PDF FORM - Girl Scouts of Greater Iowa
PDF FORM - Girl Scouts of Greater Iowa
PDF FORM - Girl Scouts of Greater Iowa

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
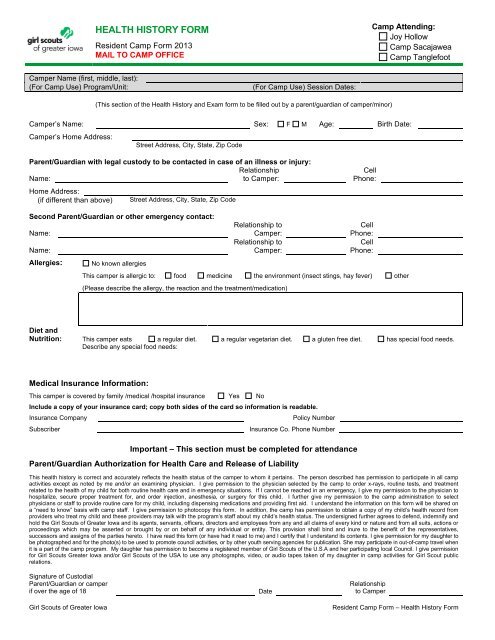
HEALTH HISTORY <strong>FORM</strong><br />
Resident Camp Form 2013<br />
MAIL TO CAMP OFFICE<br />
Camp Attending:<br />
Joy Hollow<br />
Camp Sacajawea<br />
Camp Tanglefoot<br />
Camper Name (first, middle, last):<br />
(For Camp Use) Program/Unit:<br />
(For Camp Use) Session Dates:<br />
(This section <strong>of</strong> the Health History and Exam form to be filled out by a parent/guardian <strong>of</strong> camper/minor)<br />
Camper’s Name: Sex: F M Age: Birth Date:<br />
Camper’s Home Address:<br />
Street Address, City, State, Zip Code<br />
Parent/Guardian with legal custody to be contacted in case <strong>of</strong> an illness or injury:<br />
Relationship<br />
Name:<br />
to Camper:<br />
Home Address:<br />
(if different than above)<br />
Street Address, City, State, Zip Code<br />
Cell<br />
Phone:<br />
Second Parent/Guardian or other emergency contact:<br />
Name:<br />
Name:<br />
Allergies:<br />
No known allergies<br />
Relationship to<br />
Camper:<br />
Relationship to<br />
Camper:<br />
Cell<br />
Phone:<br />
Cell<br />
Phone:<br />
This camper is allergic to: food medicine the environment (insect stings, hay fever) other<br />
(Please describe the allergy, the reaction and the treatment/medication)<br />
Diet and<br />
Nutrition: This camper eats a regular diet. a regular vegetarian diet. a gluten free diet. has special food needs.<br />
Describe any special food needs:<br />
Medical Insurance Information:<br />
This camper is covered by family /medical /hospital insurance Yes No<br />
Include a copy <strong>of</strong> your insurance card; copy both sides <strong>of</strong> the card so information is readable.<br />
Insurance Company<br />
Subscriber<br />
Policy Number<br />
Insurance Co. Phone Number<br />
Important – This section must be completed for attendance<br />
Parent/Guardian Authorization for Health Care and Release <strong>of</strong> Liability<br />
This health history is correct and accurately reflects the health status <strong>of</strong> the camper to whom it pertains. The person described has permission to participate in all camp<br />
activities except as noted by me and/or an examining physician. I give permission to the physician selected by the camp to order x-rays, routine tests, and treatment<br />
related to the health <strong>of</strong> my child for both routine health care and in emergency situations. If I cannot be reached in an emergency, I give my permission to the physician to<br />
hospitalize, secure proper treatment for, and order injection, anesthesia, or surgery for this child. I further give my permission to the camp administration to select<br />
physicians or staff to provide routine care for my child, including dispensing medications and providing first aid. I understand the information on this form will be shared on<br />
a “need to know” basis with camp staff. I give permission to photocopy this form. In addition, the camp has permission to obtain a copy <strong>of</strong> my child’s health record from<br />
providers who treat my child and these providers may talk with the program’s staff about my child’s health status. The undersigned further agrees to defend, indemnify and<br />
hold the <strong>Girl</strong> <strong>Scouts</strong> <strong>of</strong> <strong>Greater</strong> <strong>Iowa</strong> and its agents, servants, <strong>of</strong>ficers, directors and employees from any and all claims <strong>of</strong> every kind or nature and from all suits, actions or<br />
proceedings which may be asserted or brought by or on behalf <strong>of</strong> any individual or entity. This provision shall bind and inure to the benefit <strong>of</strong> the representatives,<br />
successors and assigns <strong>of</strong> the parties hereto. I have read this form (or have had it read to me) and I certify that I understand its contents. I give permission for my daughter to<br />
be photographed and for the photo(s) to be used to promote council activities, or by other youth serving agencies for publication. She may participate in out-<strong>of</strong>-camp travel when<br />
it is a part <strong>of</strong> the camp program. My daughter has permission to become a registered member <strong>of</strong> <strong>Girl</strong> <strong>Scouts</strong> <strong>of</strong> the U.S.A and her participating local Council. I give permission<br />
for <strong>Girl</strong> <strong>Scouts</strong> <strong>Greater</strong> <strong>Iowa</strong> and/or <strong>Girl</strong> <strong>Scouts</strong> <strong>of</strong> the USA to use any photographs, video, or audio tapes taken <strong>of</strong> my daughter in camp activities for <strong>Girl</strong> Scout public<br />
relations.<br />
Signature <strong>of</strong> Custodial<br />
Parent/Guardian or camper<br />
if over the age <strong>of</strong> 18<br />
<strong>Girl</strong> <strong>Scouts</strong> <strong>of</strong> <strong>Greater</strong> <strong>Iowa</strong><br />
Date<br />
Relationship<br />
to Camper<br />
Resident Camp Form – Health History Form
Camper Name<br />
The following non-prescription medications may be stocked in the camp Health Center and are used on an as needed basis to manage illness and<br />
injury. Cross out those the camper should not be given.<br />
Acetaminophen (Tylenol) Hydrocortisone cream Loperamide (Imodium)<br />
Ibupr<strong>of</strong>en (Advil, Motrin) Benadryl Cream Polyethylene Glycol (Miralax)<br />
Antibiotic cream Calamine lotion Diphenhydramine antihistamine (Benadryl)<br />
Burn Cream Lice shampoo or cream (Nix or Elimite) Dextromethorphan cough syrup (Robitussin DM)<br />
Tums<br />
General Health History: (Check “yes” or “no” for each statement)<br />
1. Ever been hospitalized? Yes No 12. Had fainting or dizziness? Yes No<br />
2. Ever had surgery? Yes No 13. Passed out/had chest pain during exercise? Yes No<br />
3. Have recurrent/chronic illnesses? Yes No 14. Had mononucleosis (mono) during the past 12 months? Yes No<br />
4. Had a recent infectious disease? Yes No 15. If female, have problems with periods/menstruation? Yes No<br />
5. Had a recent injury? Yes No 16. Have problems with falling asleep/sleepwalking? Yes No<br />
6. Had asthma/wheezing/shortness <strong>of</strong> breath? Yes No 17. Ever had back/joint problems? Yes No<br />
7. Have diabetes? Yes No 18. Have a history <strong>of</strong> bedwetting? Yes No<br />
8. Had seizures? Yes No 19. Have problems with diarrhea/constipation? Yes No<br />
9. Had headaches/migraines? Yes No 20. Have any skin problems? Yes No<br />
10. Wear glasses, contacts or protective eyewear? Yes No 21. Traveled outside the country in the past 9 months? Yes No<br />
11. Have a communicable disease? Yes No (list countries visited and dates below)<br />
Please explain “yes” answers in the space below, noting the number <strong>of</strong> the questions.<br />
Mental, Emotional and Social Health: Has the camper:<br />
Ever been treated for attention deficit disorder (ADD) or attention deficit/hyperactivity disorder (ADHD)? Yes No<br />
Ever been treated for emotional or behavioral difficulties and/or eating disorder? Yes No<br />
During the past 12 months, seen a pr<strong>of</strong>essional to address mental/emotional health concerns? Yes No<br />
Had a significant life event that continues to affect the camper’s life?<br />
(History <strong>of</strong> abuse, death <strong>of</strong> a loved one, family change, adoption, foster care, new sibling, survived a disaster, etc.)<br />
Yes No<br />
Please explain “yes” answers in the space below, noting the number <strong>of</strong> the questions.<br />
Is the camper undergoing treatment at this time, to be continued at camp? Yes, as described below No<br />
Restrictions: I have reviewed the program and activities <strong>of</strong> the camp and feel that the camper can participate without<br />
restrictions. Yes No (please describe or list specific activities and any recommendations below)<br />
Health-Care Providers:<br />
Name <strong>of</strong> camper’s primary doctor(s):<br />
Name <strong>of</strong> dentist(s):<br />
Name <strong>of</strong> orthodontist(s):<br />
Phone:<br />
Phone:<br />
Phone:<br />
Immunization History:<br />
Camper is up to date on all immunizations:<br />
Yes Required – Date <strong>of</strong> last tetnus shot: ____/____ (month/year)<br />
No, camper has not been fully immunized and I understand and accept the risks to my child from not being fully immunized.<br />
Signature <strong>of</strong> Custodial<br />
Parent/Guardian or camper<br />
if over the age <strong>of</strong> 18<br />
Date<br />
Relationship<br />
to Camper<br />
<strong>Girl</strong> <strong>Scouts</strong> <strong>of</strong> <strong>Greater</strong> <strong>Iowa</strong><br />
Resident Camp Form – Health History Form