluation of <strong>the</strong> diabetic<br />
foot. Clin Podiatr Med Surg. 1998;15(a):49<strong>–</strong>83.<br />
5. Moffatt C, O’Hare L. Ankle pulses are not sufficient to detect<br />
impaired circulation in patients with leg ulcers. Journal of<br />
<strong>Wound</strong> Care. 1995;4(3):134<strong>–</strong>138.<br />
6. Moffatt CJ, Dorman MC. Recurrence of leg ulcers within a<br />
community ulcer service. Journal of <strong>Wound</strong> Care.<br />
1995;4(2):57<strong>–</strong>61.<br />
7. Margolis D, Gross E, Wood CR, Lazarus GS. Planimetric<br />
rate of healing in venous ulcers of <strong>the</strong> leg treated with pressure<br />
b<strong>and</strong>age <strong>and</strong> hydrocolloid dressing. JAAD. 1993;28:418<strong>–</strong>421.<br />
8. Young MJ, Cavanagh PR, Thomas G, et al. The effect of callus<br />
removal on dynamic plantar foot pressures in diabetic<br />
patients. Diabet Med. 1992;9(1):55<strong>–</strong>57.<br />
9. Panel for <strong>the</strong> Prediction <strong>and</strong> Prevention of Pressure Ulcers in<br />
Adults. Clinical Practice Guideline Number 3: Pressure Ulcers<br />
in Adults: Prediction <strong>and</strong> Prevention. Rockville, Md: US<br />
Department of Health <strong>and</strong> Human Services. Public Health<br />
Service. Agency for Health Care Policy <strong>and</strong> Research; 1992.<br />
AHCPR Publication 92-0047.<br />
10. Krasner D. Pressure ulcers: assessment, classification <strong>and</strong><br />
November 2000 Vol. 46 Issue 11 33
management. In: Krasner D, Kane D, eds. Chronic <strong>Wound</strong><br />
Care: A Clinical Source Book for Healthcare Professionals, 2nd<br />
ed. Wayne, Pa.: Health Management Publications, Inc.;<br />
1997:152<strong>–</strong>157.<br />
11. Lavery LA, Armstrong DG, Vela SA, Quebedeaux TL,<br />
Fleischli JG. Practical criteria for screening patients at high<br />
risk for diabetic foot ulceration. Arch Intern Med.<br />
1998;158:157<strong>–</strong>162.<br />
12. Armstrong DG, Lavery LA, Harkless L. Validation of diabetic<br />
wound classification. Diabetic Care. 1998;21:855<strong>–</strong>859.<br />
13. Krasner D. Chronic wound pain. In: Krasner D, Kane D,<br />
eds. Chronic <strong>Wound</strong> Care: A Clinical Source Book for<br />
Healthcare Professionals, 2nd ed. Wayne, Pa: Health<br />
Management Publications, Inc.; 1997:336<strong>–</strong>343.<br />
14. Ferris FD, Krasner DL, Sibbald RG. 12 toolkits for Successful<br />
<strong>Wound</strong> Care: A Case-Based Approach. In press.<br />
15. Fletcher A, Cullum N, Sheldon TA. A systematic review of<br />
compression treatment for venous leg ulcers. BMJ<br />
1997;315:576<strong>–</strong>580.<br />
16. Kikta MJ, Schuler JJ, Meyer JP, et al. A prospective, r<strong>and</strong>omized<br />
trial of Unna’s boots versus hydroactive dressing in <strong>the</strong><br />
treatment of venous stasis ulcers. J Vasc Surg.<br />
1988;7:478<strong>–</strong>483.<br />
17. Rubin JR, Alex<strong>and</strong>er J, Plecha EJ, Marman C. Unna’s boot<br />
verus polyurethane foam dressings for <strong>the</strong> treatment of venous<br />
ulceration: a r<strong>and</strong>omized prospective study. Arch Surg.<br />
1990;125:489<strong>–</strong>490.<br />
18. Sikes E. Evaluation of a transparent dressing in <strong>the</strong> treatment<br />
of stasis ulcers of <strong>the</strong> lower limb. Journal of Enterostomal<br />
Therapy. 1985;12:116<strong>–</strong>120.<br />
19. Steed DL, Donohoe D, Webster MW, et al. Effect of extensive<br />
debridement <strong>and</strong> treatment on <strong>the</strong> healing of diabetic<br />
foot ulcers. J Am Coll Surg. 1996;183:61<strong>–</strong>64.<br />
20. Holm J, Andren B, Grofford K. Pain control in <strong>the</strong> surgical<br />
debridement of leg ulcers by <strong>the</strong> use of a topical lidocaineprilocaine<br />
cream, EMLA. Acta Derm Venereol.<br />
1990;70:132<strong>–</strong>136.<br />
21. Lok C, Paul C, Amblard P, et al. EMLA cream as a topical<br />
anes<strong>the</strong>tic for <strong>the</strong> repeated mechanical debridement of venous<br />
leg ulcers: a double-blind, placebo-controlled study. J Am<br />
Acad Dermatol. 1999;40(2.1):208<strong>–</strong>213.<br />
22. Kennedy KL, Tritch DL. <strong>Debridement</strong>. In: Krasner D, Kane<br />
D, eds. Chronic <strong>Wound</strong> Care: A Clinical Source Book for<br />
Healthcare Professionals, 2nd ed. Wayne, Pa: Health<br />
Management Publications, Inc.; 1997:227<strong>–</strong>235.<br />
23. Levenson L. Use of hyperbaric oxygen <strong>and</strong> a sterile hydrogel<br />
in <strong>the</strong> management of a full thickness dorsal foot ulcer. Poster<br />
presentation: Clinical Symposium on <strong>Wound</strong> Care; October<br />
8<strong>–</strong>11, 1996, Atlanta, Ga.<br />
24. Boxer AM, Gottesman N, Bernstein H, M<strong>and</strong>l I.<br />
<strong>Debridement</strong> of dermal ulcers <strong>and</strong> decubiti with collagenase.<br />
Geriatrics. 1969;24:75<strong>–</strong>86.<br />
25. Varma AO, Bugatch E. <strong>Debridement</strong> of dermal ulcers with<br />
collagenase. Surgery, Gynecology <strong>and</strong> Obstetrics.<br />
1973;136:281<strong>–</strong>282.<br />
26. Romanelli M, Piagessi A. Clinical importance of collagenase in<br />
diabetic foot ulcers. Presented at <strong>the</strong> 9th Annual Meeting of<br />
<strong>the</strong> European Tissue Repair Society, Bordeaux, France; 1999.<br />
27. Krasner DL, Sibbald RG. Nursing management of chronic<br />
wounds: best practices across <strong>the</strong> continuum of care. Nurs<br />
Clin North Am. 1999;34(4):933<strong>–</strong>953.<br />
28. Rodeheaver GT. <strong>Wound</strong> cleansing, wound irrigation, wound<br />
disinfection. In: Krasner D, Kane D, eds. Chronic <strong>Wound</strong><br />
Care: A Clinical Source Book for Healthcare Professionals, 2nd<br />
ed. Wayne, Pa: Health Management Publications, Inc.;<br />
1997:97<strong>–</strong>108.<br />
34 Ostomy<strong>Wound</strong> Management<br />
29. De Haan B, Ellis H, Wilkes M. The role of infection in<br />
wound healing. Surgery, Gynecology <strong>and</strong> Obstetrics.<br />
1974;105:283.<br />
30. Pollack S. The wound healing process. Clin Dermatol.<br />
1984;2:8.<br />
31. Altemeier W, Culbertson W. Surgical infection. In: Moyer C,<br />
et al (eds). Surgery, Principals, Practice, 3rd ed. Philadelphia,<br />
Pa: JB Lippincott Co; 1965.<br />
32. Dow G, Browne A, Sibbald RG. Infection in chronic<br />
wounds: controversies in diagnosis <strong>and</strong> treatment.<br />
Ostomy/<strong>Wound</strong> Management. 1999;45(8):23<strong>–</strong>40.<br />
33. Levine NS, Lindberg RB, Mason AD, Pruitt BA. The quantitative<br />
swab culture <strong>and</strong> smear. A quick simple method for<br />
determining <strong>the</strong> number of viable aerobic bacteria on open<br />
wounds. J Trauma. 1976;16:89<strong>–</strong>94.<br />
34. Cutting KF, Harding KGH. Criteria for identifying wound<br />
infection. Journal of <strong>Wound</strong> Care. 1994;3(4):198<strong>–</strong>201.<br />
35. Browne AC, Sibbald RG. <strong>Bacterial</strong> burden assessment of diabetic<br />
neuropathic foot ulcers (DNFU) prior to <strong>the</strong> application<br />
of Dermagraft ® . Presented at: First World <strong>Wound</strong><br />
Healing Congress, September 10<strong>–</strong>13, 2000; Melbourne,<br />
Australia.<br />
36. Krasner D, Cooling M, Hyder T, et al. Sterile versus<br />
Nonsterile <strong>Wound</strong> Care: An Interactive Monograph for<br />
Healthcare Professionals. Toronto, Ontario, Canada: Dumex<br />
Medical Surgical Products Ltd.; 1998.<br />
37. Eltringham I. Mupiricon resistance <strong>and</strong> methicillin-resistant<br />
Staphylococcus aureus (MRSA). J Hosp Infect. 1997;35:1<strong>–</strong>8.<br />
38. Sapico F, Witte J, Canawati H, et al. The infected foot of <strong>the</strong><br />
diabetic patient: quantitative microbiology <strong>and</strong> analysis of<br />
clinical features. 1984 Rev Infect Dis. 1984;6(Suppl 1):S171.<br />
39. Cameron J. The importance of contact dermatitis in <strong>the</strong><br />
management of leg ulcers. Journal of Tissue Viability.<br />
1997;5(2):182<strong>–</strong>185.<br />
40. Sibbald RG, Coutts P, Browne AC, Coehlo S. Acticoat , a<br />
new ionized silver-coating dressings: its effect on bacterial load<br />
<strong>and</strong> healing rates. Poster presented at: First World <strong>Wound</strong><br />
Healing Congress, September 10<strong>–</strong>13, 2000; Melbourne,<br />
Australia.<br />
41. Geronemus RG, Robins P. The effect of two new dressings on<br />
epidermal wound healing. Journal of Dermatological Surgery.<br />
1982;8:850<strong>–</strong>852.<br />
42. Bergstrom N, Bennet MA, Carlson CE, et al. Clinical Practice<br />
Guideline Number 15: Treatment of Pressure Ulcers. Rockville,<br />
Md: US Department of Health <strong>and</strong> Human Services. Public<br />
Health Service. Agency for Health Care Policy <strong>and</strong> Research;<br />
1992. AHCPR Publication 95-0652.<br />
43. Ovington LG. Dressings <strong>and</strong> adjunctive <strong>the</strong>rapies: AHCPR<br />
guidelines revisited. Ostomy/<strong>Wound</strong> Management.<br />
1999;45(suppl 1A):94S<strong>–</strong>106S.<br />
44. Kim YC, Shin JC, Park CI, Oh SH, Choi SM, Kim YS.<br />
Efficacy of hydrocolloid occlusive dressing technique in decubitus<br />
ulcer treatment: a comparative study. Yonsei Med J.<br />
1996;37(3):181<strong>–</strong>185.<br />
45. Xakellis GC, Chrischilles EA. Hydrocolloid versus saline<br />
gauze dressings in treating pressure ulcers: a cost-effective<br />
analysis. Arch Phys Med Rahabil. 1992;73(5):463<strong>–</strong>469.<br />
46. Mulder GD, Altman M, Seeley JE, Tintle T. Prospective r<strong>and</strong>omized<br />
study of <strong>the</strong> efficacy of hydrogel, hydrocolloid, <strong>and</strong><br />
saline solution-moistened dressings on <strong>the</strong> management of<br />
pressure ulcers. <strong>Wound</strong> Repair <strong>and</strong> Regeneration.<br />
1993;1(4):213<strong>–</strong>218.<br />
47. Stotts N. Co-factors in impaired wound healing. In: Krasner<br />
D, Kane D, eds. Chronic <strong>Wound</strong> Care: A Clinical Source Book<br />
for Healthcare Professionals, 2nd ed. Wayne, Pa: Health<br />
Management Publications, Inc.;1997:64<strong>–</strong>72.
48. Day AL, Dombranski S, Farkas C, et al. Managing sacral<br />
pressure ulcers with hydrocolloid dressings: results of a controlled,<br />
clinical study. Ostomy/<strong>Wound</strong> Management.<br />
1995;41(2):52<strong>–</strong>65.<br />
49. Baccari G, Boschetti E. Ferite, ustioni e piaghi medicate con<br />
spugnoa di poliuretano. Communication of <strong>the</strong> Sixth<br />
National Congress of <strong>the</strong> Societa Italiana di Chirurgia<br />
d’Urgenza e Pronto; June 9<strong>–</strong>11, 1977, Padua, Italy.<br />
50. Turner TD. The development of wound management products.<br />
In: Krasner D (ed). Chronic <strong>Wound</strong> Care: A Clinical<br />
Sourcebook for Healthcare Professionals. King of Prussia, Pa.:<br />
Health Management Publications, Inc.; 1990: 31<strong>–</strong>46.<br />
51. Gensheimer D. A review of calcium alginates. Ostomy/<strong>Wound</strong><br />
Management. 1993;39:34<strong>–</strong>38,42<strong>–</strong>43.<br />
52. Gacesa P. Alginates. Carb Polymers. 1988;8:1<strong>–</strong>22.<br />
53. Blair SD, Jarvis P, Salmon M, McCollum C. Clinical trial of<br />
calcium alginate haemostatic swabs. Br J Surg.<br />
1990;77:568<strong>–</strong>570.<br />
54. Barnett SE, Varley SJ. The effects of calcium alginate on<br />
wound healing. Ann R Coll Surg Engl. 1987;69:153<strong>–</strong>155.<br />
55. Peppas NA (ed). Hydrogels in Medicine <strong>and</strong> Pharmacy, vols<br />
1<strong>–</strong>3. Boca Raton, Fla: CRC Press; 1987.<br />
56. Thomas S. <strong>Wound</strong> Management <strong>and</strong> Dressings. London,<br />
Engl<strong>and</strong>: The Pharmaceutical Press; 1990.<br />
57. Falanga V. Occlusive wound dressings: Why, when, what?<br />
Arch Dermatol. 1988;124:872<strong>–</strong>877.<br />
58. Friedman SJ, Su WP. Management of leg ulcers with hydrocolloid<br />
occlusive dressings. Arch Dermatol.<br />
198:120;1329<strong>–</strong>1336.<br />
59. Thomas S (ed). H<strong>and</strong>book of <strong>Wound</strong> Dressings. London,<br />
Engl<strong>and</strong>: Journal of <strong>Wound</strong> Care; 1994.<br />
60. Alper JC. Use of <strong>the</strong> vapour permeable membrane for cutaneous<br />
ulcers: details of application <strong>and</strong> side-effects. J Am Acad<br />
Dermatol. 1984;11:858<strong>–</strong>866.<br />
61. Margolis DJ, Verlin JA, Strom BL. Risk factors associated<br />
with <strong>the</strong> failure of a venous leg ulcer to heal. Arch Dermatol.<br />
1999;135(8):920<strong>–</strong>926.<br />
62. Margolis DJ, Gross EA, Wood CR, Lazarus GS. Planimetric<br />
rate of healing in venous ulcers of <strong>the</strong> leg treated with pressure<br />
b<strong>and</strong>age <strong>and</strong> hydrocolloid dressing. J Am Acad Dermatol.<br />
1993;28(3):418<strong>–</strong>421.<br />
63. Tallman P, Muscare E, Carson P, Eaglestein WH, Falanga V.<br />
Initial rate of healing predicts complete healing of venous<br />
ulcers. Arch Dermatol. 1997;133(1):1231<strong>–</strong>1234.<br />
64. Rheinwald JG, Green H. Serial cultivation of strains of<br />
human epidermal keratinocytes: <strong>the</strong> formation of keratising<br />
colonies from single cells. Cell. 1975;6:331-344.<br />
65. Chen WYJ, Abatangelo G. Functions of hyaluronan in<br />
wound repair. <strong>Wound</strong> Repair <strong>and</strong> Regeneration. 1999;7:79<strong>–</strong>89.<br />
66. Krasner D, Sibbald RG. <strong>Wound</strong> management: best chronic<br />
wound care practices for <strong>the</strong> hyperbaric practitioner. In:<br />
Hyperbaric Medicine Practice, 2nd ed. Flagstaff, Ariz.: Best<br />
Publishing Company; 1999: 395<strong>–</strong>429.<br />
67. Krasner DL, Sibbald RG. Diabetic foot ulcer care: assessment<br />
<strong>and</strong> management. In: Bowker JH, Pfeifer MA (eds). Levin<br />
<strong>and</strong> O’Neill’s The Diabetic Foot, 6th ed. Philadelphia, Pa.:<br />
Mosby/WB Saunders Harcourt Health Services;<br />
2000:283<strong>–</strong>300.