the anorexic tortoise - BSAVA
the anorexic tortoise - BSAVA
the anorexic tortoise - BSAVA

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
How to approach<br />
<strong>the</strong> <strong>anorexic</strong><br />
<strong>tortoise</strong><br />
John Chitty, who runs<br />
<strong>the</strong> exotics service at<br />
Anton Vets, helps us<br />
tackle a challenging<br />
topic<br />
Anorexia is probably <strong>the</strong> most<br />
common presenting sign for<br />
<strong>tortoise</strong>s seen in veterinary<br />
practice. In some cases patients<br />
are overtly unwell; in o<strong>the</strong>rs <strong>the</strong> animal<br />
still seems bright; and some will be in<br />
between, appearing ‘just a little slow’<br />
to <strong>the</strong>ir owners.<br />
In an article such as this it is important<br />
to define some of <strong>the</strong> terms used:<br />
■■ Tortoise. For <strong>the</strong> purposes of this<br />
article a <strong>tortoise</strong> is one of <strong>the</strong> Testudo<br />
group of Mediterranean/Middle<br />
Eastern <strong>tortoise</strong>s – <strong>the</strong> Spur-thighed<br />
group; Hermann’s: marginated; and<br />
Horsfield’s <strong>tortoise</strong>s: <strong>the</strong>se are <strong>the</strong><br />
<strong>tortoise</strong>s most commonly kept as pets<br />
in <strong>the</strong> UK. With <strong>the</strong> exception of some<br />
North African spur-thighed <strong>tortoise</strong>s,<br />
<strong>the</strong> majority will hibernate. All are<br />
herbivorous and terrestrial.<br />
■■ Anorexia. Literally means lack of, or<br />
reduced appetite. However, reptiles do<br />
not always eat every day, especially<br />
when breeding or immediately before/<br />
after hibernation. Therefore it is<br />
important to determine whe<strong>the</strong>r <strong>the</strong><br />
anorexia is persistent and significant or<br />
a single occurrence. It is necessary to<br />
investigate fur<strong>the</strong>r if:<br />
– ■ There is concurrent weight loss.<br />
– ■ There are any o<strong>the</strong>r signs of ill<br />
health, including lethargy.<br />
– ■ The <strong>tortoise</strong> has not eaten for over a<br />
12 | companion<br />
week. If less than a week and <strong>the</strong><br />
<strong>tortoise</strong> appears well, advise<br />
owners to keep <strong>the</strong> <strong>tortoise</strong> warm<br />
(25–35°C in <strong>the</strong> day: 20–25°C at<br />
night), ba<strong>the</strong> it daily in plain warm<br />
water for 10–15 minutes and<br />
monitor bodyweight daily.<br />
Post-hibernation anorexia is not a<br />
specific condition. Anorexia is common<br />
during this period mainly because this is a<br />
time of maximal metabolic stress in <strong>the</strong><br />
animal and because UK wea<strong>the</strong>r can be<br />
particularly variable in Spring (for this<br />
reason, it is also common to see <strong>anorexic</strong><br />
animals in Autumn too). In any event, <strong>the</strong><br />
diagnostic investigation of <strong>the</strong> <strong>anorexic</strong><br />
<strong>tortoise</strong> is largely <strong>the</strong> same whatever <strong>the</strong><br />
time of year.<br />
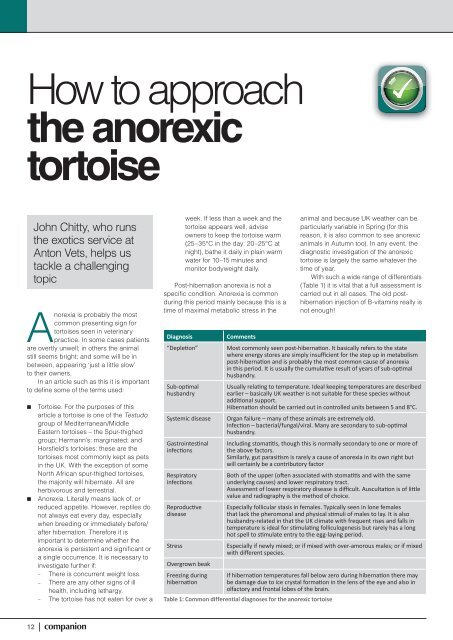
With such a wide range of differentials<br />
(Table 1) it is vital that a full assessment is<br />
carried out in all cases. The old posthibernation<br />
injection of B-vitamins really is<br />
not enough!<br />
Diagnosis Comments<br />
“Depleti on” Most commonly seen post-hibernati on. It basically refers to <strong>the</strong> state<br />
where energy stores are simply insuffi cient for <strong>the</strong> step up in metabolism<br />
post-hibernati on and is probably <strong>the</strong> most common cause of anorexia<br />
in this period. It is usually <strong>the</strong> cumulati ve result of years of sub-opti mal<br />
husbandry.<br />
Sub-opti mal<br />
husbandry<br />
Usually relati ng to temperature. Ideal keeping temperatures are described<br />
earlier – basically UK wea<strong>the</strong>r is not suitable for <strong>the</strong>se species without<br />
additi onal support.<br />
Hibernati on should be carried out in controlled units between 5 and 8°C.<br />
Systemic disease Organ failure – many of <strong>the</strong>se animals are extremely old.<br />
Infecti on – bacterial/fungal/viral. Many are secondary to sub-opti mal<br />
husbandry.<br />
Gastrointesti nal<br />
infecti ons<br />
Respiratory<br />
infecti ons<br />
Reproducti ve<br />
disease<br />
Including stomati ti s, though this is normally secondary to one or more of<br />
<strong>the</strong> above factors.<br />
Similarly, gut parasiti sm is rarely a cause of anorexia in its own right but<br />
will certainly be a contributory factor<br />
Both of <strong>the</strong> upper (oft en associated with stomati ti s and with <strong>the</strong> same<br />
underlying causes) and lower respiratory tract.<br />
Assessment of lower respiratory disease is diffi cult. Auscultati on is of litt le<br />
value and radiography is <strong>the</strong> method of choice.<br />
Especially follicular stasis in females. Typically seen in lone females<br />
that lack <strong>the</strong> pheromonal and physical sti muli of males to lay. It is also<br />
husbandry-related in that <strong>the</strong> UK climate with frequent rises and falls in<br />
temperature is ideal for sti mulati ng folliculogenesis but rarely has a long<br />
hot spell to sti mulate entry to <strong>the</strong> egg-laying period.<br />
Stress Especially if newly mixed; or if mixed with over-amorous males; or if mixed<br />
with diff erent species.<br />
Overgrown beak<br />
Freezing during If hibernati on temperatures fall below zero during hibernati on <strong>the</strong>re may<br />
hibernati on<br />
be damage due to ice crystal formati on in <strong>the</strong> lens of <strong>the</strong> eye and also in<br />
olfactory and frontal lobes of <strong>the</strong> brain.<br />
Table 1: Common differential diagnoses for <strong>the</strong> <strong>anorexic</strong> <strong>tortoise</strong>
Figure 1: A male Hermann’s <strong>tortoise</strong> – note <strong>the</strong><br />
long keratinised end to <strong>the</strong> tail<br />
Clinical assessment<br />
A full history should be taken. This should<br />
concentrate on:<br />
■■ Signalment – unlike in dogs and cats<br />
this is rarely known. Most owners can<br />
say how long <strong>the</strong>y have had <strong>the</strong> animal<br />
but can rarely give more than an<br />
indication of age. If owned for many<br />
years it is worth asking if <strong>the</strong> <strong>tortoise</strong><br />
has grown in that time. If it has grown<br />
significantly <strong>the</strong>n likely it was young<br />
when first owned. If not, <strong>the</strong>n it was<br />
probably mature when first owned. With<br />
<strong>the</strong>se species physical maturity would<br />
probably suggest that <strong>the</strong> <strong>tortoise</strong> was<br />
at least 20 years old when acquired.<br />
The species of <strong>tortoise</strong> is also not<br />
always known and it is worth being<br />
familiar with <strong>the</strong> common species in<br />
this group. Sex is often determined by<br />
whe<strong>the</strong>r or not <strong>the</strong> <strong>tortoise</strong> has laid<br />
eggs or not. This is not always reliable!<br />
While Hermann’s and Horsfield’s are<br />
relatively easy to sex (males have much<br />
longer tails – Figure 1) <strong>the</strong> spur-thighed<br />
group can be very hard to sex. Shell<br />
shapes can be useful but are unreliable<br />
in captive-bred animals as <strong>the</strong>re are so<br />
many diet-induced abnormalities.<br />
Familiarity is <strong>the</strong> key!<br />
■■ Husbandry. Full details are required:<br />
– ■ Hibernation times and manner.<br />
– ■ Temperature provision if any;<br />
temperature measurements and<br />
how <strong>the</strong>se are are performed –<br />
remember that a <strong>the</strong>rmostat is a<br />
control device not an accurate<br />
measure of temperature.<br />
– ■ If housed, vivarium or tray? Is <strong>the</strong><br />
<strong>tortoise</strong> kept outside?<br />
– ■ Humidity (Mediterranean <strong>tortoise</strong>s<br />
generally require a dry environment).<br />
– ■ Diet and feeding history.<br />
– ■ Bathing?<br />
– ■ Weight history. Many owners keep<br />
accurate records of <strong>the</strong> animal’s<br />
weight, especially before and after<br />
hibernation. These data are very<br />
valuable.<br />
– ■ Contact with o<strong>the</strong>r animals,<br />
especially o<strong>the</strong>r <strong>tortoise</strong> species.<br />
■■ Medical history.<br />
■■ Urination/defecation: absence of<br />
<strong>the</strong>se (especially if being ba<strong>the</strong>d) is<br />
significant.<br />
■■ Reaction to food – is <strong>the</strong> <strong>tortoise</strong><br />
interested?<br />
■■ Activity levels.<br />
■■ Respiratory noise.<br />
Before handling, <strong>the</strong> respiratory pattern<br />
should be assessed. In most <strong>tortoise</strong>s<br />
breaths are infrequent and may be hard to<br />
detect. However, if <strong>the</strong>re is overt respiratory<br />
effort, open-mouth breathing, or excessive<br />
vocalisation on breathing <strong>the</strong>n <strong>the</strong>se may<br />
be indicators of severe disease. Do not<br />
confuse aggressive hissing with respiratory<br />
noise, nor gular pumping (throat<br />
movements) with respiratory movements.<br />
A thorough clinical examination should<br />
be performed. However, <strong>the</strong> presence of<br />
<strong>the</strong> shell severely limits what can be<br />
examined. All patients should be weighed<br />
and this weight compared to any previously<br />
recorded weights and, most importantly,<br />
with <strong>the</strong> animal’s current body condition.<br />
Body condition is assessed by <strong>the</strong><br />
amount of fat pad present in <strong>the</strong> prefemoral<br />
fossa and between forelimbs and<br />
neck. Sunken eyes may be a sign of<br />
dehydration, but may also indicate a loss of<br />
<strong>the</strong> fat pad behind <strong>the</strong> eyes.<br />
The Jackson ratio (a graphical<br />
comparison of weight:length allowing<br />
assessment of ideal condition) may be of<br />
some use for medium-sized spur-thighed<br />
and Hermann’s <strong>tortoise</strong>s, but generally is of<br />
limited value compared to body condition<br />
assessment – for example a <strong>tortoise</strong><br />
containing many eggs will have a good<br />
Jackson “score” even though it may be<br />
very thin.<br />
The eyes should be assessed for<br />
opacities and swelling of lids,<br />
conjunctiva, etc.<br />
The nares should be checked for<br />
discharges, abscessation, etc.<br />
The mouth should be carefully<br />
assessed (Figure 2) for:<br />
Figure 2: Oral examination – note normal<br />
membrane colour and texture<br />
companion | 13
14 | companion<br />
How to approach <strong>the</strong> <strong>anorexic</strong> <strong>tortoise</strong><br />
■■ Mucous membrane colour. Some<br />
yellowing may be normal in <strong>the</strong><br />
post-hibernation period. Cyanosis<br />
potentially indicates respiratory disease.<br />
■■ Dry sticky membranes – may show<br />
severe dehydration.<br />
■■ Presence of purulent or diph<strong>the</strong>ritic<br />
material.<br />
■■ Foreign bodies within <strong>the</strong> choana<br />
(passage in roof of mouth to nasal<br />
chamber).<br />
Limbs should be checked for swellings<br />
and it is useful to see <strong>the</strong> <strong>tortoise</strong> walk,<br />
though this is not always possible.<br />
The cloaca should be examined as<br />
much as possible, in particular for<br />
discharges and ulceration.<br />
The shell should be assessed for<br />
damage or infection. In septicaemia<br />
<strong>the</strong>re may be a reddening of parts of <strong>the</strong><br />
shell. This will “blanch” when pressed with<br />
a fingernail.<br />
The skin may be checked for<br />
ulceration, flakiness or o<strong>the</strong>r lesions.<br />
Tenting of <strong>the</strong> skin is not a reliable indicator<br />
of dehydration.<br />
Limited palpation of <strong>the</strong> abdomen<br />
may be performed by placing fingers in<br />
<strong>the</strong> prefemoral fossae and gently<br />
rocking <strong>the</strong> <strong>tortoise</strong> side-to-side.<br />
Large masses or eggs may bump<br />
against <strong>the</strong> fingers.<br />
The heart may be auscultated using<br />
a 8MHz Doppler device (as used for<br />
measuring feline blood pressure) placed<br />
on <strong>the</strong> skin between forelimb and neck.<br />
Harsh murmurs may be an indication<br />
of endocarditis.<br />
Sample taking<br />
Clinical findings will dictate which<br />
samples are taken. However, a blood<br />
sample is essential in nearly all cases in<br />
order to assess underlying disease, fluid<br />
and electrolyte balance, nutritional status<br />
and immune status and inflammatory<br />
status. Without sampling it is nearly<br />
impossible to assess hydration and<br />
feeding needs adequately.<br />
Table 2 details <strong>the</strong> parameters<br />
evaluated in blood analysis of <strong>the</strong>se<br />
patients. Some tests are performed patientside,<br />
o<strong>the</strong>rs by a diagnostic laboratory.<br />
Most laboratories will be able to assess<br />
<strong>the</strong>se on approx 1 ml heparinised blood<br />
(haematology is performed on blood taken<br />
into heparin not EDTA) and two fresh blood<br />
smears, however <strong>the</strong>y should be consulted<br />
prior to sampling to check <strong>the</strong>ir needs and<br />
also which parameters <strong>the</strong>y include in <strong>the</strong>ir<br />
profiles. Blood samples may be taken from<br />
jugular, subcarapacial (Figure 3) or tail<br />
veins. It is always worth stating on<br />
submission forms which sampling site has<br />
been used, as <strong>the</strong>re is a much higher<br />
incidence of lymphodilution from <strong>the</strong> tail<br />
vein. Where obvious lymphodilution<br />
occurs, <strong>the</strong> sample should be discarded.<br />
Interpretation of blood parameters<br />
(Table 2) can be very difficult. Not only do<br />
individual labs and machines vary in <strong>the</strong>ir<br />
reference intervals, but <strong>the</strong>re may be<br />
differences between species and certainly<br />
Figure 3: Sampling from subcarapacial vein – a<br />
bent needle is inserted in <strong>the</strong> dorsal midline<br />
approximately where skin joins shell<br />
major differences in individual parameters<br />
through <strong>the</strong> annual cycle. It is very<br />
important to use laboratories with<br />
experienced consultants to assist in such<br />
interpretation – to this end a thorough<br />
written history and as accurate a<br />
signalment as possible should accompany<br />
each case submission.<br />
Parameter Notes<br />
Haematology Full haematology – red and white cell parameters. Oft en <strong>the</strong> cell counts are<br />
of lesser importance than cell morphology which is why an experienced<br />
“exoti cs” haematologist should always be consulted.<br />
Urea See Table 3.<br />
Uric acid See Table 3. Also a useful assessment of renal disease. Levels >1000 µmol/l<br />
indicati ve of renal disease: >2500 µmol/l grave prognosis.<br />
Electrolytes Sodium, potassium, ionised calcium. Potassium levels >5 mmol/l are<br />
signifi cant; >9 mmol/l grave prognosis. These should be measured<br />
pati entside or a spun heparin gel tube should also be supplied. O<strong>the</strong>rwise<br />
post-sampling changes may arti fi cially raise potassium levels.<br />
Total calcium and Not as useful in assessment of renal disease as in iguanas, but of use in<br />
phosphate assessing reproducti ve functi on in females (Box 1).<br />
Glucose Measure pati entside – immediate assessment of nutriti onal status/depleti on.<br />
Beta-<br />
Ketosis.<br />
Hydroxybutyrate<br />
Liver enzymes AST, CK, GLDH and GGT may all be assessed. These allow some assessment<br />
of hepatocellular damage and ti ssue damage. However, none is sensiti ve nor<br />
specifi c and it is hard to assess liver disease in chelonians. Biliverdinuria is a<br />
more specifi c indicator, though not sensiti ve.<br />
Bile acids Can be hard to assess unless extremely high.<br />
Proteins Albumin, globulins and rati o. Assessment of protein balance and<br />
infl ammatory responses. Electrophoresis may be helpful in <strong>the</strong> latt er case.<br />
Table 2: Parameters to be included in an <strong>anorexic</strong> <strong>tortoise</strong> blood panel
Parameter Comments<br />
Skin tenting Hard to assess and a very insensitive measure.<br />
Mucous membranes Dry sticky membranes more sensitive than skin tenting.<br />
Haemoconcentration In <strong>the</strong>ory, raised albumin and haematocrit should accompany<br />
dehydration. However, most of <strong>the</strong>se <strong>tortoise</strong>s will have varying degrees<br />
of hypoalbuminaemia and anaemia (due to underlying disease/debility/<br />
anorexia) that such an interpretation is confounded.<br />
Uric acid Will rise in dehydration. However, will also rise in renal disease.<br />
Urea These species use <strong>the</strong> urinary bladder as a water store. Accessing this<br />
allows smaller molecules, including urea, to enter <strong>the</strong> bloodstream – i.e.<br />
urea is a measure of degree of access to stores. The higher <strong>the</strong> level of<br />
urea, <strong>the</strong> greater <strong>the</strong> dehydration. It is unaffected by renal disease (except<br />
in severe disease) so is an extremely important indicator of hydration.<br />
Table 3: Assessment of dehydration in <strong>the</strong> <strong>tortoise</strong><br />
BOX 1: Markers of reproductive function in female <strong>tortoise</strong>s<br />
The following parameters may all rise in <strong>the</strong> reproductively active female:<br />
■■ Protein – total/albumin/globulin<br />
■■ Total calcium<br />
■■ Phosphate – Calcium:phosphate ratio usually remains in normal range<br />
■■ AST/ALKP/CK<br />
■■ Cholesterol/triglyceride<br />
NB: This “pattern” is not a marker for reproductive disease or follicular stasis unless such<br />
levels remain high and <strong>the</strong> <strong>tortoise</strong> is not recovering. Ra<strong>the</strong>r, it indicates a need to assess <strong>the</strong><br />
reproductive system via radiography/ultrasonography.<br />
Follicular stasis is diagnosed by a persistent:<br />
■■ Reproductive blood picture<br />
■■ Ovarian follicles – <strong>the</strong>se show no evidence of atresia nor progression to egg<br />
Test Comments Indication<br />
Faecal analysis May be hard to obtain! Worth<br />
bathing daily to twice daily to<br />
stimulate defecation. Fresh (
Apart from <strong>the</strong> very mildest cases, it is<br />
highly unlikely this can be provided at<br />
home, so almost all cases will require<br />
hospitalisation. As husbandry problems<br />
started at home, out-patient <strong>the</strong>rapy is<br />
unlikely to be successful.<br />
Hospitalisation is usually 5–14 days for<br />
<strong>the</strong> average case. Therefore a practice<br />
treating <strong>the</strong>se species will need specific<br />
facilities. This may vary from a heat lamp in<br />
a kennel for <strong>the</strong> occasional case, to vivaria<br />
or <strong>tortoise</strong> trays where <strong>the</strong>re is a greater<br />
caseload (Figure 5).<br />
Again, important biological parameters,<br />
especially temperature should be<br />
measured and maintained at correct levels<br />
in hospital (Figure 6). Half measures will<br />
not suffice and result in more unsuccessful<br />
cases and frustrated owners.<br />
It is vital that owner education is a part<br />
of <strong>the</strong> treatment plan. This is especially<br />
important for older <strong>tortoise</strong>s as owners do<br />
not see why <strong>the</strong>re is a problem now with<br />
<strong>the</strong>ir husbandry when <strong>the</strong>re had been no<br />
issues over <strong>the</strong> previous thirty-odd years!<br />
However, reluctance to change husbandry<br />
will simply result in relapsing cases. A<br />
frequent finding with inadequate home<br />
temperatures is that <strong>the</strong> <strong>tortoise</strong> will do well<br />
for 48 hours following discharge and <strong>the</strong>n<br />
stop eating: some research suggests<br />
reptiles can maintain internal temperatures<br />
for up to 2 days!<br />
16 | companion<br />
How to approach <strong>the</strong> <strong>anorexic</strong> <strong>tortoise</strong><br />
A B Figure 7: Daily bathing is vital. It also helps<br />
Figure 5: Hospitalisation units. Vivaria are a typical means of housing all reptiles. They have,<br />
erroneously, gained a reputation as a cause of respiratory disease in <strong>tortoise</strong>s due to high humidity.<br />
However, this can be controlled as well as temperature. Trays are excellent means of hospitalising<br />
<strong>tortoise</strong>s but rely on a high background room temperature as it is this that sets crucial minimum<br />
temperatures. The author’s unit uses combined ultra-violet and heat sources as basking points<br />
Figure 6: Digital maximum–minimum<br />
<strong>the</strong>rmometers are easily available and <strong>the</strong>se<br />
units with two probes are inexpensive. This<br />
photo shows minimum values that should be<br />
achieved in <strong>the</strong> hospitalised setting. If using<br />
vivaria, <strong>the</strong>y should be insulated to achieve<br />
<strong>the</strong>se temperatures. If using trays, room<br />
temperature needs controlling to <strong>the</strong>se levels<br />
While hospitalised, all cases will require<br />
basic supportive care.<br />
Rehydration<br />
All <strong>tortoise</strong>s should be ba<strong>the</strong>d daily in plain<br />
warm water or in a glucose/electrolyte mix<br />
(e.g. Reptoboost (Vetark, Winchester UK)).<br />
For mildly dehydrated animals this may be<br />
sufficient to restore fluid balance. Bathing<br />
will also help to stimulate urination/<br />
defecation (Figure 7).<br />
stimulate defecation/urination (see <strong>tortoise</strong> on<br />
left). Biosecurity is vital – all equipment should<br />
be labelled (in this case bath numbers match<br />
tray numbers) so no fomite transfer occurs<br />
between in-patients<br />
For more severe cases, fluids may be<br />
given:<br />
■■ Oral fluids – Hypotonic fluids (including<br />
plain water!) may be given by gavage<br />
tube. Around 20ml/kg in single or<br />
divided doses (Figure 8).<br />
■■ Intra- or epi-coelomic (Figure 9) – Up to<br />
30 ml/kg once daily of isotonic fluid.<br />
■■ Intra-osseous – Needles may be<br />
placed into <strong>the</strong> femur or humerus, or<br />
Figure 8: Gavage tubing a <strong>tortoise</strong>. The neck is<br />
held straight and <strong>the</strong> tube gently inserted down<br />
<strong>the</strong> oesophagus
Figure 9: Epi-coelomic fluid injection into <strong>the</strong><br />
prefemoral fossa<br />
<strong>the</strong> bridge of <strong>the</strong> shell between <strong>the</strong><br />
plastron and carapace. Isotonic fluids<br />
are given at approx 30 ml/kg/day and a<br />
syringe driver or Springfusor pump is<br />
required for administration.<br />
Fluid choice for systemic <strong>the</strong>rapy<br />
depends on electrolyte assessment.<br />
Critical nutrition<br />
It is important to stimulate eating as<br />
quickly as possible. To this end, <strong>the</strong><br />
<strong>tortoise</strong>’s favourite foods should be<br />
ascertained and offered.<br />
Where <strong>the</strong>re is no particular favourite,<br />
this author offers a standard salad mix<br />
(lettuce/cucumber/tomato) with<br />
strawberries and dandelions whenever<br />
available. This is not a balanced diet and<br />
vitamin supplementation is not offered as<br />
many <strong>tortoise</strong>s do not like <strong>the</strong>se. Once <strong>the</strong><br />
<strong>tortoise</strong> is eating well, <strong>the</strong> diet can be<br />
amended to a more healthy one.<br />
Those cases that are suspected of<br />
being blind and/or cold-damaged should<br />
be hand-fed especially if <strong>the</strong>y actively<br />
appear interested in food.<br />
O<strong>the</strong>rwise critical nutrition is provided<br />
by gavage tube. Initially, simple<br />
carbohydrate mixes (e.g. Critical Care<br />
Formula (Vetark, Winchester, UK) or Liquid<br />
Lifeade (Norbrook, Carlisle, UK))<br />
progressing to higher fibre formulas in<br />
herbivores (e.g. Oxbow Fine Grind (Oxbow,<br />
Nebraska, USA), Emeraid Herbivore<br />
(Lafeber, USA)). Formulas for carnivores<br />
should be avoided.<br />
Animals that are difficult to tube, will<br />
require long-term tubing or have sufficiently<br />
good husbandry to be treated at home can<br />
be fed by means of an oesophagostomy<br />
tube. This should be fitted under sedation<br />
or local anaes<strong>the</strong>sia (depending on level of<br />
debility) in much <strong>the</strong> same way as in a cat.<br />
Antibiotic <strong>the</strong>rapy<br />
Broad-spectrum “cover” is required in all<br />
<strong>tortoise</strong>s with extremely low white cell<br />
counts or those showing an active<br />
inflammatory response. Where <strong>the</strong>re are<br />
identifiable lesions (e.g. stomatitis,<br />
pneumonia), drug choice should be<br />
based on culture and sensitivity of<br />
collected samples.<br />
Where <strong>the</strong>re are no obvious lesions,<br />
fluoroquinolones or ceftazidime may be<br />
used empirically. Care should be taken not<br />
to select very irritant drugs for long-term<br />
intramuscular administration. If long-term<br />
use is needed, <strong>the</strong>n ei<strong>the</strong>r a less irritant<br />
drug should be used or <strong>the</strong> medication<br />
switched to oral dosing as soon as <strong>the</strong><br />
clinician is sure gut absorption is optimal.<br />
Monitoring<br />
Where <strong>the</strong> <strong>tortoise</strong> is clearly improving<br />
clinically (appears stronger, eating,<br />
urinating/defecating, etc.) and continues to<br />
do well at home, <strong>the</strong>re is rarely a need to<br />
do more than physical checks.<br />
However, for animals that ei<strong>the</strong>r showed<br />
severe abnormalities on initial blood<br />
sampling or that are showing little or no<br />
response to <strong>the</strong>rapy, repeat blood sampling<br />
at 7–10-day intervals is a very good means<br />
of assessing progress and prognosis.<br />
Prevention<br />
It is clear that <strong>the</strong> key to avoiding anorexia<br />
is maintenance of good husbandry.<br />
Traditional means of keeping <strong>tortoise</strong>s in<br />
<strong>the</strong> UK, combined with <strong>the</strong> older methods<br />
of hibernation (such as a box of hay in<br />
garage/shed/loft), are simply not adequate<br />
and as animals get older <strong>the</strong>y will succumb.<br />
For lone females, access to healthy<br />
males of <strong>the</strong> same species in May and<br />
June each year may assist in avoiding<br />
follicular stasis.<br />
Good advice on husbandry is now<br />
available from many sources, including<br />
<strong>the</strong> British Chelonia Group and The<br />
Tortoise Trust.<br />
It is also worthwhile carrying out<br />
regular health checks to assess weight and<br />
condition pre- and post-hibernation. This<br />
can be combined with endoparasite<br />
control and ultrasound scanning of females<br />
to monitor ovarian activity.<br />
In <strong>the</strong> author’s practice most checks are<br />
done at twice yearly “parties” for “healthy”<br />
<strong>tortoise</strong>s. This enables not only <strong>the</strong> clinical<br />
check, but also allows interested owners to<br />
meet and exchange tips and techniques. It<br />
is also a very good way for <strong>the</strong> lone females<br />
with follicular stasis to meet males – speed<br />
dating for <strong>tortoise</strong>s!<br />
Conclusion<br />
Modern <strong>tortoise</strong> keeping recognises that<br />
<strong>tortoise</strong>s are reptiles and that <strong>the</strong>ir keeping<br />
requires levels of biological support as<br />
does keeping snakes and lizards.<br />
The difficulty for <strong>the</strong> practitioner is that<br />
many Mediterranean <strong>tortoise</strong>s have coped<br />
with <strong>the</strong> British climate for many years,<br />
giving <strong>the</strong> illusion that <strong>the</strong>se animals do not<br />
need such support. To overcome this, vets<br />
seeing <strong>the</strong>se animals must communicate<br />
well to educate <strong>the</strong> “traditional” keeper and<br />
demonstrate such standards in <strong>the</strong>ir<br />
hospitalisation and treatment. ■<br />
companion | 17