DADS or HHSC Form - The Texas Department of Aging and ...
DADS or HHSC Form - The Texas Department of Aging and ...
DADS or HHSC Form - The Texas Department of Aging and ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
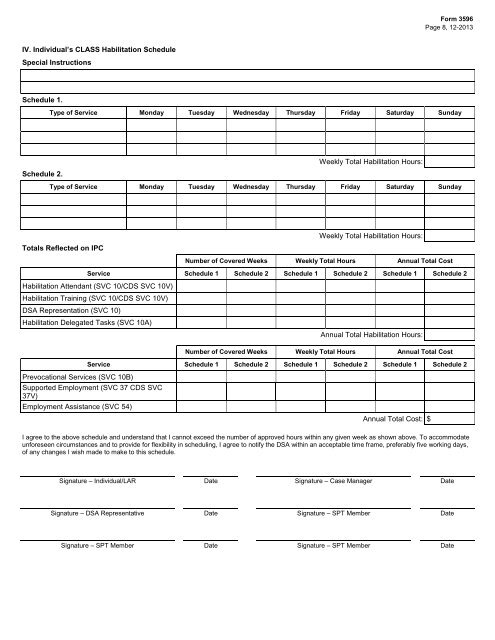
F<strong>or</strong>m 3596<br />
Page 8, 12-2013<br />
IV. Individual’s CLASS Habilitation Schedule<br />
Special Instructions<br />
Schedule 1.<br />
Type <strong>of</strong> Service Monday Tuesday Wednesday Thursday Friday Saturday Sunday<br />
Schedule 2.<br />
Weekly Total Habilitation Hours:<br />
Type <strong>of</strong> Service Monday Tuesday Wednesday Thursday Friday Saturday Sunday<br />
Weekly Total Habilitation Hours:<br />
Totals Reflected on IPC<br />
Number <strong>of</strong> Covered Weeks Weekly Total Hours Annual Total Cost<br />
Service Schedule 1 Schedule 2 Schedule 1 Schedule 2 Schedule 1 Schedule 2<br />
Habilitation Attendant (SVC 10/CDS SVC 10V)<br />
Habilitation Training (SVC 10/CDS SVC 10V)<br />
DSA Representation (SVC 10)<br />
Habilitation Delegated Tasks (SVC 10A)<br />
Annual Total Habilitation Hours:<br />
Number <strong>of</strong> Covered Weeks Weekly Total Hours Annual Total Cost<br />
Service Schedule 1 Schedule 2 Schedule 1 Schedule 2 Schedule 1 Schedule 2<br />
Prevocational Services (SVC 10B)<br />
Supp<strong>or</strong>ted Employment (SVC 37 CDS SVC<br />
37V)<br />
Employment Assistance (SVC 54)<br />
Annual Total Cost: $<br />
I agree to the above schedule <strong>and</strong> underst<strong>and</strong> that I cannot exceed the number <strong>of</strong> approved hours within any given week as shown above. To accommodate<br />
unf<strong>or</strong>eseen circumstances <strong>and</strong> to provide f<strong>or</strong> flexibility in scheduling, I agree to notify the DSA within an acceptable time frame, preferably five w<strong>or</strong>king days,<br />
<strong>of</strong> any changes I wish made to make to this schedule.<br />
Signature – Individual/LAR Date Signature – Case Manager Date<br />
Signature – DSA Representative Date Signature – SPT Member Date<br />
Signature – SPT Member Date Signature – SPT Member Date