REQUEST FOR LEAVE FORM – AFSCME MEMBERS ONLY
REQUEST FOR LEAVE FORM – AFSCME MEMBERS ONLY
REQUEST FOR LEAVE FORM – AFSCME MEMBERS ONLY

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>REQUEST</strong> <strong>FOR</strong> <strong>LEAVE</strong> <strong>FOR</strong>M <strong>–</strong> <strong>AFSCME</strong> <strong>MEMBERS</strong> <strong>ONLY</strong><br />
Option 1: (Scan it)<br />
Step one: (Employee) completes the form and signs it in pen;<br />
Step two: (Manager) signs the form in pen, scans it and sends it electronically to the<br />
attention of <strong>AFSCME</strong>-RFL@facilities.udel.edu. (HR Liaison/Timekeeper team);<br />
Step Three: (Manager) provides a copy of the signed (approved) form to the employee.<br />
Option 2: (Manual)<br />
Step one: (Employee) completes the form and signs it in pen;<br />
Step two: (Manager) signs the form in pen, makes a copy of the signed (approved)<br />
form;<br />
Step Three: (Manager) provides a copy of the signed (approved) form to the employee.<br />
Step four: (Manager) sends the original form to the attention of Sheila Boyle or Kathy<br />
Michael (to whoever is the designated HR Liaison/Timekeeper) via an inter-office<br />
envelope or hand delivers the original document;<br />
Step five: (Sheila or Kathy) scans the form and sends the original form back to the<br />
designated manager for his/her records.<br />
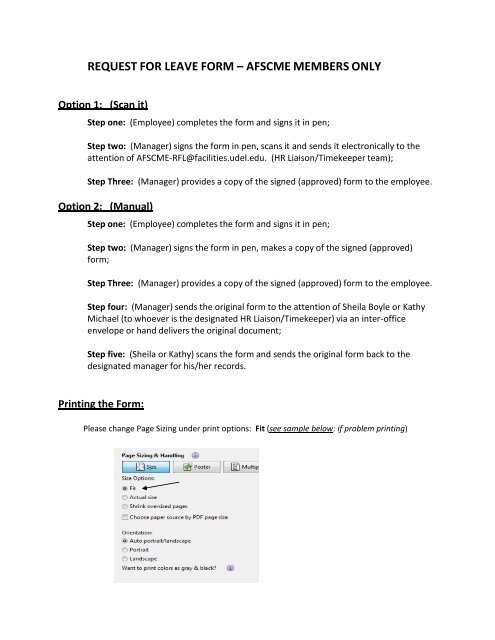
Printing the Form:<br />
Please change Page Sizing under print options: Fit (see sample below: if problem printing)
NAME EMPL ID#<br />
DEPARTMENT<br />
REASON <strong>FOR</strong> ABSENCE: Sick No Pay Bereavement<br />
Vacation<br />
Emergency Vac<br />
Comp Time Off<br />
Sick Pay<br />
LTI<br />
Accident Paid<br />
Accident Not Paid<br />
Ex Absence<br />
Jury Duty<br />
Late No Pay<br />
DEP CARE<br />
FMLA<br />
BEGINNING DATE BEGINNING TIME<br />
AM PM<br />
ENDING DATE ENDING TIME<br />
REASON <strong>FOR</strong> ABSENCE: Sick No Pay<br />
AM PM<br />
Bereavement<br />
Vacation<br />
LTI<br />
Jury Duty<br />
Emergency Vac<br />
Accident Paid<br />
Late No Pay<br />
Comp Time Off<br />
Accident Not Paid<br />
DEP CARE<br />
Sick Pay<br />
Ex Absence<br />
FMLA<br />
BEGINNING DATE BEGINNING TIME<br />
AM PM<br />
ENDING DATE ENDING TIME<br />
COMMENTS<br />
AM PM<br />
PRINT EMPLOYEE NAME & SIGN DATE<br />
SUPERVISOR/MANAGER'S SIGNATURE DATE<br />
Revised 05/2012<br />
HOURS<br />
DAYS<br />
HOURS<br />
DAYS<br />
FMLA NO PAY<br />
FMLA Vac<br />
Other<br />
FMLA NO PAY<br />
FMLA Vac<br />
Other