

Tier 2 cover - Health Plan of Nevada
Tier 2 cover - Health Plan of Nevada
Tier 2 cover - Health Plan of Nevada

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
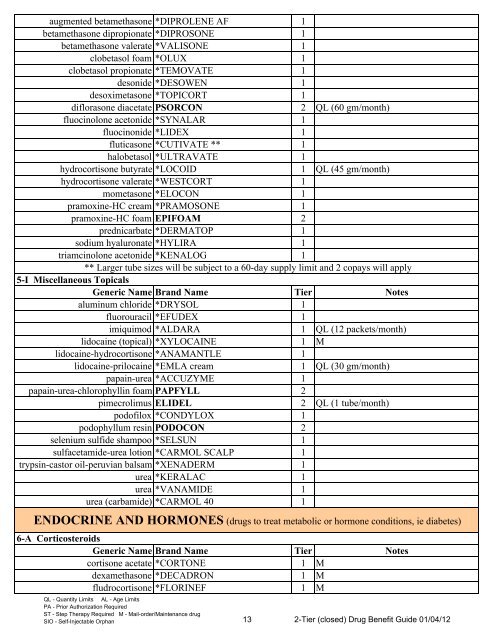
augmented betamethasone *DIPROLENE AF 1<br />
betamethasone dipropionate *DIPROSONE 1<br />
betamethasone valerate *VALISONE 1<br />
clobetasol foam *OLUX 1<br />
clobetasol propionate *TEMOVATE 1<br />
desonide *DESOWEN 1<br />
desoximetasone *TOPICORT 1<br />
diflorasone diacetate PSORCON 2 QL (60 gm/month)<br />
fluocinolone acetonide *SYNALAR 1<br />
fluocinonide *LIDEX 1<br />
fluticasone *CUTIVATE ** 1<br />
halobetasol *ULTRAVATE 1<br />
hydrocortisone butyrate *LOCOID 1 QL (45 gm/month)<br />
hydrocortisone valerate *WESTCORT 1<br />
mometasone *ELOCON 1<br />
pramoxine-HC cream *PRAMOSONE 1<br />
pramoxine-HC foam EPIFOAM 2<br />
prednicarbate *DERMATOP 1<br />
sodium hyaluronate *HYLIRA 1<br />
triamcinolone acetonide *KENALOG 1<br />
** Larger tube sizes will be subject to a 60-day supply limit and 2 copays will apply<br />
5-I Miscellaneous Topicals<br />
Generic Name Brand Name<br />
<strong>Tier</strong><br />
Notes<br />
aluminum chloride *DRYSOL 1<br />
fluorouracil *EFUDEX 1<br />
imiquimod *ALDARA 1 QL (12 packets/month)<br />
lidocaine (topical) *XYLOCAINE 1 M<br />
lidocaine-hydrocortisone *ANAMANTLE 1<br />
lidocaine-prilocaine *EMLA cream 1 QL (30 gm/month)<br />
papain-urea *ACCUZYME 1<br />
papain-urea-chlorophyllin foam PAPFYLL 2<br />
pimecrolimus ELIDEL 2 QL (1 tube/month)<br />
pod<strong>of</strong>ilox *CONDYLOX 1<br />
podophyllum resin PODOCON 2<br />
selenium sulfide shampoo *SELSUN 1<br />
sulfacetamide-urea lotion *CARMOL SCALP 1<br />
trypsin-castor oil-peruvian balsam *XENADERM 1<br />
urea *KERALAC 1<br />
urea *VANAMIDE 1<br />
urea (carbamide) *CARMOL 40 1<br />
ENDOCRINE AND HORMONES (drugs to treat metabolic or hormone conditions, ie diabetes)<br />
6-A Corticosteroids<br />
Generic Name Brand Name<br />
<strong>Tier</strong><br />
cortisone acetate *CORTONE 1<br />
dexamethasone *DECADRON 1<br />
fludrocortisone *FLORINEF 1<br />
QL - Quantity Limits<br />
AL - Age Limits<br />
M<br />
M<br />
M<br />
Notes<br />
PA - Prior Authorization Required<br />
ST - Step Therapy Required M - Mail-order/Maintenance drug<br />
SIO - Self-Injectable Orphan 13 2-<strong>Tier</strong> (closed) Drug Benefit Guide 01/04/12














