T - Huntington's Disease Society of America
T - Huntington's Disease Society of America
T - Huntington's Disease Society of America

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
T ' ' i t A T t 4 E r , l T<br />
IVothing may be mzre chalkngtng tltan to design a plan <strong>of</strong> care tltat alloas maximal<br />
independence uith minimalrisfr--rspedalfiforpatients it/t a disease tltat not only impairs<br />
motor sfrills but ditninishes cognitiL,e abilities antl ahers personaliry.<br />
ffiu,<br />
By Suzonne lmbriglio, PT<br />
Lrntin-eton's disease (FID) is<br />
a progressive and degenerari'<br />
- ^--^"i..^",1;.;^. ^f the<br />
central nervous system that<br />
is transmitted through ar-rtosomal<br />
dominant inheritance. The incidence<br />
<strong>of</strong> HD is one case per 10,000<br />
people in the general population, and<br />
the child who has a parent rvith HD<br />
has a 50 percent chrnce ..-tf inheriring<br />
rlrc geuc and consrqLrcrrtlr acquiring<br />
the disease, lvhich alr'vays manifests<br />
itself rvhen the individual lives long<br />
enough (<strong>Huntington's</strong> <strong>Disease</strong> Socieiy*<br />
<strong>of</strong> <strong>America</strong> 1991).<br />
'l h" rr- oinn.et vrrics considerably;<br />
rvith s\,mptorns generall,v appearing<br />
bcnrccn 3U entl 50 vears; houever,<br />
in sonre cases, svmptoms have been reporteLl<br />
as eariy as 2 1'ears and as late as<br />
701's2r-5 (Nlartin and Gr-rseila 1991).<br />
The HD Triod<br />
Huntingon's disease involves a<br />
triad oIchnica] ferrurcs: cognitive deficit'.<br />
motor impairnrcnts. rnd behavioral<br />
changes. The time <strong>of</strong> onset for<br />
svmptoms in each <strong>of</strong> these three areas<br />
Varics ll'om licrson to person. as does<br />
thc r',rtc oIdetcriorrtion. Irr adtlition,<br />
s) mpton)i progrcss irrdepcn'.lcnrlr.<br />
0ognitiue defiri ts. Although n-rovement<br />
disorclers trpicall1'are the rnost<br />
conspicuor.rs feature <strong>of</strong> HI), the cog-<br />
,ritir e rhrrroes thet nlerrr i. th" prt]r'<br />
stages are the major sollrce <strong>of</strong> disability<br />
(N4ayeu.x et al. 1986). These<br />
mental changes are more variable in<br />
onset and manifcstation than are the<br />
movenent disorders.<br />
Cognitive deficits in HD may<br />
range from forgeCulness and inability<br />
to concentrate for long periods <strong>of</strong> time<br />
to severe memory deficits. Early-stage<br />
symptolns affect the persorJs ability to<br />
manage personal finances and occupational<br />
ski-Ils. As the disease progresses,<br />
deficits in recent and remote memory<br />
become increasinglv apparent. The<br />
person ma,v not be able to recall the<br />
nan.re <strong>of</strong> the \Ace President <strong>of</strong> the<br />
United States, for example, but may<br />
bc able to correctly answer a mu.Ltiplechr-'icc<br />
qLrestion. Over timc, prompting<br />
becomes a less and less effbctive<br />
sfateg.y- in dealing with information<br />
retrieval and other memorv deficits<br />
(Caine et aL I977).*<br />
Even in the most advanced stages<br />
<strong>of</strong> HD, howeve5 the person may<br />
remain cognizant <strong>of</strong> his or her surroundings.<br />
Higher-level intellectual<br />
fi-rnctions, such rs those involving<br />
"Editor's notc: For an in-t/eptlt disctusion<br />
af cognitk't r/efirit.r ttnrl their inpor'l<br />
on plrysir.al tlterapl tre(ttmmt, .tee<br />
"Bqonrl tlte Sensorimotor ^ltrip" 14t<br />
M. I'l'oherv/orf, CN[, L'o/. ]2, i\io. 3,<br />
IIaylJune 1992, pnges 63-69.<br />
Clinical Nlanageme nt
uumne Inbrig/io rtttr/ /tet'.rtdf<br />
ff<br />
\fo//ot;'nan.r<br />
potiutts tt'irfi HD<br />
# rfiroug/tour thefinu/ stag(s. HI-,D<br />
do tltq, /tandle t/te innitrrbilitl <strong>of</strong> tlteir<br />
patients' deterio ration ? Alt/to ug/t r/tere<br />
carrentb is n<strong>of</strong>ornnl supp\rt grLup,<br />
tlte treatntc.nf Iea?n meets 0n a quarter/y<br />
bask aitlt rr consulting niltrzlogistl<br />
psyc/titttrtsto discuss t/te nrl-stages <strong>of</strong><br />
HD, w/ten, says Intbriglio,"a discussion<br />
<strong>of</strong>feelngs usualfi comes ilp. W nner<br />
use the term 'burnouf.' W aclnoa/er/ge<br />
t/tnt it's ohay to cry, tlmt oe should<br />
feel attaclmt?nt.t t0 t/tese patienn. [;[lten<br />
one 0f zur patient.r dies, use nre preparulfor<br />
it, borlt in a pr<strong>of</strong>essionalsense<br />
ant/ in il Itersorut/ s(nse."<br />
acquired knorvledge and insight, r-rsually<br />
are rvell-preserved 1},'lcHugh<br />
ancl Folstein 1975; Fisher et al. 1983).<br />
A,[otor imlsoinnents. 1'he earliest<br />
signs <strong>of</strong> movement disorder in HD<br />
typicalll, appear as choretc mo'ements<br />
in thc fingersl as a result, thc pelson<br />
lvith HD may appear nervous or<br />
"fidgety." As the disease progresses)<br />
coordination deteriorates, resulting<br />
in diFficLrltics with sclllcare rctirities.<br />
Dystonic posturing, bradykinesia, or<br />
rigidiw and postural instabilitv that<br />
severely inrpairs walking also mr1<br />
ocst. Problems with speech and sw'al-<br />
Iolt'ing der clop in the later stagcs,<br />
reqr-riring a high level <strong>of</strong>clre ro n]cer<br />
the person's daily needt.<br />
Behauiorrt/ t hatgcl People with<br />
HD typically hrvc a range oIpsychiatric<br />
problems that may be manifested<br />
as behavioral probiems, such as delusional<br />
an.i paranoid behrvior, .lepression,<br />
and other alfective disorders.<br />
lbl. 12 No.5 September/October 199?<br />
Epi:odcs ot-isolation mav occur, end<br />
i mpulsc-control difliculties, aprthl,<br />
rltd Itsel self-estecma1'exist.<br />
These personality changes create a<br />
tremendous bLrrden on the pcrsoris<br />
social relationships.<br />
Mani individLrals t-ith etrh-srage<br />
svmptoms are able to live at home<br />
with a supportive family; horvever,<br />
because <strong>of</strong>the early onset <strong>of</strong>psychological<br />
problems, manv people with HD<br />
enter the mental health svstem at this<br />
tinrc. Repeated ps1 ehiatric problems<br />
and disruption <strong>of</strong> the familv social<br />
strucfure rnav lerd to placement in a<br />
psvchiatric f-aciliw that provides longterm<br />
care. This rnav mean that b1'the<br />
tirne motor zrnd cognitive problems<br />
become apparent, the individual is 1iving<br />
in a setting that is poorly eqLupped<br />
to address these s,vmptoms. Even for<br />
people r'vhose fanrilies are able to continue<br />
providing care at hone during<br />
the early stages, there may be a lack <strong>of</strong><br />
appropriate long-term care providers<br />
to meet the needs <strong>of</strong> these individuals<br />
rvhen thev enter the later stages <strong>of</strong><br />
the disease.<br />
Teomwork, To Ensure o High Quolity <strong>of</strong><br />
Life in the Leost Reslrictive Setting<br />
Stafrat the Christian Hill Rehabilitation<br />
and Skilled Nursing Center<br />
(CH) in Lowell, N'lassachusetts, prov-ide<br />
rnedical management, skilled<br />
nursing, subacute neurological and<br />
ps,vchological treatment, and traditional<br />
rehabilitation services for peoplc<br />
in thc intermediate l"transitionai";<br />
and adranced stages <strong>of</strong> HD. Patients<br />
range in age from their early 20s to<br />
late 60s and early 70s. In all cases,<br />
treatment is based on a belief that people<br />
with HD should maintain a matimal<br />
level <strong>of</strong> independence for<br />
as long as possible.<br />
Patients mav be followed b,y the<br />
treatment team thror,rghouthe final<br />
&*<br />
63m
Physical Therapy and HD:<br />
- ' From A Social Worker's Perspective<br />
-' I ;,:- eople with Hunting;ton's disease,4ro;e' u'hat's happeling to dretrl,"<br />
- emphasizes<br />
I -- 'social lvorker Paui F-erreira, NIS\V. "They mav still be anrbulator,r'i br-rtheir<br />
,- coordination skills are decrcasing. l-hey have less endurance tl-ran theY trsed<br />
to have, thel'hn1,e difficulq' transferrir.rg fiorn chair to bcd, and the,v rnay need safety<br />
devices to pieventhem fronr falling or sustairrilg head injuries...Thel' 11gecl a lot r:f<br />
ernotional supporto help thenr deal u'ith thcse losses in ph1'sical function. A cr-itical<br />
fbctor in the tr-eatur.rent <strong>of</strong> these patients is the attitude <strong>of</strong> the phvsicai therapist, lvho<br />
rnust have a positive-but realistic--outlook." Both ps)'chodreraPist and case matiageq<br />
Ferreira coordinates the tleatment team tlrat lr,orks rvith patients rvidr HD at tbe<br />
C|u-istian Hill Rcfiabilitatior.r and Skilled Nursing Center ir.r Lorvcll, N4assachr.rsetts.<br />
"Ph,vsical<br />
tlrerapy is a major compone nt <strong>of</strong> the trcatmcnt progfarn for pcople rvith<br />
"TIre<br />
rnid-stage FID," says Fcrreira. trich.part is that HD isrlt just a ph1'sical problem.<br />
It's the ph1,sica1 therapist'sjob to clistinguish anrons changcs relatcd to ph1'sical deterioration,<br />
mental detcrioration, and tllc patient's elt-totional state'"<br />
As Suzanne Imbriglio, P! discusscs o1 drese pagcs, sornc patients t'ith HD 1.ray<br />
"For<br />
strongly resist physical therapl.: these patients, to participate in phl'sical therapv is<br />
to aclilit that the1, are sick," cxirlains Fcrreira. "Some paticuts are t(xr deep in dcnial to<br />
to do that. In otlter cases, the disease affccts the mind, rcsultin$ in a psych6{c thought<br />
process. Son-re patients rnay be depresscd-r'vhicli tvpicall1'affects dreir urotivatiou aud<br />
iself-startilg' 'pzrssinQ<br />
abiliq'-or may leel guilq' for thc diseasc on' to drcir cfiildre1'<br />
Sone studie suggest that the incidence c-,f suicidc tr.rav be l.righer among peoplc rvith<br />
HD than among the general population. Ald then thcrc arc patients rvho u'ant to do<br />
anlthingthcy can do to help themselves." Ferrcim adds th:rt a paticnt's preexisting<br />
"If<br />
persolaliq' 16its tnay be agrplifred by thc disease. tfie patient telded to be anrit'rus<br />
tr negative befc,rc theonset <strong>of</strong> F{l), he or she will probably have a big problenr t'ith<br />
an-xiety as the disease progfesses; if the patient tended to be optimistic, that will be a<br />
big help as tiure goes ott."<br />
Florv does the social rvot-lier help the patient accept physical therapvl<br />
"Patients<br />
leecl to ex;'rlc.rre their- feelings about IfD,. .Iltdrei/re ir.r deniai, for eriamprle,<br />
1'ou cirtr't'force'them out <strong>of</strong> it. L-rstcad i'ou tDr to find some t'indolv <strong>of</strong> oppol'tunirv'<br />
it's important to talk about the real-ities <strong>of</strong> da1'-16-6|n" 6le' 'FIou'' are l'ou doiugi Are you<br />
talling dorvn a lot? A.r-e ),ou able to r.valk around as rnuch as you used tol'As the patient<br />
'RetnemLler<br />
becomes rnore comfortable talking about these problerns, )rotl can sa1"<br />
phvsical therapi'f lVlaybs rve could tr.v drat. N'[at'be it could help'' "<br />
When Ferreir-a sepses during a counseling sessiotr that a patient nral'be readl' f61'<br />
pitysical therapii he lr-ra1'rvalk u,ith tl.re patient to the ph,vsical drerapy deparlrnento<br />
h1d out rvhetfier a ph,vsical therapist can mect rvitlt the patient right au'a1i L]ntil the<br />
patient becorr.res familiar rvitlt the ph1'sical tlierapist. F-erreiralso may "sit in" otr the<br />
phi'sical thcrapy scssions.<br />
"This "After open door policl'can be hard on the PG," he sa1's' all, tl"rey're very<br />
busti In addition to 2J patiertts'w4lo ltave I-ID, diey also treat geriatric patients and<br />
patients with subacute tratunatic brain iljury But because <strong>of</strong> the day-to-da-V variability<br />
among patients rn'ith HD, dris is the method that lr,orks best." Ferreira pauses.<br />
"I guess<br />
you could say that PG havc to str-il;e ivlile the iron is hot."<br />
Psycholropic Medicotions<br />
In addition to lcrorving rvhether a syrxptom is related to thc tlisease Process or to<br />
the patient's aruiiegi the physical therapist also ntust r.urclerstand the eflects <strong>of</strong>pst'chotropic<br />
r.nedications.<br />
"There are basical\, fbur categories <strong>of</strong> drr-rgs r,rsed u'ith patients n'ith FID," explains<br />
Ferreila,<br />
"a1l <strong>of</strong> rvhich tnal' l1n1's an irnpact on ;'l.rrsical therapl'treatnrent' f'he first<br />
includes the ner-rroleptics, suclr as Flalclol", ri'liich, in lou'dclsages-'l to 10 mgstages,<br />
inciuding death and dying.<br />
Some fanrilies believe tl-rat when the<br />
paticnt has reached the last stage <strong>of</strong><br />
the disease, he or she should be transferred<br />
to a nursing horne for medical<br />
mallagement, whereas other families<br />
believe that the patient should<br />
remain in familrar surroundings.<br />
T-\^, r^ l^, -.^'..-.nrent<br />
udy-lw-ud) 1rrarraSLt and care<br />
<strong>of</strong> the person rvith HD are delivered<br />
bJ, u tet- <strong>of</strong> nembers from the follouing<br />
disciplinet: nursing, restorative<br />
sen'ices, health and special education<br />
sen ices, and :ocial services.<br />
h'ursittg carc.'Ihe nursing staffdeal<br />
witl-r such issues as l) the monitoring<br />
<strong>of</strong>dietary intake because <strong>of</strong>eating and<br />
f'eecling problems that ma1 rcsult in<br />
chokingl 2) skin management problems<br />
resulting from excessive invoLuntarv<br />
moverrents; 3) deficits in<br />
activities-<strong>of</strong>-dailpfvltt* (ADL) skiJls,<br />
rvhich may result from incoordination<br />
and deteriorating psychomotor<br />
functions; and 4) pharmacologicai<br />
management.<br />
Rrstotuti:ce serttins. These services<br />
include speech therapy, occupational<br />
therap1,, and physical therapir Physical<br />
drerapy is beneficial in improving<br />
or stabilizing motor abiliti! preveuting<br />
contracrures, and adapting the<br />
enr.ironmento foster independence<br />
rvl'rile ensuring safety. Occupational<br />
thcrapy sen'ices help tJre patient maximize<br />
coordination abilittes as rvell as<br />
ADL skills. \\-itlr speech therapy,<br />
people witli HD may be able to improve<br />
intelJigibility; sonre may benefit<br />
frorn the use <strong>of</strong> augmentative speech<br />
der,'ices. The speech therapist also is<br />
responsible for evaluating dysphagia.<br />
Healtlt and special education seraice-s.<br />
Provided by health educators<br />
and special education tcaclrers, these<br />
servicef include cognitir.e retraining,<br />
rnemor)/ and awareness training, and<br />
"self-ir-nprovement" classes especiaily<br />
designed to help people rvith HD<br />
improve their self-esteem.<br />
Soria/ srrt'ires. Peoplc u itli HD<br />
require specialized intenrention strat-<br />
64 Clinical N4anagement
egies to defiise or avoid potentiall,v<br />
explosirc episodes. Because <strong>of</strong>poor<br />
impulse control, patients rvith HD<br />
rnay become easily frustrated rvhen<br />
their needs are not quickly met. Thev<br />
also may benefit from psychotherapv<br />
that addresses their grief, fear, and<br />
concerns about loss <strong>of</strong>firnction. Because<br />
judgment may be impaired and<br />
impulsivity may increase as the disease<br />
progrcsses, thcsc paticnrs ma1 require<br />
close nrorritoring and supervi=ion.<br />
Maintainine rcgrrlar la mil1' contrct<br />
and familv counseling also are social<br />
services priorities (see "Physical Therapy<br />
and F{D: From a Social \\brker's<br />
Perspective," pages 6.1-65).<br />
A Never-Ending Educotion Proces<br />
Whether it's the education <strong>of</strong> a ner,v<br />
ph1'sician on the medical staff or the<br />
continuing education <strong>of</strong> direct-care<br />
staff,, ongoing training is integral to<br />
the success <strong>of</strong>anv treatn-rent program<br />
for people with HD-no mafter hor.v<br />
big or small the facility. To treat the<br />
whole person, everyone on staffmust<br />
have an understanding <strong>of</strong>the disease<br />
process. Classes mav be <strong>of</strong>fcred for<br />
both day and evening shifts on such<br />
topics as "Wl.rat Is FIDi", "\Vhat the<br />
Person witlr HD Can Do," and"Hor<br />
to \\hlk with a Person with lID."<br />
Ciasses, rvhich mav be scheduled on<br />
a quarterly basis, for example, also<br />
can be provided on bchai ior manegement,<br />
restorative services, and feeding<br />
protocols. Experienced members<br />
<strong>of</strong> the treatment team may be the<br />
best teachers.<br />
Intoke ond Assessmenl<br />
Upon admission to the facilirv,<br />
each patient undergoes a colnpreher.rsiv'e<br />
medical, neurological, and<br />
psychologrcal asscssrncnt perlormed<br />
by the attending physician and the<br />
co nsulting neurologi st/ps1-chiatrist<br />
and an intake process @gure 1) that<br />
mav be facilitated by any mernber <strong>of</strong><br />
the treatment team.<br />
\/ol. I I \o.5 Seprcmbcr/Oerubcr l,lQl<br />
mav rcdnce chorcic movement. Llpon adnrission to our progranr, son-re people r,vith<br />
FID are receiving too higli a dosage, and if you get too far outside tl're theraper-rtic<br />
lvindou,-, tl.re medication actually rnal'make rnatten rvorse, resnlting in side efllcts sgch<br />
a:- d1,516n1" or rigiditv and afrecting the abiliry* to walk. If a person is not realJy bathet"ul<br />
by dre choreic lnovements, it ma1' 116g be necessary for tl.rem to take these drugs at all."<br />
I,trreira sirys that among younger people widr HD, s).mptoms ma1. [s sirni]ar to those<br />
<strong>of</strong>Parkinsorls disease, in u'hich rnovenent tends to be stiffrather than choreic.<br />
Nledication for aruxiety, sr-tch as Ativan'n', mav be used in lolv doses with these patients<br />
rvhen thev are prone to explosiv'e or ag'glessive behar"ior, notes Ferreira. Antidepressants<br />
also rnav be helpfi.rl.<br />
"lldivicluals lvith HD mav har.'e an underffig depression drat is not readil1' appryent,"<br />
he eiaborates.<br />
"Traditional sylllptorn such as a depressed rnood, sleepingdisorders,<br />
and'"veight gain or loss may not be evident. In FIn, the patient's mood may be ilat,<br />
irritable, or extremelv labile. Drugs such as Prozac@ and sorne <strong>of</strong> the tr-icyclics rnay<br />
help." The fourd.r category <strong>of</strong> rnedication incl-rdes drugs such as ltgretoln! and lithium,<br />
which rnav help people with HD rvho hare qytrerne mood sr,vilgs.<br />
The Teom Efforl<br />
Because <strong>of</strong> the physiological, cognitir,'e, ancl behavioral changes and the effects <strong>of</strong><br />
medications, it is especialll'- i-rn;lortant for the treatrnenteam to have r-egular communication.<br />
An interclisciplinary'st;rffmeeting r,vith physical drerapists, occupational therapiss,<br />
speech d.rempists, ntirsing stafi and social workers takes place weekly for the revierv <strong>of</strong><br />
cases' and qpicaily includes the aftending physicians and the consulting psvchiatrist.<br />
Quarterly and annual tneetings are held fbr each patient, with special tearn meetings<br />
calied as rleccssary<br />
In adclition to team'"vork among stald savs Fbrreira, there is a kind <strong>of</strong> tearn'"vor-k<br />
among patients.<br />
"Patients<br />
rvith Hl) don't need to be isolated from patients with other<br />
qpes <strong>of</strong> disorden. lVe group patients according to linctional abilities. In social i:rteractions,<br />
patie nts v"ithHD mtry be irnpulsive or aggressive. Holvever, il many instances, the<br />
emotional problens <strong>of</strong> patients with HD and patients with brail injuy, for e:
T R T A T [ i t N T<br />
f or nrany patients with <strong>Huntington's</strong> disease (HD), de-<br />
F .t.ur.d pirysical activity may result in degeneration drat<br />
I *.u^ too early to be attributed to the diseasc process<br />
alone. This suggests that nraintetrance or<br />
temporary irllfiIorr.rn.nt <strong>of</strong> fu nctional<br />
abilities within the limitations <strong>of</strong> tire HDilvolved<br />
"Among<br />
the 40 potienh wilh whom I hove<br />
centrai nervous svstem may be<br />
workeduring the posl seven yeors, loss<br />
possible in the early stages ffoung ii86). <strong>of</strong> $rength in lhe eorly sloges wos nol 0<br />
A program <strong>of</strong>active exercise based on the<br />
uatiends identified needs is recomrnend- significont foctor for lhose who remoined<br />
.a 6Ioy Hicks, and Barraclough 1985; ortive. When lhere is o decreose in octivity<br />
Hayden 1981).<br />
os the diseose progresses, los <strong>of</strong> stren$h<br />
The physical therapy evaluation may<br />
moy be consideroble. Although weight lifting<br />
moy increose intoordinslion ond mus-<br />
indicate that the oatient needs to develop<br />
an awzlreness <strong>of</strong> the differences benveen<br />
muscle tension and muscle relaxation; cle tension, it moy be effective in building<br />
learn controlled breathingte.ldq:.tl<br />
musde strenglh for some potients."<br />
matntaT or lmprove coorclmauon, rlqlbiliry<br />
and balalce; and, when applicable,<br />
-lnez Peocock<br />
increase muscle stength (Pcacock i987).<br />
Routine active exercise for neck, trunk,<br />
and extrernities and firnctional activities forbalance and coordi-<br />
;"; ; m;ftant cornponents <strong>of</strong> the treatrnent program;<br />
wa$ing should be part <strong>of</strong> the daily regimen (Chiu 1989).<br />
It is irnportanto begirl an ongoing exercise program early<br />
in the course <strong>of</strong> the disease befotz many patients and fanillies<br />
believe there is a need for it. At this point, tle patient still rnay<br />
By Inez W. Peocock, PT<br />
ffi,,<br />
Durir-Lg the initial nvo rveeks, the<br />
patient is given time to "get used" to<br />
the new surroundings, and the treatment<br />
tearn assesses motor skills and<br />
coordinarion (IrigLrre 1 ). Phvsical<br />
therapy evaluation documents range<br />
<strong>of</strong> motion, muscle strengd-r, leg lengdr,<br />
trurrk mohiliry standing enJ sining<br />
balance, prosture, sensation levels, cardiopulmonary<br />
status, the existence <strong>of</strong><br />
pain, the ability to rriake transfers, gait,<br />
tlre need for special equipnrent, and<br />
the need for special tests. Also assessed<br />
by tJre team: spceclr, sw'allowirrg, anJ<br />
.^o.ir,rze firnetinns<br />
-'b^'-"<br />
Figurcs 2, J, and -[ are examplcs<br />
<strong>of</strong> some <strong>of</strong> the fbrrns used in rnotor<br />
skill and cognitive assessment. These<br />
particular examples are based on the<br />
precision teaching method (N4c-<br />
Greery 1984; Pennlpacke5 Koenig,<br />
and Lindsley 1972), rn which tlie<br />
therapist or teacher breaks dorvn each<br />
task into separate movements withirr<br />
1S-second intervals and records the<br />
per-minute rate at which these movements<br />
are con-rpleted. Both ability and<br />
thefluency <strong>of</strong> movement are assessed,<br />
with the goal <strong>of</strong> increasing the rate at<br />
which a patient is able to perform a<br />
task. IJsed prirnarilf in special education<br />
settings, this method can be<br />
useful widr patients rvith HD because<br />
these patients have many <strong>of</strong> the sarne<br />
.leficits tlrat people in spccial education<br />
settings have. In assessing reading<br />
skil1s (trigure 2), for example,<br />
the tcster wants to detcrrnine not<br />
onLy whether the patient understands<br />
what he o[ she reads, but whether eye<br />
movements already may have begun<br />
to decrease because <strong>of</strong>the disease,<br />
resuhing in what may appear to be<br />
slorved comprehension.<br />
When the various assessments are<br />
brought together to provide a comprehensive<br />
functional and clinical picfure<br />
<strong>of</strong> the patient's status, the team formu-<br />
Iates an individualized plan <strong>of</strong> care.<br />
'Friendly<br />
Persuosion"<br />
Persons in de middle stages <strong>of</strong> the<br />
disease nsually are all too aware <strong>of</strong> a<br />
number <strong>of</strong> losses, both physical and<br />
mental. They also may be aware <strong>of</strong> the<br />
degcn erative and progrcssive nature<br />
<strong>of</strong> dre disease. Thcy may feel helpless<br />
Clinical Management
; I I A T I t I N T<br />
ball. Music can accompany movement-pattern e
i F E t . T L l E t { T<br />
ffi,'<br />
i:{{<br />
: .:t,, :': :/.1:'!<br />
which in turn help to bolster selfesteem.<br />
After meeting u'ith some level<br />
<strong>of</strong> success, the paticnt may be more<br />
open to discussing the aspects <strong>of</strong>physical<br />
functioning with which he or she<br />
is hai,ing the most dificulgv. The therapist<br />
and patient together can adapt the<br />
environment or provide a-ltematives to<br />
conpensate for the loss <strong>of</strong> function.<br />
A"lurd se//." The process described<br />
above <strong>of</strong>ten is a slorv one. Bv the time<br />
patients reach the middle stages <strong>of</strong> the<br />
disease, thev already have had to deal<br />
lvith a multitude <strong>of</strong> "failures," an6lbecause<br />
<strong>of</strong> disease-related cognitive<br />
losses and emotional imbalancetheir<br />
abiiiq'to cope with these fai.lur-es<br />
mav he sevcrclv comoromised.<br />
'"-'-r-' At<br />
FF nowting thnt I Tnould this point, many people rn'ith HD<br />
isolate themselves. Horverter, a<br />
to /mae at /east some conn-o/<br />
patient mav seek out one person frorn<br />
olu' ft'erj siuarion. tlre nrimarw caresivinrt staff and conpatient<br />
J -*'-b.'^'-b<br />
I try to a//oa: tlrc Patient sorn e/ement<br />
0f cznrrzl in finding solutions.<br />
linue to respond well to this person,<br />
as in the case described below.<br />
Tltis drffers somerCIhatfrom tlte<br />
LH's Story<br />
traditional role <strong>of</strong> t/tu'apkt as I'ae LH had had a series <strong>of</strong> near falls,<br />
experienced it in t/te past. In many<br />
traditional settings, tlte tlterutpist<br />
and her therapist had begun to discuss<br />
some safety guidelines rvith her.<br />
LH became angry rvith her therapist<br />
?nafres tnzst <strong>of</strong> tlte treannent decisions,<br />
such as c/toosirtg t/te treatment<br />
and stated that she would not see hirn<br />
again for "arry kind <strong>of</strong> therapy." LFI<br />
regxmen and settirtg tlte goak. But clearly was unable to cope ivith the<br />
then, in nrun! troditiznol settings,<br />
tlte patient is going to ger bettaror,<br />
deterioration in her physical functioning<br />
and furthermore associated her<br />
at t/te oer! /east, /earn to com-<br />
therapist rvidr this deterioration. LH<br />
eventually turned her back on her<br />
pensatefor a drsability and get on<br />
speech therapist and occupational<br />
airlt ltfe, and therefore night not therapist as u,ell, becoming reclusive<br />
take lift-t/trcarening risrts. But rt;lten<br />
lou frnout ysu're going to become<br />
tnore and more i// ancl nentuafit<br />
and withdrawn; holveveq she did<br />
maintain a relationship with one <strong>of</strong><br />
the health education teachers. This<br />
tearher hceemn rrerrr imrrnrferrt in<br />
die frorn tlils debilitating disease,<br />
the care and treatment <strong>of</strong> LH.<br />
lou migltt thinh,'Wty ilot take I-FI's treatment plan r,vas revised<br />
a @a/k u;it/tout rny /te/ma? So altat<br />
if I fa// and get a ltematonm?'<br />
to allow much <strong>of</strong> thc physical therapy,<br />
occupational therapr5 and speech therapy<br />
to be provided by the one person<br />
It's aur clta//enge to conaince t/te<br />
LH trusted. Although this stratcgy<br />
patient tltat tltere arv altenutiDes."<br />
n'as far from thc traditional delivery<br />
-$v7sluts Intbriglio<br />
oFserr-ice in many skilled nursing<br />
centers, the outcome r /as successful:<br />
LHt dignity was preserved because<br />
she was provided with a way to continue<br />
fi.rnctioning at her optimal level.<br />
LFI now is much less reclusive<br />
and allows her therapists to observe<br />
her periodicalil so that her progress<br />
can be charted and her program can<br />
be updated.<br />
lsues o{ So{ety ond Self-Determinotion<br />
Because <strong>of</strong> the nature <strong>of</strong> the HD<br />
process, faulqv judgment and impulsivity<br />
may result in difficult or<br />
unsafe situations.<br />
For some patients, the fear <strong>of</strong> selfinjury<br />
is enough to motivate them to<br />
adapto their new limitations. These<br />
patients may rnore readily accepthe<br />
idea <strong>of</strong>wearing knee and elbow pads<br />
or a protective helmet, for example,<br />
because using these aids means maintaining<br />
the ability to walk without help<br />
or supervision. Patients who deny<br />
their limitations or who are not intimidated<br />
by the possibility <strong>of</strong> self-injury<br />
howeveq pose difficult chailenges to<br />
the treatment team.<br />
Nthough it is the responsibiliry <strong>of</strong><br />
all stafrto ensure the safety <strong>of</strong>patients,<br />
the physical therapistypically is the<br />
one r,r,ho assesses the condition <strong>of</strong> a<br />
patient when physical functioning and<br />
safety are in question. It may be very<br />
difficult to convince the person whose<br />
judgment has become faulty or whose<br />
physical functioning has deteriorated<br />
that he or she now needs assistance.<br />
There is nothing more challenging,<br />
horvever, than developing a plan <strong>of</strong><br />
care that allows maximal independence<br />
with minimal risk to safety<br />
and well-being.<br />
There are no easy or set "cookbook"<br />
answers to the problems <strong>of</strong><br />
HD. In developing approaches to<br />
solve these problerns, it may help the<br />
therapist to envision himself or herself<br />
in the patient'situation. How<br />
important is it for you to have control<br />
over a given situation inyurltfel<br />
Clinical \,lanagement
1 R i A T i l 1 T i . l I<br />
The patient may go through a period<br />
<strong>of</strong>anger or depression or both as<br />
changes occur in physical starus. \\tth<br />
counseling and support, hor,vever,<br />
these changes can be "turned around"<br />
into something more positive. The<br />
patiEnt may learn that he sti1l can go<br />
out to the donut shop as long as he<br />
wears a helmet or knee pads for protection<br />
or that using a wheelchair<br />
does not prevcnt him flrom going<br />
out to the Monday night bingo<br />
gamc. Helping the patient nraintain<br />
a normal routine while adjusting to<br />
physical changes is essential.<br />
The Fomily os Future Potienl<br />
Because <strong>of</strong> the genetic component<br />
<strong>of</strong> HD, many family members <strong>of</strong><br />
patients are at risk for FID and<br />
therefore may be patients themselves<br />
in the furure.<br />
tramily members must deal with<br />
many emotions when placing a<br />
patient in long-term care. When the<br />
patient is a child <strong>of</strong>an unaffected<br />
parent, the parent's concerns primari-<br />
Iy revoive around obtaining highquality<br />
care for the chi1d, and the parent<br />
feels some reliefr,vhen this care is<br />
found. When the patient is a parent,<br />
the children are themselves at risk for<br />
HD and therefore have additional<br />
concerns. The childrcn oIpatients<br />
with HD require support and the<br />
opportuniry to talk in-depth abour<br />
the rype <strong>of</strong> care the patient wiil<br />
receive, pardv because they know<br />
they may need that care themselves<br />
one day.<br />
Family members who are themselves<br />
at risk for HD rypicalJy have<br />
been caregivers in the past and therefore<br />
may have some very helpful ideas<br />
about how to deal with the patient.<br />
This information can be vital, particularly<br />
upon admission. This transfer<br />
<strong>of</strong> information also is a good way for<br />
that family member to become accustomed<br />
to the notion that the patient<br />
rnill be cared for by someone else.<br />
Very <strong>of</strong>ten the "at-risk" family mem-<br />
Vol. 12 No.5 September/October 1992<br />
ber is esneciallv interested<br />
the<br />
therapeutic interventions available to<br />
th" LrrL ^.tio.r r.rl tl'"t C-ilr, dIIU tll4t lall/ll) -"-ht. rrrLlrluLr<br />
PAUlllL\<br />
sometinies looks to the therapist for<br />
hope that treatment will delay or preverrt<br />
the inevitable degeneration.<br />
Working with families who are at<br />
risk takes a great deal <strong>of</strong>sensitivity<br />
on the part <strong>of</strong>the therapist. In addition<br />
to meeting the needs <strong>of</strong> tlie<br />
patient, the therapist must provide<br />
connseling, teaching, and support to<br />
the family, making appropriate counseJing<br />
referrais as needed.<br />
It has been r,vell-documented that<br />
thc qualiry <strong>of</strong> care given to patients<br />
rvith HD-as perceived by the patients'<br />
children-decply affects rhe<br />
childlen's ability to face their orvn<br />
illness. The perception <strong>of</strong> the quality<br />
<strong>of</strong> care also influences their abilig<br />
to make use <strong>of</strong> pr<strong>of</strong>essional services<br />
( Martindale 1987 ). A slogan commonly<br />
used in the HD communiry<br />
underscores this need For quality<br />
care: "Until there's a cure) there's<br />
only care." crt<br />
Suzanne Imhriglio, PT, is Director<br />
<strong>of</strong> Restoratice Seroica, C/tristittn Hill<br />
Relnbilitation and S li/led l{ursittg<br />
Ccnte6 19 y'arnurn St., Lor'le//, l,lA.<br />
The author tlunls Jim Po/lard, Paul<br />
Ferreira, and Tbn Imbrigli<strong>of</strong>or their<br />
assistance in uriting rhts article, and tie<br />
HD treatment te(tm at C/tristian Hill<br />
for tlteir continu&/ roopff(ttizu.<br />
For more informotion obout<br />
Huntingfon's diseose, cqll the<br />
Huntingfon's Diseose Sociefy:<br />
<strong>of</strong> Americo, 212 / 242-1968.<br />
REF'ERENCES<br />
Caine ED, Ebert NIH, \\'eingartner<br />
H. An outline for the analysis <strong>of</strong><br />
dementia: the memory disorder <strong>of</strong><br />
<strong>Huntington's</strong> <strong>Disease</strong>. Neurologt<br />
1977;27:1087 -1092.<br />
FisherJNl, KennedyJL, Caine ED,<br />
Shoulson I. Dementia in Hunt-<br />
"'b'"" inqton's " disease' a cross-seclional<br />
analysis <strong>of</strong> intellectual decline.<br />
Adv Neurol. 1983;38: 229-238.<br />
Fluntingtorls <strong>Disease</strong> Sociery <strong>of</strong><br />
<strong>America</strong>. Facts at a G/ance. New<br />
lbrk, NY: Huntingtoris <strong>Disease</strong><br />
uvLlLL/<br />
q^^:^-. ^t Ur r<br />
^ !rlr!r1L4)<br />
^^:^^. Iggl.<br />
Martin JB, Gusella JE Huntingtorls<br />
<strong>Disease</strong>: pathogenesis and management.<br />
N EngJ Med. I99l;<br />
315:1267<br />
-1276.<br />
Martindale B. <strong>Huntington's</strong> chorea:<br />
some psychodynamicseen in<br />
those at risk and in the responses<br />
<strong>of</strong> the helping pr<strong>of</strong>essions . Britislt<br />
Joumal <strong>of</strong> Pslchiatrl. 1987 ;<br />
| 50319-323.<br />
Mayeux R, Stern d Herman A, et<br />
al. Correlates <strong>of</strong> early disability in<br />
F{untingtods D rsease. Ann<br />
Neurol. 19 B 6;20 :727-731.<br />
Mccreery P Frequency and the<br />
standard celeration chart: Necessary<br />
components <strong>of</strong> precision<br />
teaching. Joumal <strong>of</strong> Precision<br />
Tiaclting. 198 4 ; 5 (2):28-36.<br />
NlcHugh PR, Folstein Mtr Rychiatric<br />
syndromes <strong>of</strong> <strong>Huntington's</strong><br />
chorea: A clinical and phenomenological<br />
study. In: DF Benson,<br />
D Blumer, eds. Pslcltiatric Aspec*<br />
<strong>of</strong> Neurolctgic <strong>Disease</strong>. New York,<br />
NY Crune and Stratton; 1975.<br />
Pennlpacker HS, Koenig CII,<br />
Lindsley OP.. Handbook <strong>of</strong> tlze<br />
Standard Beltavior Chart. Kansas<br />
City, KS: Precision Medta 1972.<br />
SUGGESf'ED READINGS<br />
Harper PS, ed. <strong>Huntington's</strong> <strong>Disease</strong>.<br />
London, Engiand: W.B. Saunden<br />
and Co.; 1991.<br />
Shoulson I. <strong>Huntington's</strong> disease:<br />
cognitive and psychiatric features.<br />
Neurolog 1990 ;3:I 5 -21.<br />
Young AB. A Neurologist Speaks<br />
Alout Fluntingtoni <strong>Disease</strong>. Excetpt:<br />
from Dr Young\ speech to tlte annual<br />
workhop. NewYork, NY <strong>Huntington's</strong><br />
<strong>Disease</strong> <strong>Society</strong> <strong>of</strong><br />
<strong>America</strong>;1986.<br />
w<br />
6effi
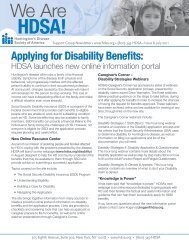
Intoke: Regording your fomily membe/s core while home wiilr fomih-<br />
1. Who assisted u'ith self-care?<br />
\Vith u,hich tasks?<br />
Bothing: Dressing: Grooming: Toileting:<br />
Upper body- Upper bod-v- Brushing hair fusist with pants up/down -<br />
Lower bodv- Lorver body- Brushing teeth - Help complete task<br />
Hands/face -<br />
Socks/shoes - Shaving - Commode was used<br />
Underclothes only - Makeup - Bathroom was used<br />
Nail care -<br />
Which tasks were the most difficulti \\hvi<br />
2. \Ahen did assistance wirh homemaking skills become necessary?<br />
Which chores could your family member still perforn-r independentlyi<br />
Which chores could he or she Derform oart <strong>of</strong>?<br />
3. Sho assisted your family member with eating?<br />
\Vere there anv "tricks" that made<br />
this task easier? (such as using special cups or utensils, avoiding certain t-vpes <strong>of</strong> food, using special chairs or clothes)<br />
4. Please describe the position used by your family member while he or she was eating or being fed:<br />
Heod:<br />
Trunk (chest) Hips: Legs ([eet):<br />
Up - Forward - Back in chair - Flat on floor -<br />
Down _ Backward _ To one side ieft/right - Resring on stool -<br />
Foru,ard - Sidervays right/left - Fonvard in chair - In constant motion -<br />
Straight ahead - Upright -<br />
Under buttocks -<br />
Othei (please describe): Orher (please describe): Other (please describe):<br />
5. Did your family member have an,v difficulty sitting in a chair? Yes - No -<br />
Which type <strong>of</strong> chairs did he or she use? Sling back chair - Straight backed chair -<br />
Wheelchair - Lounge chair - Rocking chair - Recliner (e.g.,Lazy Boi€) - Didn t use a chair -<br />
Did you use anything to help your family member stay in the chair?<br />
A sheer tied around the chair - A tray placed over chair - Never used anything -<br />
\\hen did you use something to help your family member stay in the chairi<br />
During meals - In the morning - In the afternoon - In the evening - In the middle <strong>of</strong> the night -<br />
6. Did you need to help -vour family member u'alk? Yes - No -<br />
Did you provide a wheelchairl Yes - No -<br />
How did you help,vour family member walk?<br />
One person held onto belt - One person held onto hips - One person held onto arm -<br />
'livo<br />
Didn r let him/her rvalk - Tivo people on each arm - people held hands - Two people held onto belt -<br />
7. Is there anyrhing yor.d used during your family member's stay at home that made his or her stay easier for you?-<br />
ffiro<br />
Designed by Linda Anderson, OTNL, 1990<br />
Figure 1. Sample intahe form used hy rhe <strong>Huntington's</strong> disease treatment€am to he lp assess tlte patient's functional lroels--and os part <strong>of</strong> a<br />
strateg to help ensurefamifinoolaement in the patient's care.<br />
Clinical Management
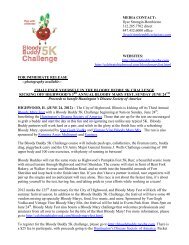
Hunlinglon's Diseose AssessmenlJVlovemenls to Moniior<br />
l. ADL Streening ond Asesment-ADL screening 0nd ossessment will be completed.<br />
ll. "The Big Six'-Specific movements will be torgeted bosed on the informotion obtoined through these ossessments.<br />
lll. Augmentotive Communicolion-Movements rlsed in communicotion will be osessed.<br />
lV. Nutrition-Movements used in the wrilten ond verbol expression <strong>of</strong> nufillionol knowledge will be osessed.<br />
ll. "The Big Six", Hond Usoge<br />
Reach for 9" target<br />
Reach for 6" target<br />
Reach for 3" target<br />
Pointo 9" target within 12" <strong>of</strong> target<br />
Point to 6" targetrvithin 12" <strong>of</strong>target<br />
Point to 3" target within 12" <strong>of</strong> target<br />
Touch 9" target<br />
Touch 6" target<br />
lbucll 3" target<br />
Grasp release ("Hook")<br />
Crasp release ("C1'lindrical" )-lcft and righr<br />
Grasp release ("Lateral";-hands for all<br />
Grasp release ("Three Jaw Chuck")-grasps<br />
Grasp release ("Pincer")<br />
Grasp release ("f ip Pinch")<br />
Aim place object onto 8"-by- 11<br />
" target<br />
Aim place object onto 6" by 8" target<br />
Aim place object onto 4" bv 6" target<br />
Thist doorknob<br />
Twist 1/2" nut onto bolt<br />
Grasp pull cards from holder<br />
lll. Movements Used in Augmentotive<br />
Communicotion (to prepore potient to use ommunicotion boord)<br />
Imitate therapist as therapist reaches for target<br />
Poinr to l" snr;:res leFto rioht-fnn tn hottnm<br />
Point to 1" colored squares on 9"-X-11" grid<br />
Point to requested picrure and to picture <strong>of</strong> the requested size<br />
Point to letters in name<br />
\\'rite words from word iist<br />
Read rvords with picture<br />
Read word list<br />
Type name<br />
lV. Movemenh Used in the Written ond Verbol Exoression <strong>of</strong> Nutrilion<br />
Knowledge<br />
Write list <strong>of</strong> high-calorie food<br />
Say list <strong>of</strong> high-calorie food<br />
Circle high-calorie food choices<br />
<strong>Huntington's</strong> Diseos+-Worksheet for the Assessmenl <strong>of</strong> Moior Coordinoiion ond Hond Uscge<br />
Rerord the number 0f ilmes potient c0n reoch within o l5-second time period<br />
MovEMENTcY(LE Left<br />
Reoch (Gros Motor)<br />
Arm length +10'<br />
Right<br />
9" 6"<br />
P0int,.................><br />
3" 9" 6" 3"<br />
Arm length + 5'<br />
9"<br />
Touch ..................p<br />
6" 3' 9' 6" 3"<br />
(Fine Motor)<br />
srlt GRAsPs<br />
#l Hook<br />
(block ond whife gripper)<br />
#2 Cylindrirol<br />
(sponges-specify no.)<br />
#3 Lsterol<br />
(cllck+op pen or click toy<br />
olligotor)<br />
#4 Three Jow Chuck<br />
(spinner-pinwheel)<br />
#5 Pincer<br />
(clothespin)<br />
#6 Tip Pinch<br />
(pin or swob $ick wifi<br />
tension<br />
onend)<br />
Figure 2. A form tltat ma! be used in assessing coardination and hand usage amang patients aith Huntington\ disease. Based on the prici<br />
sion teaching method <strong>of</strong> monitoringfanuional performance (LIcGreny 1984; Pennyparher, Koenig, and LindslE 1972).<br />
Left<br />
Right<br />
Vol. 12 No.5 September/Oc rol:er 1992<br />
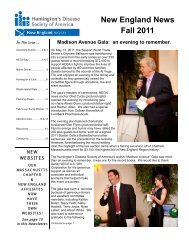
Tm gH
Purpose Assess Read-ng<br />
StartDate_<br />
Plonning Sheet<br />
Behavior Label Proiect # 1<br />
Cnmnrahen q j on StopDate<br />
Ir{anager Adviser<br />
Dole Situslion: Selfing<br />
npIYRFormol,<br />
fine<br />
One-to-one<br />
Quiet room<br />
Patient seated<br />
at table<br />
7 days<br />
Nlaterials:<br />
.Sample worksheet<br />
. Test Worksheet<br />
.2 pencils<br />
.Timer or watch<br />
rv/second hand<br />
.Standard Behavior<br />
Chart (Dailv)<br />
Events Before/Unlil/Dudng<br />
Day 1<br />
1) Give pacient a sanple worksheet,<br />
and explain how it is complered.<br />
2) Place test worksheet face dou'n<br />
on table.<br />
3) Directions to patient:<br />
. Read and answer questions<br />
by marking correct ones.<br />
. Skip arw questions,vou don t knorv.<br />
4) Flip paper.<br />
.5)Ask patient to "Go."<br />
6)Time for one minute.<br />
7),$k patient to "Stop."<br />
Days 2-7<br />
1) Revierv directions.<br />
2) Repear steps 2-7.<br />
Movemenl<br />
Cyrle(s)<br />
See/read<br />
and answer<br />
questions<br />
(by marking<br />
correct<br />
response).<br />
Evenls After<br />
Praise work.<br />
Correct<br />
worksheet<br />
rvith patient.<br />
Review skips<br />
and errors.<br />
Page #2<br />
Peformonce<br />
Slondord(s) AIM(S)<br />
8-13 items<br />
completed<br />
per minute<br />
@rh6<br />
mqt use tlt sfarm in assessing t/te cognitioe shilk <strong>of</strong> patfunts wth Hnttingtons disease. In t/tis exttmp/e,<br />
,"r'odirrg roorprehenii6n skilk arc to he tested. (Adapted aitlt permis.sion <strong>of</strong> Precision Teac/ing and Management Systems, Nar;ton, MA).<br />
ffirt<br />
To qssess le:ord the nunber <strong>of</strong> items lhe Gompleles pel minute,<br />
Coin Combin<strong>of</strong>ions<br />
1. nickel, penny<br />
2. dime, 2 per-rnies<br />
3. dime, nickel<br />
4. quarteq dime<br />
( ^r tartnr nPnn\/<br />
6. quarter, dime, nickel<br />
7. 2 dimes,3 nickels<br />
8 3quarters,2dimes<br />
9. 1 quaner,2 dimcs,<br />
3 nickels, 1 penny<br />
10.3 dimes, 4 pennies<br />
Bill (ombinotions<br />
1. 3 one dollar bills<br />
?.? fwe dollar bills<br />
and 1 one dollar bill<br />
3. 1 ten dollar bill,<br />
1 five dollar bill<br />
Pctienl ldentifies llen Costs {ou Poy with"<br />
$ 1.89<br />
ongwers.<br />
'{ou Gel Chonge Bock"<br />
; in assessing tlte paticnt's ability to use ntonqt-botlt in terms <strong>of</strong> functionalrnotor skills<br />
oid in trrr,t <strong>of</strong> ngitite ahilin-roitlt a ga/ <strong>of</strong> rtelpirtg t/rc poticnt renmin as independent as possible'<br />
b+.ti)<br />
Db. /J<br />
b /.95<br />
$11.64<br />
$18.65<br />
Items Cost<br />
4 for $1.00<br />
3 for $ .99<br />
5 for $1.00<br />
6 for $1.50<br />
3 for $1.00<br />
4 for $1.00<br />
5 for $1.00<br />
3 for $ .99<br />
$5.00 bill<br />
$1.00 bill<br />
$10.00 bill<br />
$10.00 bill<br />
$20.00 bill<br />
$20.00 bill<br />
$20.00 bill<br />
'{ou Wonf'<br />
I<br />
1<br />
1<br />
1<br />
I<br />
3<br />
2<br />
2<br />
'{ou Poy''<br />
Clinical N4anagement