Prescribing Eyeglass Correction for Astigmatism in Infancy and Early ...
Prescribing Eyeglass Correction for Astigmatism in Infancy and Early ...
Prescribing Eyeglass Correction for Astigmatism in Infancy and Early ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
190 Harvey et al<br />
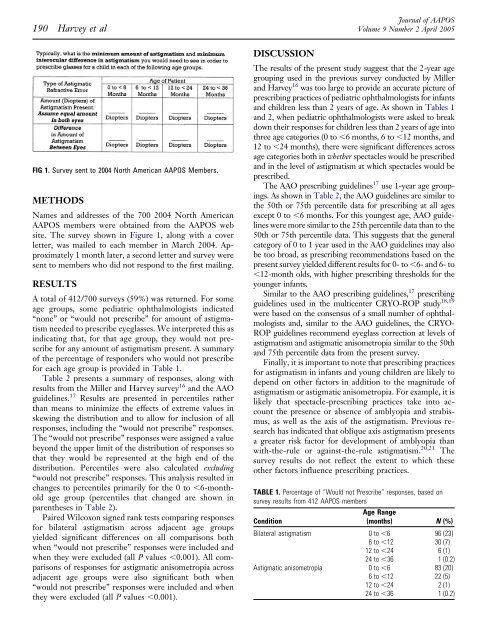
FIG 1. Survey sent to 2004 North American AAPOS Members.<br />
METHODS<br />
Names <strong>and</strong> addresses of the 700 2004 North American<br />
AAPOS members were obta<strong>in</strong>ed from the AAPOS web<br />
site. The survey shown <strong>in</strong> Figure 1, along with a cover<br />
letter, was mailed to each member <strong>in</strong> March 2004. Approximately<br />
1 month later, a second letter <strong>and</strong> survey were<br />
sent to members who did not respond to the first mail<strong>in</strong>g.<br />
RESULTS<br />
A total of 412/700 surveys (59%) was returned. For some<br />
age groups, some pediatric ophthalmologists <strong>in</strong>dicated<br />
“none” or “would not prescribe” <strong>for</strong> amount of astigmatism<br />
needed to prescribe eyeglasses. We <strong>in</strong>terpreted this as<br />
<strong>in</strong>dicat<strong>in</strong>g that, <strong>for</strong> that age group, they would not prescribe<br />
<strong>for</strong> any amount of astigmatism present. A summary<br />
of the percentage of responders who would not prescribe<br />
<strong>for</strong> each age group is provided <strong>in</strong> Table 1.<br />
Table 2 presents a summary of responses, along with<br />
results from the Miller <strong>and</strong> Harvey survey 16 <strong>and</strong> the AAO<br />
guidel<strong>in</strong>es. 17 Results are presented <strong>in</strong> percentiles rather<br />
than means to m<strong>in</strong>imize the effects of extreme values <strong>in</strong><br />
skew<strong>in</strong>g the distribution <strong>and</strong> to allow <strong>for</strong> <strong>in</strong>clusion of all<br />
responses, <strong>in</strong>clud<strong>in</strong>g the “would not prescribe” responses.<br />
The “would not prescribe” responses were assigned a value<br />
beyond the upper limit of the distribution of responses so<br />
that they would be represented at the high end of the<br />
distribution. Percentiles were also calculated exclud<strong>in</strong>g<br />
“would not prescribe” responses. This analysis resulted <strong>in</strong><br />
changes to percentiles primarily <strong>for</strong> the 0 to 6-monthold<br />
age group (percentiles that changed are shown <strong>in</strong><br />
parentheses <strong>in</strong> Table 2).<br />
Paired Wilcoxon signed rank tests compar<strong>in</strong>g responses<br />
<strong>for</strong> bilateral astigmatism across adjacent age groups<br />
yielded significant differences on all comparisons both<br />
when “would not prescribe” responses were <strong>in</strong>cluded <strong>and</strong><br />
when they were excluded (all P values 0.001). All comparisons<br />
of responses <strong>for</strong> astigmatic anisometropia across<br />
adjacent age groups were also significant both when<br />
“would not prescribe” responses were <strong>in</strong>cluded <strong>and</strong> when<br />
they were excluded (all P values 0.001).<br />
DISCUSSION<br />
Journal of AAPOS<br />
Volume 9 Number 2 April 2005<br />
The results of the present study suggest that the 2-year age<br />
group<strong>in</strong>g used <strong>in</strong> the previous survey conducted by Miller<br />
<strong>and</strong> Harvey 16 was too large to provide an accurate picture of<br />
prescrib<strong>in</strong>g practices of pediatric ophthalmologists <strong>for</strong> <strong>in</strong>fants<br />
<strong>and</strong> children less than 2 years of age. As shown <strong>in</strong> Tables 1<br />
<strong>and</strong> 2, when pediatric ophthalmologists were asked to break<br />
down their responses <strong>for</strong> children less than 2 years of age <strong>in</strong>to<br />
three age categories (0 to 6 months, 6 to 12 months, <strong>and</strong><br />
12 to 24 months), there were significant differences across<br />
age categories both <strong>in</strong> whether spectacles would be prescribed<br />
<strong>and</strong> <strong>in</strong> the level of astigmatism at which spectacles would be<br />
prescribed.<br />
The AAO prescrib<strong>in</strong>g guidel<strong>in</strong>es 17 use 1-year age group<strong>in</strong>gs.<br />
As shown <strong>in</strong> Table 2, the AAO guidel<strong>in</strong>es are similar to<br />
the 50th or 75th percentile data <strong>for</strong> prescrib<strong>in</strong>g at all ages<br />
except 0 to 6 months. For this youngest age, AAO guidel<strong>in</strong>es<br />
were more similar to the 25th percentile data than to the<br />
50th or 75th percentile data. This suggests that the general<br />
category of 0 to 1 year used <strong>in</strong> the AAO guidel<strong>in</strong>es may also<br />
be too broad, as prescrib<strong>in</strong>g recommendations based on the<br />
present survey yielded different results <strong>for</strong> 0- to 6- <strong>and</strong> 6- to<br />
12-month olds, with higher prescrib<strong>in</strong>g thresholds <strong>for</strong> the<br />
younger <strong>in</strong>fants.<br />
Similar to the AAO prescrib<strong>in</strong>g guidel<strong>in</strong>es, 17 prescrib<strong>in</strong>g<br />
guidel<strong>in</strong>es used <strong>in</strong> the multicenter CRYO-ROP study 18,19<br />
were based on the consensus of a small number of ophthalmologists<br />
<strong>and</strong>, similar to the AAO guidel<strong>in</strong>es, the CRYO-<br />
ROP guidel<strong>in</strong>es recommend eyeglass correction at levels of<br />
astigmatism <strong>and</strong> astigmatic anisometropia similar to the 50th<br />
<strong>and</strong> 75th percentile data from the present survey.<br />
F<strong>in</strong>ally, it is important to note that prescrib<strong>in</strong>g practices<br />
<strong>for</strong> astigmatism <strong>in</strong> <strong>in</strong>fants <strong>and</strong> young children are likely to<br />
depend on other factors <strong>in</strong> addition to the magnitude of<br />
astigmatism or astigmatic anisometropia. For example, it is<br />
likely that spectacle-prescrib<strong>in</strong>g practices take <strong>in</strong>to account<br />
the presence or absence of amblyopia <strong>and</strong> strabismus,<br />
as well as the axis of the astigmatism. Previous research<br />
has <strong>in</strong>dicated that oblique axis astigmatism presents<br />
a greater risk factor <strong>for</strong> development of amblyopia than<br />
with-the-rule or aga<strong>in</strong>st-the-rule astigmatism. 20,21 The<br />
survey results do not reflect the extent to which these<br />
other factors <strong>in</strong>fluence prescrib<strong>in</strong>g practices.<br />
TABLE 1. Percentage of “Would not Prescribe” responses, based on<br />
survey results from 412 AAPOS members<br />
Condition<br />
Age Range<br />
(months) N (%)<br />
Bilateral astigmatism 0 to 6 96 (23)<br />
6to12 30 (7)<br />
12 to 24 6 (1)<br />
24 to 36 1 (0.2)<br />
Astigmatic anisometropia 0 to 6 83 (20)<br />
6to12 22 (5)<br />
12 to 24 2 (1)<br />
24 to 36 1 (0.2)