STARK BASIC TRAINING - The American Health Lawyers Association
STARK BASIC TRAINING - The American Health Lawyers Association
STARK BASIC TRAINING - The American Health Lawyers Association

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>STARK</strong> <strong>BASIC</strong> <strong>TRAINING</strong><br />
<strong>Health</strong> Care Compliance <strong>Association</strong> and<br />
<strong>American</strong> <strong>Health</strong> <strong>Lawyers</strong> <strong>Association</strong><br />
Fraud & Compliance Forum<br />
September 30 – October 2, 2012<br />
Run for your<br />
life!!<br />
Joan P. Dailey. Esq.<br />
HHS Office of the General Counsel<br />
200 Independence Ave. S.W.<br />
Washington, D.C. 20201<br />
Telephone: 202-619-2794<br />
Email: joan.dailey@hhs.gov<br />
Robert A. Wade, Esq.<br />
Partner<br />
Krieg DeVault LLP<br />
4101 Edison Lakes Parkway, Suite 100<br />
Mishawaka, IN 46545<br />
Telephone: 574-485-2002<br />
Email: bwade@kdlegal.com 1<br />
OVERVIEW<br />
• Statutory and Regulatory Background<br />
• How to Analyze a Stark Issue<br />
• <strong>The</strong> Universal 3-Question Analysis<br />
• Key Elements of the Prohibition<br />
• Details on Key Exceptions<br />
• A Few Caveats<br />
2<br />
1
STATUTORY &<br />
REGULATORY<br />
BACKGROUND<br />
(<strong>The</strong> 30,000 foot view)<br />
3<br />
THE PROBLEM:<br />
FINANCIAL INCENTIVES TIED<br />
TO REFERRALS<br />
• Overutilization<br />
• Increased program costs<br />
• Corruption of medical decision-making<br />
• Systemic corruption<br />
4<br />
2
THE SOLUTION:<br />
MULTIPLE STATUTES<br />
• Anti-Kickback Statute (AKS)<br />
• Stark Statute<br />
• Prohibition against inducements to<br />
beneficiaries<br />
• State laws<br />
5<br />
THE PROHIBITION<br />
If a physician (or immediate family member)<br />
has a direct or indirect financial relationship<br />
with an entity that provides designated health<br />
services (“DHS”), the physician cannot refer<br />
the patient to the entity for DHS and the<br />
entity cannot submit a claim to CMS for such<br />
DHS, unless the financial relationship fits in<br />
an exception.<br />
6<br />
3
SANCTIONS<br />
• 1877(g)(1): Denial of claims<br />
• Intent is irrelevant<br />
• Recoupment<br />
• Obligation to make refund to CMS<br />
• New compromise authority (§6409 ACA)<br />
• 1877(g)(2): Refunds to beneficiary<br />
• Coinsurances<br />
• Deductible<br />
• Often an overlooked obligation<br />
7<br />
SANCTIONS<br />
• CMPs for knowing violations only<br />
• $15,000/DHS; $100,000 for circumvention<br />
schemes<br />
• Referring physicians can be liable<br />
• Potential False Claims Act liability<br />
• Requires intent to defraud<br />
8<br />
4
WHAT’S NOT PROHIBITED<br />
• Physicians can make some ancillary services<br />
available to patients<br />
• Physicians can own DHS entities if they<br />
don’t refer to them<br />
• Generally, physicians can get fair market<br />
value compensation for their services<br />
9<br />
THE MANY REGS…<br />
• Phase I: 66 FR 856 (2001)<br />
• Phase II: 69 FR 16054 (2004)<br />
• Phase III: 72 FR 51012 (2007)<br />
• EHR Exception: 71 FR 45140 (2006)<br />
• FY 2009 IPPS: 73 FR at 48688 (2008)<br />
• CY 2010 PFS: 74 FR at 61932 (2009)<br />
• ACA Changes (FR 11/24/10, 11/29/10,<br />
11/30/11)<br />
See handout for more… 10<br />
5
HOW TO ANALYZE<br />
A <strong>STARK</strong> ISSUE<br />
(Get out your crayons and eyeglasses)<br />
11<br />
BREAK IT DOWN<br />
• First, Draw a Diagram!<br />
• Ask Yourself Three Questions<br />
• Five Key Concepts<br />
• Read the Statute, Reg Text & Preambles<br />
• Remember a Few Caveats<br />
12<br />
6
THREE QUESTIONS<br />
1. Is there a referral from a physician for a<br />
designated health service? If so…<br />
2. Does the physician (or an immediate family<br />
member) have a financial relationship with the<br />
entity providing the DHS service? If so…<br />
3. Does the financial relationship fit in an<br />
exception?<br />
If not, there’s a violation<br />
13<br />
KEY CONCEPTS<br />
• Physician referrals<br />
• Designated health services (DHS)<br />
• Entity<br />
• Financial relationships<br />
• Exceptions<br />
14<br />
7
WHAT IS A<br />
“REFERRAL”?<br />
(You had to ask…)<br />
15<br />
WHAT IS A “REFERRAL”?<br />
• A request, order, plan of care, etc. –<br />
• For a DHS<br />
• For a service that includes a DHS<br />
• For consultation with another physician<br />
•Includes DHS ordered by consulting<br />
physician!<br />
• Written, oral, electronic<br />
16<br />
8
IMPUTED REFERRALS<br />
• Consulting physician’s referrals for DHS<br />
imputed to physician requesting consult<br />
• Referrals made by nonphysicians that are<br />
deemed to be made by the physician<br />
• Facts and circumstances test<br />
• Degree of control or influence exerted by<br />
physician on the nonphysician<br />
17<br />
WHAT IS A REFERRAL<br />
“TO AN ENTITY”?<br />
• Anything “reasonably intended” to result in<br />
patient receiving service from the entity<br />
• Need not be in writing or absolute<br />
• Directing/steering referrals<br />
• “Innocent entity exception” (411.353(e))<br />
• For indirect and oral referrals<br />
• Protects DHS entities that do not know identity<br />
of referring physician<br />
18<br />
9
WHAT IS NOT A<br />
“REFERRAL”?<br />
(Brace yourself for the irony…)<br />
19<br />
WHAT’S NOT A REFERRAL<br />
• Personally performed services<br />
• “<strong>The</strong> work of your own two hands”<br />
• Excludes “incident to” services<br />
• Excludes corresponding TC of hospital<br />
service<br />
20<br />
10
WHAT’S NOT A REFERRAL<br />
• Requests made by pathologists, radiologists,<br />
and radiation oncologists<br />
• Pursuant to a consultation<br />
• For their own services (see defn)<br />
• Furnished by them or under their<br />
supervision (or by/under supervision of<br />
physician in same group and of same<br />
specialty)<br />
21<br />
“REFERRING PHYSICIAN”<br />
• A “physician” who makes a referral<br />
• 1861(r) definition of physician applies<br />
• Does not include physician extenders or<br />
other nonphysicians<br />
• But see discussion of imputed referrals<br />
22<br />
11
TIPS:<br />
• Can have multiple referring physicians for<br />
the same DHS<br />
• Do a separate 3-Question Analysis for each<br />
physician’s referrals<br />
23<br />
• 1877(h)(5)<br />
• 411.351 Definitions<br />
RESOURCES<br />
• “Physician”<br />
• “Referral”<br />
• “Referring Physician”<br />
• Phase I Preamble (2001), pp. 871-75<br />
• Phase II Preamble (2004), pp. 16063-66<br />
• Phase III Preamble (2007), pp. 51019-21<br />
24<br />
12
DESIGNATED<br />
HEALTH SERVICES<br />
(Not everything about Stark is<br />
complicated ….)<br />
25<br />
DHS<br />
• Clinical laboratory*<br />
• Physical therapy*<br />
• Occupational therapy*<br />
• Speech-language pathology*<br />
• Radiology and other imaging services*<br />
• Radiation therapy services and supplies*<br />
* Defined by CPT/HCPCS code<br />
26<br />
13
• DMEPOS<br />
DHS<br />
• Parenteral and enteral nutrients, equipment,<br />
and supplies<br />
• Prosthetics, orthotics, and prosthetic devices<br />
and supplies<br />
• Home health services<br />
• Outpatient prescription drugs<br />
• Inpatient and outpatient hospital services<br />
• except lithotripsy!<br />
27<br />
GENERAL RULES<br />
• Code List is determinative<br />
• DHS bundled into a composite rate payment<br />
is not DHS<br />
• Exception: If the service package itself is listed<br />
in the statute as a DHS (e.g., inpatient hospital<br />
services)<br />
• DHS paid as stand-alone service is DHS<br />
• New Exception (eff. 1/1/08): radiology and<br />
drugs furnished in an ASC that qualify as<br />
“covered ancillary services” per 416.164(b).<br />
28<br />
14
RESOURCES<br />
• 1877(h)(6); 411.351<br />
• Phase I (pp. 922-42)<br />
• Phase II (pp. 16099-16106)<br />
• Nuclear medicine, 70 FR at 70283 (11/21/05)<br />
• CY08 OPPS Final Rule, 72 FR 66851<br />
(11/27/07)<br />
• Revising defns of DHS, outpatient Rxn drugs,<br />
radiology<br />
• PFS CPT/HCPCS Code List Updates<br />
29<br />
ENTITY<br />
(So many entities, so little time…)<br />
30<br />
15
• Old Rule<br />
ENTITY<br />
• Person or entity to whom payment is made<br />
• New Rule (effective 10/1/09)<br />
• Person who presents claim to Medicare, AND<br />
• Person who has “performed services billed as<br />
DHS”<br />
31<br />
ENTITY<br />
• No regulatory definition of what it means to<br />
“perform” services billed as DHS<br />
• See preamble commentary …<br />
• Does physician “do the medical work” for the<br />
service and could she bill for it?<br />
• Entity does not “perform” DHS if it only:<br />
• Leases or sells space/equipment<br />
• Furnishes supplies<br />
• Provides management or billing services; or<br />
• Provides personnel<br />
32<br />
16
ENTITY<br />
• Multiple DHS entities can receive a referral<br />
• Must do separate Stark analysis for referrals to<br />
each DHS entity<br />
• Expanded definition effectively prohibits<br />
physician ownership of entities that perform<br />
DHS “under arrangements” with a hospital<br />
33<br />
RESOURCES<br />
• 411.351 definition<br />
• Phase I (p.943)<br />
• Phase II (pp. 16106-07)<br />
• Phase III (pp. 51014-15)<br />
• CY09 IPPS (73 FR 48721-33) for current law<br />
34<br />
17
Financial<br />
Relationships<br />
(Follow the money .…)<br />
35<br />
FINANCIAL RELATIONSHIP<br />
• Ownership/Investment<br />
• Compensation<br />
• Direct or Indirect<br />
• Statute is implicated even if relationship<br />
is not about the provision of DHS!<br />
36<br />
18
DIRECT<br />
DOCTOR<br />
DHS ENTITY<br />
(No intervening entities)<br />
37<br />
INDIRECT<br />
DOCTOR COMPANY DHS ENTITY<br />
(One or more intervening entities)<br />
38<br />
19
INDIRECT OWNERSHIP<br />
• All links in chain are ownership<br />
• If the links are a mix of ownership and<br />
compensation, it may be an indirect<br />
compensation arrangement.<br />
• DHS entity knows or should know that the<br />
physician has some ownership interest in it.<br />
• No affirmative obligation to inquire<br />
• Duty of reasonable inquiry<br />
39<br />
INDIRECT COMPENSATION<br />
ARRANGEMENTS (ICAs)<br />
• Definition (411.354(c))<br />
• Unbroken chain of 3+ persons/entities;<br />
• Aggregate compensation to physician varies<br />
with or takes into account referrals or other<br />
business for DHS entity; and<br />
• DHS entity knows or should know nature of<br />
physician’s compensation<br />
• Stark not applicable to ICAs that fail to meet<br />
definition<br />
40<br />
20
ICA EXCEPTION<br />
• Compensation must be FMV not taking into<br />
account referrals or other business generated<br />
• Does not look to aggregate compensation<br />
• Apply special compensation rules at<br />
411.354(d)(2),(3) regarding per unit comp<br />
• Other requirements (e.g., in writing)<br />
41<br />
SPECIAL RULES ON<br />
COMPENSATION<br />
• Unit-based comp does not TIA “v/v of referrals” if<br />
per unit payment is FMV and does not vary during<br />
the term in a manner that TIA referrals of DHS.<br />
• Example of varying: $10/item for first 100 items;<br />
$8/item thereafter<br />
• Unit-based comp does not TIA “OBG btw the<br />
parties” if FMV and does not vary during the term<br />
in manner that TIA referrals or OBG, including<br />
private pay business<br />
42<br />
21
THE METHOD BEHIND<br />
THE MADNESS<br />
• ICA definition includes potentially abusive<br />
relationships<br />
• Focus is on aggregate comp<br />
• Per unit comp rules not applied at definition stage<br />
• Captures both fixed and variable comp that reflects<br />
referrals<br />
• Knowledge standard solves liability problem for<br />
nonabusive remote relationships<br />
43<br />
THE METHOD BEHIND<br />
THE MADNESS<br />
• ICA exception immunizes ICAs that are not<br />
actually abusive.<br />
• Focus is on individual, unaggregated payments;<br />
per unit comp rules apply<br />
• Exception will not immunize fixed (flat fee)<br />
compensation that is not FMV<br />
44<br />
22
“STAND IN THE SHOES”<br />
Physician<br />
Owners<br />
(aka, when an unbroken<br />
chain of 3 is a direct comp<br />
arrangement)<br />
DHS ENTITY<br />
Physician<br />
Group<br />
45<br />
“STAND IN THE SHOES”<br />
• Current Rule (since 10/1/08):<br />
• Physician SITS of his physician organization<br />
(PO) if he has an ownership/investment interest<br />
in the PO<br />
• Non-owners and titular owners may elect to<br />
SITS<br />
• Old Rule: All physicians SITS of their PO<br />
• Really Old Rule: Nobody SITS at all<br />
46<br />
23
THE “NEW” DIRECT<br />
COMPENSATION<br />
Group<br />
Physician<br />
Owners<br />
47<br />
INDIRECT<br />
BUT -- No change if intervening entity<br />
owned by physician is not a PO:<br />
DOCTOR COMPANY DHS ENTITY<br />
48<br />
24
RESOURCES<br />
• 1877(a)(2), (h)(1)<br />
• 411.354<br />
• Phase I (pp. 864-870)<br />
• Phase II (pp. 16057-63)<br />
• Phase III (pp. 51026-31)<br />
• CY09 IPPS (pp. 48690-700)<br />
49<br />
EXCEPTIONS<br />
(<strong>The</strong> devil is in the details ….)<br />
50<br />
25
EXCEPTIONS<br />
• “Close enough” doesn’t work<br />
• Three categories<br />
• Ownership only<br />
• Ownership and compensation<br />
(“service based”)<br />
• Compensation only<br />
51<br />
OWNERSHIP EXCEPTIONS<br />
• Rural providers<br />
• “Whole” hospitals<br />
• Puerto Rico hospitals<br />
• Mutual funds and public securities<br />
52<br />
26
“SERVICE-BASED”<br />
EXCEPTIONS<br />
• Physician Services<br />
• In-Office Ancillary Services<br />
• Supervision, location & billing requirements<br />
• Academic Medical Centers (AMCs)<br />
• Prepaid plans (managed care services)<br />
• Intra-family rural referrals<br />
• Others<br />
53<br />
• Many exceptions<br />
COMPENSATION<br />
EXCEPTIONS<br />
• Fair market value is key<br />
• Multiple exceptions may apply<br />
• In general, provider can choose which of<br />
several potentially applicable exceptions to<br />
satisfy (the “any exception will do” rule)<br />
54<br />
27
FAIR MARKET VALUE<br />
• Value in arm’s length transaction, result of<br />
bona fide bargaining between parties not in<br />
a position to refer to one another<br />
• Special rules for rental property<br />
• Value for general commercial purposes, not<br />
taking into account intended use<br />
• Not adjusted to reflect proximity to physician<br />
lessor<br />
• See definition at §411.351.<br />
55<br />
FAIR MARKET VALUE<br />
• Documentation<br />
• Use of appraisals prudent, but not mandated<br />
• Any appropriate commercially reasonable<br />
methodology<br />
• Ultimately, a facts and circumstances test<br />
• Nature of transaction<br />
• Location<br />
• Other factors<br />
56<br />
28
FMV RESOURCES<br />
• Phase I (pp. 944-45)<br />
• Phase II (p. 16107)<br />
• Phase III (pp. 51015-16)<br />
• Not advisory opinions!<br />
57<br />
COMPENSATION<br />
EXCEPTIONS<br />
• Rentals of space & equipment<br />
• Personal services arrangements, employment<br />
• Employment<br />
• Non-monetary compensation (within limits)<br />
• Medical staff incidental benefits<br />
• Recruitment and retention<br />
• Indirect compensation arrangements<br />
• Fair market value<br />
• Electronic health records donations<br />
• More<br />
58<br />
29
In-Office Ancillary<br />
Services Exception<br />
(A wide, well-worn path out of the<br />
Stark woods….)<br />
59<br />
OVERVIEW<br />
• For provision of DHS when truly ancillary to<br />
office practice of medicine<br />
• Definition of “group practice” is key<br />
• Fully integrated, not a loose confederation of<br />
physicians designed to profit from DHS<br />
referrals<br />
• Financial incentives to make DHS referrals are<br />
attenuated<br />
60<br />
30
GROUP PRACTICE CRITERIA<br />
• Group practice means a single group of two<br />
or more physicians legally organized as a<br />
partnership, professional corporation,<br />
faculty practice plan or similar association<br />
where<br />
• Each physician member provides substantially<br />
the full range of services that physician routinely<br />
provides (including medical care, consultation,<br />
diagnosis or treatment)<br />
• Professional services provided through joint use<br />
of shared office space, facilities, equipment and<br />
personnel<br />
61<br />
GROUP PRACTICE CRITERIA<br />
• Substantially all (75%+) of each physician<br />
member’s patient care services are --<br />
• Provided through group<br />
• Document through time cards, personal schedules, etc.;<br />
• Must meet within 12 months of formation or 12 months<br />
of new physician relocating (25 miles+) to join group.<br />
• Billed under group’s billing number<br />
• All income is treated as receipts of group<br />
• Overhead expenses and income from<br />
practice are distributed in accordance with<br />
previously determined methods<br />
62<br />
31
Member of Group Practice v.<br />
Physician in Group Practice<br />
• Independent Contractors are “Physicians in<br />
Group Practice” but not “Members of Group<br />
Practice”<br />
• Issues:<br />
• Range of Care—Members only<br />
• 75% Test—Members only<br />
• Productivity Bonuses and Profit-Share—All,<br />
including Independent Contractors<br />
63<br />
GROUP PRACTICE CRITERIA<br />
• No physician in group may directly or<br />
indirectly receive compensation based on<br />
volume or value of referrals by physician.<br />
• Exception: Group physicians may be paid<br />
share of overall profits or productivity bonus<br />
(for personally performed or “incident to”<br />
services) if not directly related to DHS<br />
referrals.<br />
64<br />
32
GROUP PRACTICE CRITERIA<br />
• Share of profits will not be directly related to<br />
volume or value of referrals if one of the<br />
following conditions is met:<br />
• Profits divided per capita (i.e., equal share per<br />
physician in group);<br />
• DHS revenues are distributed in the same manner<br />
as non-DHS revenues from any federal health care<br />
program or private payor; or<br />
• DHS revenues for group practice is less than 5% of<br />
group practices’ total revenue and those revenues<br />
allocated to each physician in the group is 5% or<br />
less of each physician’s total compensation from the<br />
group<br />
65<br />
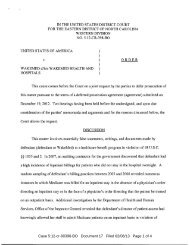
GROUP PRACTICE CRITERIA<br />
Permitted:<br />
Patient<br />
$<br />
GROUP PRACTICE<br />
DHS $ Pooled<br />
%of $<br />
%of $<br />
%of $<br />
DR.<br />
DR.<br />
DR.<br />
Distribution of Profit from DHS<br />
Should Reflect Pooling<br />
66<br />
33
GROUP PRACTICE CRITERIA<br />
Group Practice<br />
Pt.<br />
Pt.<br />
Pt.<br />
Pt.<br />
Pt.<br />
Pt.<br />
Pt.<br />
Pt.<br />
Pt.<br />
Dr.<br />
Dr.<br />
2<br />
Dr.<br />
Can Pool Profits from DHS Into Components If Each Component<br />
Has at Least 5 Physicians<br />
3<br />
Dr.<br />
Dr.<br />
Dr.<br />
Dr.<br />
Dr.<br />
Dr.<br />
Dr.<br />
Dr.<br />
Dr.<br />
Dr.<br />
Dr.<br />
Dr.<br />
Dr.<br />
Dr.<br />
Dr.<br />
67<br />
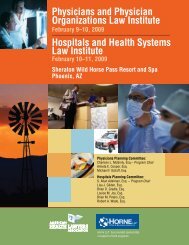
GROUP PRACTICE CRITERIA<br />
Not Permitted:<br />
PATIENT<br />
PATIENT<br />
PATIENT<br />
$<br />
$<br />
$<br />
GROUP PRACTICE<br />
$<br />
$<br />
$<br />
DR.<br />
DR.<br />
DR.<br />
$ Passes Through<br />
Group Practice Cannot Be Used To Pay<br />
Physician Directly for DHS Ordered<br />
68<br />
34
69<br />
IN-OFFICE ANCILLARY<br />
SERVICES EXCEPTION<br />
Must answer 3<br />
questions:<br />
Who?<br />
How?<br />
Where?<br />
70<br />
35
IOAS EXCEPTION<br />
Who May Provide Services?<br />
• Referring physician;<br />
• Physician who is member of same group practice<br />
as referring physician;<br />
• Individuals who are directly supervised by<br />
physician or another physician in same group<br />
practice; and<br />
• Physicians in the group practice such as<br />
employees and independent contractors of group<br />
practice<br />
71<br />
IOAS EXCEPTION<br />
Where Are Services Provided?<br />
Same building<br />
or<br />
Centralized building<br />
72<br />
36
IOAS EXCEPTION<br />
Where Are Services Provided?<br />
• “Same Building” where referring physician<br />
(or others in group) furnish services<br />
unrelated to the furnishing of DHS<br />
• Building must have a single street address<br />
assigned by the U.S. Postal Service, not<br />
including interior loading docks, mobile<br />
vehicles, vans or trailers<br />
• Must meet one of three tests<br />
73<br />
IOAS EXCEPTION<br />
Same Building Tests<br />
• 1) Office is open to the group’s patients for medical services at least 35<br />
hours per week and a member of the group provides physician services<br />
(including non-DHS services) to patients at least 30 hours per week<br />
• 2) Referring physician’s group owns or rents an office that is normally<br />
open to patients for medical services at least 8 hours per week and<br />
referring physician provides physician services (include non-DHS<br />
services) to patients at this office at least 6 hours per week<br />
• 3) Referring physician’s group owns or rents an office that is normally<br />
open to patients for medical services at least 8 hours per week, either<br />
referring physician orders DHS services while seeing the patient on the<br />
premises or a member of referring physician’s group practice is on<br />
premises when DHS is performed and referring physician or member<br />
of group practices at site at least 6 hours per week<br />
74<br />
37
IOAS EXCEPTION<br />
Where Are Services Provided?<br />
A Centralized Building, which means<br />
all or part of a building that is owned<br />
or leased on a full-time basis by a<br />
group practice including a mobile<br />
vehicle, van or trailer where some or<br />
all of the group practices DHS is<br />
provided<br />
75<br />
IOAS EXCEPTION<br />
Not Covered by Exception<br />
Given to Patient in<br />
Physician’s Office But<br />
Intended To Be Used at<br />
home or outside<br />
Physician’s Office<br />
76<br />
38
IOAS EXCEPTION<br />
How Are Services Billed?<br />
• By physician performing or supervising services<br />
• By group practice of which such physician is<br />
member, employee or independent contractor<br />
under billing number assigned to group practice;<br />
or<br />
• By entity that is wholly owned by such physician or<br />
such group practice<br />
77<br />
IOAS EXCEPTION<br />
DME<br />
• How is equipment used by patient?<br />
• Durable medical equipment (“DME”), like<br />
canes, crutches, walkers, blood glucose monitors,<br />
can be subject to in-office ancillary exception if:<br />
• the DME is required by the patient to depart from the<br />
physician’s office, or is a blood glucose monitor<br />
• it is furnished in the same building as the patientphysician<br />
encounter; and<br />
• the DME is furnished personally by the physician, a<br />
physician in the same group practice, or an employee of<br />
the same group practice<br />
78<br />
39
IOAS EXCEPTION<br />
Notification Requirements<br />
• Applies only to MRI, CT and PET<br />
• CMS has not extended to any other radiology<br />
services under PPACA specific authority<br />
• Notice of 5 other suppliers of service<br />
• Physician groups need not identify hospital<br />
competitors<br />
• Applies to services furnished on or after<br />
January 1, 2011<br />
79<br />
Recruitment Exception<br />
(It’s so nice to be wanted so<br />
badly…)<br />
80<br />
40
RECRUITMENT<br />
• Payments made to induce physician to<br />
relocate to “geographic area served by<br />
hospital” (zip code test)<br />
• Not conditioned on referrals<br />
• Compensation not determined based on v/v<br />
actual or anticipated referrals or OBG<br />
• Recruit allowed to establish privileges at and<br />
refer to other entities<br />
81<br />
RECRUITMENT<br />
• Relocation of medical practice<br />
• Moving at least 25 miles into geographic area<br />
• Deriving >75% of revenues from new patients<br />
compared to previous 3 years<br />
• Relocation requirement waived for<br />
• Residents, physicians practicing
RECRUITMENT<br />
Additional criteria for physician recruitment<br />
into group practice:<br />
• Except for actual costs incurred by group,<br />
remuneration is passed directly to recruit<br />
• Income guarantee: costs allocated to recruit do not<br />
exceed actual additional incremental costs for that<br />
physician<br />
• Group can’t unreasonably restrict recruit’s ability to<br />
practice in the hospital’s geographic area<br />
83<br />
Personal Service<br />
Arrangements<br />
Exception<br />
(When impersonal service just<br />
won’t do…)<br />
84<br />
42
PSA EXCEPTION<br />
• Arrangement is set out in writing, signed by<br />
parties and specifies services covered by<br />
arrangement<br />
• Arrangement covers all services to be provided<br />
by physician to entity<br />
• References all other arrangements; or<br />
• References master list of contracts that is<br />
maintained with historical record of all<br />
arrangements<br />
• Term for at least one year<br />
85<br />
PSA EXCEPTION<br />
• Services are reasonable and necessary<br />
• Compensation to be paid over term of<br />
arrangement is set in advance, does not<br />
exceed FMV, and is not determined in<br />
manner which takes into account volume or<br />
value of referrals between parties<br />
86<br />
43
PSA EXCEPTION<br />
• Hold over month-to-month following a term<br />
of at least one year, assuming all other<br />
provisions of the exception are met,<br />
continuing on a month-to-month basis for<br />
up to 6 months as long as the terms during<br />
the hold over period are fair market value<br />
will meet the personal service arrangement<br />
exception<br />
87<br />
Rental Exceptions<br />
(When lease is more…)<br />
88<br />
44
RENTAL EXCEPTIONS<br />
• Lease is in writing, signed, and specifies<br />
premises and equipment to be leased<br />
• Space and equipment rented does not<br />
exceed that which is reasonable and<br />
necessary and is used exclusively by lessee<br />
when being leased by lessee<br />
• Term of lease is for at least one year<br />
• Commercially reasonable<br />
89<br />
RENTAL EXCEPTIONS<br />
• Rental charges are set in advance, fair<br />
market value, and not determined in a<br />
manner that takes into account volume or<br />
value of referrals or other business generated<br />
between parties<br />
• No “per click” if physician/owner is source of<br />
referral<br />
• No charges on percentage of revenue<br />
• Remember special FMV definition<br />
90<br />
45
RENTAL EXCEPTIONS<br />
• Hold over month-to-month following a term<br />
of at least one year, assuming all other<br />
provisions of the exception are met,<br />
continuing on a month-to-month basis for<br />
up to 6 months as long as the terms during<br />
the hold over period are fair market value<br />
will meet the rental of office space and<br />
equipment exceptions<br />
91<br />
Employment<br />
Exception<br />
(Becoming more and more<br />
popular…)<br />
92<br />
46
EMPLOYMENT EXCEPTION<br />
• Employment is for identifiable services<br />
• Compensation is:<br />
• Fair market value;<br />
• Not determined in manner which takes into<br />
account volume or value of referrals; and<br />
• Commercially reasonable even if no referrals<br />
were made to employer<br />
93<br />
EMPLOYMENT EXCEPTION<br />
• Productivity bonuses can be paid if based on<br />
services performed personally by the<br />
physician (i.e., worked RVUs)<br />
94<br />
47
EMPLOYMENT EXCEPTION<br />
Required Referrals (411.354(d)(4))<br />
Employer can require employee to refer to a<br />
particular provider, practitioner or supplier if:<br />
• Referral requirement is in writing, signed<br />
• Compensation is set in advance & FMV<br />
• Referral requirement not applicable if:<br />
• Patient expresses a contrary preference<br />
• Provider not covered by patient’s insurance<br />
• Not in the patient’s best medical interest …<br />
95<br />
EMPLOYMENT EXCEPTION<br />
Required Referrals<br />
• <strong>The</strong> required referrals must relate solely to the<br />
physician’s services covered by the scope of the<br />
employment and be reasonably necessary for<br />
the legitimate business purposes of the<br />
arrangement<br />
Good:<br />
Primary Care –<br />
Inpatient<br />
Bad:<br />
Medical Director –<br />
Inpatient<br />
96<br />
48
Non-Monetary<br />
Compensation Exception<br />
(Because sometimes a physician<br />
needs a gift basket…)<br />
97<br />
NON-MONETARY<br />
COMPENSATION EXCEPTION<br />
• Compensation, not including cash or cash<br />
equivalents (i.e., gift certificates), up to an<br />
aggregate of $373 per year per physician as<br />
long as:<br />
• Benefit is not determined based upon volume or<br />
value of referrals<br />
• Benefit is not solicited by physician or anyone<br />
affiliated with their practice<br />
• Maximum cannot be aggregated to make a<br />
larger gift to a group<br />
98<br />
49
NON-MONETARY<br />
COMPENSATION EXCEPTION<br />
• <strong>The</strong> current $373 limit is updated annually.<br />
• For updates, see<br />
www.cms.hhs.gov/PhysicianSelfReferral/<br />
99<br />
NON-MONETARY<br />
COMPENSATION EXCEPTION<br />
• If a hospital inadvertently exceeds the annual limit,<br />
the hospital will still be deemed to be in<br />
compliance if (i) the value of the excess is no more<br />
than 50% of the limit, and (ii) the physician returns<br />
the excess by the end of the calendar year or within<br />
180 consecutive calendar days, whichever is earlier<br />
• NOTE: Can only be used once every 3 years<br />
• Hospitals can hold 1 formal medical staff event per<br />
year without including the cost in this exception<br />
100<br />
50
NON-MONETARY<br />
COMPENSATION EXCEPTION<br />
• For example:<br />
• Cannot give $1,000 oil painting to 5 physician<br />
group and allocate $200 to each physician<br />
101<br />
NON-MONETARY<br />
COMPENSATION EXCEPTION<br />
• Preamble, on Page 16112 of Phase II, stated<br />
that “[the Medical Staff Incidental Benefits<br />
Exception] was not intended to cover the<br />
provision of tangential, off-site benefits,<br />
such as restaurant dinners or theater tickets,<br />
which must comply with the exception for<br />
non-monetary compensation<br />
up to $300.” (emphasis added)<br />
102<br />
51
Medical Staff<br />
Incidental Benefits<br />
(Because doctors can’t make<br />
rounds without lab coats and<br />
donuts …)<br />
103<br />
MEDICAL STAFF INCIDENTAL<br />
BENEFITS EXCEPTION<br />
• Items or services used on the hospital's<br />
campus may be given to members of its<br />
medical staff if:<br />
• Provided to all members in the same specialty<br />
without regard to volume or value of referrals<br />
• Provided only during periods when the medical<br />
staff members are making rounds or involved in<br />
other services that benefit the hospital and its<br />
patients<br />
104<br />
52
MEDICAL STAFF INCIDENTAL<br />
BENEFITS EXCEPTION<br />
• <strong>The</strong> item or service is reasonably related to<br />
the delivery of medical services at the<br />
hospital<br />
• Each item or service is less than $31 per<br />
benefit (updated annually)<br />
Free For<br />
Physicians<br />
105<br />
MEDICAL STAFF INCIDENTAL<br />
BENEFITS EXCEPTION<br />
• Protects internet access, pagers, or two-way<br />
radios, used away from the campus only to<br />
access hospital medical records/info or to<br />
access patients or personnel who are on the<br />
hospital campus<br />
• Protects identification of the<br />
medical staff on a hospital<br />
website or in hospital<br />
advertising<br />
106<br />
53
WHAT IF NO EXCEPTION<br />
APPLIES?<br />
• Consider exceptions for temporary<br />
noncompliance (§411.353(f), (g))<br />
• Disclose to CMS<br />
• Voluntary Refund to CMS payment contractor<br />
• Stark Self-Referral Disclosure Protocol – permits<br />
compromise<br />
Provider Bankruptcy<br />
Prevention Hotline:<br />
1-800-CMS-SRDP<br />
• Disclose to OIG or AUSA<br />
107<br />
SUMMARY<br />
(Yes, Virginia, there IS light at the<br />
end of the tunnel…)<br />
108<br />
54
TIPS<br />
• Always draw a diagram<br />
• Always ask the 3 Questions<br />
• Always reread the applicable definitions and<br />
preambles of all the various rules<br />
• Never rely on your memory!<br />
• Two heads are better than one<br />
109<br />
A FEW CAVEATS<br />
• Analyze relationships under the law that<br />
existed at the relevant time<br />
• Revisions can make the difference between<br />
compliance and noncompliance<br />
• E.g., ACA change to IOAS exception; SITS<br />
& entity definition reg changes<br />
• Stark compliant relationships can still<br />
violate AKS<br />
110<br />
55
111<br />
56