

occult celiac disease: a common cause of short stature - GGH Journal
occult celiac disease: a common cause of short stature - GGH Journal
occult celiac disease: a common cause of short stature - GGH Journal

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Occult Celiac Disease<br />
continued from page 1<br />
No clinical or laboratory clues enabled<br />
the investigators to differentiate<br />
between the cases <strong>of</strong> <strong>short</strong><br />
<strong>stature</strong> due to <strong>occult</strong> CD and those<br />
due to other <strong>cause</strong>s. Equally unhelpful<br />
in differential diagnosis<br />
was the age at diagnosis, length <strong>of</strong><br />
follow-up prior to referral to the GIservice,<br />
and degree <strong>of</strong> bone-age<br />
retardation. Although abnormal<br />
stool-fat excretion was found only<br />
in children with CD, sensitivity waslow,<br />
and abnormal results were<br />
found in only four <strong>of</strong> nine patients<br />
tested. However, testing for the<br />
presence <strong>of</strong> microcytic anemia revealed<br />
that all <strong>of</strong> the children with<br />
CD, but none without the <strong>disease</strong>,<br />
were anemic. A positive history <strong>of</strong><br />
past GI problems, particularly diarrhea,<br />
during early childhood<br />
also was very helpful.<br />
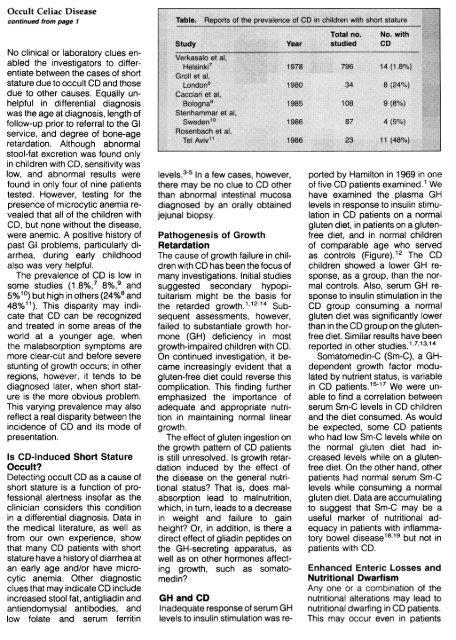
The prevalence <strong>of</strong> CD is low in<br />
some studies (1.8%,7 8%,9 and<br />
5% 1°) but high in others (24%8 and<br />
48%11). This disparity may indicate<br />
that CD can be recognized<br />
and treated in some areas <strong>of</strong> the<br />
world at a younger age, when<br />
the malabsorption symptoms are<br />
more clear-cut and before severe<br />
stunting <strong>of</strong> growth occurs; in other<br />
regions, however, it tends to be<br />
diagnosed later, when <strong>short</strong> <strong>stature</strong><br />
is the more obvious problem.<br />
This varying prevalence may also<br />
reflect a real disparity between the<br />
incidence <strong>of</strong> CD and its mode <strong>of</strong><br />
presentation.<br />
Is CD-Induced Short Stature<br />
Occult?<br />
Detecting <strong>occult</strong> CD as a <strong>cause</strong> <strong>of</strong><br />
<strong>short</strong> <strong>stature</strong> is a function <strong>of</strong> pr<strong>of</strong>essional<br />
alertness ins<strong>of</strong>ar as the<br />
clinician considers this condition<br />
in a differential diagnosis. Data in<br />
the medical literature. as well as<br />
from our own experience, show<br />
that many CD patients with <strong>short</strong><br />
<strong>stature</strong> have a history <strong>of</strong> diarrhea at<br />
an early age and/or have microcytic<br />
anemia. Other diagnostic<br />
clues that may indicate CD include<br />
increased stool fat, antigliadin and<br />
antiendomysial antibodies. and<br />
low folate and serum ferritin<br />
levels.3-S In a few cases, however,<br />
there may be no clue to CD other<br />
than abnormal intestinal mucosa<br />
diagnosed by an orally obtained<br />
jejunal biopsy.<br />
Pathogenesis <strong>of</strong> Growth<br />
Retardation<br />
The <strong>cause</strong> <strong>of</strong> growth failure in children<br />
with CD has been the focus <strong>of</strong><br />
many investigations. Initial studies<br />
suggested secondary hypopituitarism<br />
might be the basis for<br />
the retarded growth.1, 12-14 Subsequent<br />
assessments, however,<br />
failed to substantiate growth hormone<br />
(GH) deficiency in most<br />
growth-impaired children with CD.<br />
On continued investigation, it became<br />
increasingly evident that a<br />
gluten-free diet could reverse this<br />
complication. This finding further<br />
emphasized the importance <strong>of</strong><br />
adequate and appropriate nutrition<br />
in maintaining normal linear<br />
growth.<br />
The effect <strong>of</strong> gluten ingestion on<br />
the growth pattern <strong>of</strong> CD patients<br />
is still unresolved. Is growth retardation<br />
induced by the effect <strong>of</strong><br />
the <strong>disease</strong> on the general nutritional<br />
status? That is, does malabsorption<br />
lead to malnutrition,<br />
which, in turn, leads to a decrease<br />
in weight and failure to gain<br />
height? Or, in addition, is there a<br />
direct effect <strong>of</strong> gliadin peptides on<br />
the GH-secreting apparatus, as<br />
well as on other hormones affecting<br />
growth, such as somatomedin?<br />
GH and CD<br />
Inadequate response <strong>of</strong> serum GH<br />
levels to insulin stimulation was re-<br />
ported by Hamilton in 1969 in one<br />
<strong>of</strong> five CD patients examined. 1 We<br />
have examined the plasma GH<br />
levels in response to insulin stimulation<br />
in CD patients on a normal<br />
gluten diet, in patients on a glutenfree<br />
diet, and in normal children<br />
<strong>of</strong> comparable age who served<br />
as controls (Figure).12 The CD<br />
children showed a lower GH response,<br />
as a group, than the normal<br />
controls. Also, serum GH response<br />
to insulin stimulation in the<br />
CD group consuming a normal<br />
gluten diet was significantly lower<br />
than in the CD group on the glutenfree<br />
diet. Similar results have been<br />
reported in other studies.1,7,13,14<br />
Somatomedin-C (Sm-C), a GHdependent<br />
growth factor modulated<br />
by nutrient status, is variable<br />
in CD patients.1s-17 We were unable<br />
to find a correlation between<br />
serum Sm-C levels in CD children<br />
and the diet consumed. As would<br />
be expected, some CD patients<br />
who had low Sm-C levels while on<br />
the normal gluten diet had increased<br />
levels while on a glutenfree<br />
diet. On the other hand, other<br />
patients had normal serum Sm-C<br />
levels while consuming a normal<br />
gluten diet. Data are accumulating<br />
to suggest that Sm-C may be a<br />
useful marker <strong>of</strong> nutritional adequacy<br />
in patients with inflammatory<br />
bowel <strong>disease</strong> 18,19 but not in<br />
patients with CD.<br />
Enhanced Enteric Losses and<br />
Nutritional Dwarfism<br />
Anyone or a combination ot the<br />
nutritional alterations may lead to<br />
nutritional dwarfing in CD patients.This<br />
may occur even in patients













