Quality Use of Medicines for Cardiovascular Health - National Heart ...
Quality Use of Medicines for Cardiovascular Health - National Heart ...
Quality Use of Medicines for Cardiovascular Health - National Heart ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Quality</strong> <strong>Use</strong> <strong>of</strong> <strong>Medicines</strong> <strong>for</strong><br />
<strong>Cardiovascular</strong> <strong>Health</strong><br />
QUM<br />
Executive Summary<br />
An initiative <strong>of</strong> the <strong>Heart</strong> Foundation Pharmaceutical Roundtable<br />
Rob Wiseman, Anne-Marie Scully, Hayley Caspers red 3 – 2006<br />
QUM
This project was supported by the following members <strong>of</strong> the Pharmaceutical Roundtable:<br />
© 2006 <strong>National</strong> <strong>Heart</strong> Foundation <strong>of</strong> Australia. All rights reserved.<br />
This is an executive summary <strong>of</strong> the <strong>Quality</strong> use <strong>of</strong> medicines in cardiovascular health report. The<br />
report is available at www.heartfoundation.org.au<br />
This report builds on research reported in: Wiseman R and White S (2005) Views <strong>of</strong> <strong>Quality</strong><br />
<strong>Use</strong> <strong>of</strong> <strong>Medicines</strong>: Stakeholders perceptions <strong>of</strong> their needs, values and responsibilities, and the<br />
opportunities and barriers <strong>for</strong> QUM. Sydney: The Pharmaceutical Alliance.<br />
This is available from: www.pharmalliance.com.au/files/QUM_2005_Report.pdf<br />
<strong>National</strong> <strong>Heart</strong> Foundation <strong>of</strong> Australia (The <strong>Heart</strong> Foundation Pharmaceutical Roundtable)<br />
The views expressed in this report are those <strong>of</strong> the authors and not necessarily those <strong>of</strong> the <strong>Heart</strong><br />
Foundation Pharmaceutical Roundtable or its partner organisations: the <strong>National</strong> <strong>Heart</strong> Foundation<br />
<strong>of</strong> Australia, Alphapharm, Astrazeneca, Bristol-Myer Squibb, Merck Sharp & Dohme, Pfizer<br />
Australia, Roche, san<strong>of</strong>i-aventis, Solvay Pharmaceuticals and Servier Laboratories.<br />
This work is copyright. No part may be reproduced in any <strong>for</strong>m or language without prior written<br />
permission from the <strong>National</strong> <strong>Heart</strong> Foundation <strong>of</strong> Australia (national <strong>of</strong>fice). Enquiries concerning<br />
permissions should be directed to copyright@heartfoundation.org.au<br />
Suggested citation: <strong>National</strong> <strong>Heart</strong> Foundation <strong>of</strong> Australia (Wiseman R, Scully, AM and Caspers<br />
H on behalf <strong>of</strong> the <strong>Heart</strong> Foundation Pharmaceutical Roundtable). <strong>Quality</strong> <strong>Use</strong> <strong>of</strong> <strong>Medicines</strong> in<br />
cardiovascular health (executive summary). West Melbourne, Victoria, 2006.<br />
<strong>National</strong> Library <strong>of</strong> Australia Cataloguing-in-Publication data<br />
Wiseman, Rob, 1969– . <strong>Quality</strong> <strong>Use</strong> <strong>of</strong> Medicine in cardiovascular health (executive summary).<br />
Print: ISBN-10: 1-921226-07-2 ISBN-13: 978-1-921226-07-6<br />
1. <strong>Cardiovascular</strong> agents—Australia. 2. <strong>Cardiovascular</strong> diseases—Australia—Treatment.<br />
3. Pharmaceutical policy—Australia. I. Scully, Anne-Marie. II. Caspers, Hayley. III. Title.<br />
615.71<br />
[ 2 ]
Contents<br />
Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2<br />
The <strong>Heart</strong> Foundation Pharmaceutical Roundtable . . . . . . . . . . . . . . . . . . . . . . . 2<br />
About the project . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2<br />
<strong>Cardiovascular</strong> disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3<br />
<strong>Medicines</strong> and CVD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3<br />
<strong>Quality</strong> <strong>Use</strong> <strong>of</strong> <strong>Medicines</strong>. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3<br />
Contents<br />
Stages <strong>of</strong> <strong>Quality</strong> <strong>Use</strong> <strong>of</strong> <strong>Medicines</strong> in <strong>Cardiovascular</strong> <strong>Health</strong>. . . . . . . . . . . . . . . . . . . . . . 4<br />
Be<strong>for</strong>e a cardiovascular event. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5<br />
Identifying people at risk <strong>of</strong> CVD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5<br />
Encouraging consumers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5<br />
Enabling General Practitioners . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5<br />
Initiating medicines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6<br />
Counselling and education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6<br />
– Consumer medicine in<strong>for</strong>mation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6<br />
Adherence in the longer term . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7<br />
– Home medicine reviews . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7<br />
During a cardiovascular event . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8<br />
Getting people to hospital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8<br />
Admission to hospital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8<br />
Engaging specialist physicians . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8<br />
After a cardiovascular event . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9<br />
Discharge: from hospital to home. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9<br />
<strong>Medicines</strong> at discharge . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9<br />
Increasing use <strong>of</strong> rehabilitation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9<br />
Supporting environment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10<br />
In<strong>for</strong>mation <strong>for</strong> consumers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10<br />
Linking health consumer organisations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10<br />
Practice nurses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10<br />
IT, connectivity and data exchange . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10<br />
Tracking medicine use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10<br />
Missing in action . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11<br />
Hospital administrators and private health insurers . . . . . . . . . . . . . . . . . . . . . . 11<br />
Carers. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11<br />
[ 1 ]
Background<br />
Background<br />
The <strong>Heart</strong> Foundation Pharmaceutical<br />
Roundtable<br />
The Pharmaceutical Roundtable is made up <strong>of</strong><br />
the <strong>National</strong> <strong>Heart</strong> Foundation <strong>of</strong> Australia and<br />
11 pharmaceutical manufacturers: Alphapharm,<br />
AstaZeneca, CSL Biotherapies, Gilead, Eli Lilly,<br />
Merck Sharp & Dohme, Pfizer Australia, Roche,<br />
san<strong>of</strong>i-aventis, Solvay Pharmaceuticals and<br />
Servier Laboratories.<br />
About the project<br />
In July 2005, the Pharmaceutical Roundtable<br />
commissioned red 3 to explore <strong>Quality</strong> <strong>Use</strong> <strong>of</strong><br />
<strong>Cardiovascular</strong> <strong>Medicines</strong>. Specific goals <strong>of</strong> the<br />
project were to:<br />
• identify barriers to <strong>Quality</strong> <strong>Use</strong> <strong>of</strong><br />
<strong>Cardiovascular</strong> <strong>Medicines</strong><br />
• help the Roundtable develop strategies to<br />
overcome these barriers<br />
• prioritise actions to help the Roundtable<br />
achieve <strong>Quality</strong> <strong>Use</strong> <strong>of</strong> <strong>Cardiovascular</strong><br />
<strong>Medicines</strong>.<br />
red 3 conducted the research in three stages:<br />
1 Interviewing nearly fifty key stakeholders<br />
in cardiovascular health and <strong>Quality</strong> <strong>Use</strong><br />
<strong>of</strong> <strong>Medicines</strong>.<br />
2 Collating the contributions <strong>of</strong> these<br />
stakeholders and presenting the results to<br />
a <strong>National</strong> Stakeholder Workshop, held<br />
in Canberra on 25 November 2005. The<br />
event was structured to fill gaps in the<br />
work to date, correct misunderstandings<br />
and mistakes, and to add further detail. It<br />
also sought suggestions <strong>for</strong> practical action<br />
to achieve <strong>Quality</strong> <strong>Use</strong> <strong>of</strong> <strong>Medicines</strong> in<br />
<strong>Cardiovascular</strong> <strong>Health</strong>.<br />
3 Combining the workshop’s outcomes with<br />
findings reported in the research literature.<br />
This project built on previous research by red 3<br />
<strong>for</strong> the <strong>National</strong> <strong>Medicines</strong> Policy and The<br />
Pharmaceutical Alliance.<br />
[ 2 ]
<strong>Cardiovascular</strong> disease<br />
<strong>Quality</strong> <strong>Use</strong> <strong>of</strong> <strong>Medicines</strong><br />
<strong>Cardiovascular</strong> disease (CVD) is the cause <strong>of</strong><br />
more deaths in Australia than any other group<br />
<strong>of</strong> diseases. CVD accounted <strong>for</strong> 37.6 per cent <strong>of</strong><br />
all deaths in Australia during 2002. The burden<br />
<strong>of</strong> CVD continues to grow, as more and more<br />
Australians are living with the disease as a<br />
chronic condition.<br />
CVD is also a leading cause <strong>of</strong> long-term<br />
disability. In 1998, over 1.1 million Australians<br />
were affected —nearly one third <strong>of</strong> all people<br />
with a disability. Of concern is evidence that<br />
the burden <strong>of</strong> CVD is growing: in the 1990s,<br />
the prevalence <strong>of</strong> heart, stroke and vascular<br />
conditions rose by 18.2 per cent.<br />
The burden <strong>of</strong> cardiovascular disease is not<br />
spread evenly in the Australian community.<br />
CVD is more common among people in lower<br />
socio¬economic groups, and they are at a higher<br />
risk <strong>of</strong> developing the disease. People living in<br />
rural and remote areas are also more likely to die<br />
<strong>of</strong> CVD, as are Indigenous Australians.<br />
Co-morbidities with CVD are common—<br />
diabetes, renal failure and depression in<br />
particular. Over 80 per cent <strong>of</strong> elderly<br />
Australians have at least one chronic illness,<br />
and many have two or more.<br />
There is strong evidence that the burden<br />
<strong>of</strong> CVD on Australia’s health care system<br />
is growing. <strong>Cardiovascular</strong> conditions<br />
account <strong>for</strong> about 11 per cent <strong>of</strong> all problems<br />
managed by GPs in 2002–2003. CVD was the<br />
principal diagnosis <strong>of</strong> 7 per cent <strong>of</strong> all people<br />
hospitalised in 2001–2002.<br />
<strong>Medicines</strong> and CVD<br />
<strong>Medicines</strong> are one part <strong>of</strong> treating CVD.<br />
The main strategy <strong>for</strong> managing CVD is risk<br />
reduction, through lifestyle changes. Ways that<br />
medicines are used to treat CVD include:<br />
• reducing the risk <strong>of</strong> CVD—<strong>for</strong> example by<br />
lowering blood pressure, modifying lipid<br />
levels, and preventing blood clots<br />
• helping to open blocked arteries after a heart<br />
attack or stroke<br />
• helping to prevent the body rejecting<br />
implants and tissue grafts<br />
In the 1990s, Australia developed a <strong>National</strong><br />
<strong>Medicines</strong> Policy. It has four central objectives:<br />
• timely access to medicines that Australians<br />
need at a cost individuals and the<br />
community can af<strong>for</strong>d<br />
• medicines meeting appropriate standards <strong>of</strong><br />
quality, safety and efficacy<br />
• quality use <strong>of</strong> medicines<br />
• maintaining a responsible and viable<br />
medicines industry.<br />
The <strong>Quality</strong> <strong>Use</strong> <strong>of</strong> <strong>Medicines</strong> involves:<br />
1 Selecting management options wisely by:<br />
• considering the place <strong>of</strong> medicines in<br />
treating illness and maintaining health<br />
• recognising that there may be better ways<br />
than medicine to manage many disorders.<br />
2 Choosing suitable medicines if a medicine<br />
is considered necessary, so that the best<br />
available option is selected by taking into<br />
account:<br />
• the individual<br />
• the clinical condition<br />
• risks and benefits<br />
• dosage and length <strong>of</strong> treatment<br />
• any co-existing conditions<br />
• other therapies<br />
• monitoring considerations<br />
• costs <strong>for</strong> the individual, the community<br />
and the health system as a whole.<br />
3 Using medicines safely and effectively to get<br />
the best possible results by:<br />
• monitoring outcomes<br />
• minimising misuse, over-use and<br />
under-use<br />
• improving people’s ability to solve<br />
problems related to medication,<br />
such as negative effects or managing<br />
multiple medications.<br />
CVD / QUM<br />
• aiding recovery after surgery.<br />
[ 3 ]
Stages <strong>of</strong> <strong>Quality</strong> <strong>of</strong> <strong>Quality</strong> <strong>Use</strong> <strong>of</strong> <strong>Use</strong> <strong>Medicines</strong> <strong>of</strong> <strong>Medicines</strong> in <strong>Cardiovascular</strong> in <strong>Cardiovascular</strong> <strong>Health</strong> <strong>Health</strong><br />
Stages <strong>of</strong> QUM in CV <strong>Health</strong><br />
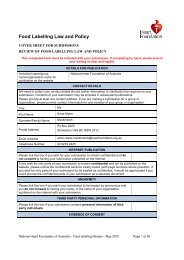
This summary presents the issues <strong>of</strong><br />
This summary presents the issues <strong>of</strong> greatest importance to those consulted. It has been organised<br />
greatest importance to those consulted. It<br />
around the patient’s journey through cardiovascular disease, summarised in the following diagram.<br />
has been organised around the patient’s<br />
journey through cardiovascular disease,<br />
summarised in the following diagram.<br />
be<strong>for</strong>e an event<br />
identifying<br />
people at risk<br />
1A<br />
diagnosing<br />
disease<br />
1B<br />
during an event<br />
cardiovascular<br />
event<br />
2<br />
lifestyle advice and<br />
prescribing medicine<br />
1<br />
getting<br />
people to<br />
hospital<br />
lifestyle<br />
changes<br />
3A<br />
3B<br />
dispensing<br />
medicine<br />
2<br />
admission<br />
4<br />
counselling and<br />
education<br />
3<br />
intervention<br />
5<br />
taking<br />
medicine<br />
4<br />
recovery<br />
6<br />
monitoring use<br />
and effects<br />
5<br />
discharge<br />
7<br />
adhering<br />
after an event<br />
1A<br />
2A<br />
3 4<br />
1B<br />
GP<br />
1C<br />
rehab<br />
2B<br />
carers<br />
support<br />
groups<br />
specialist<br />
physician<br />
community<br />
pharmacist<br />
nurses and<br />
allied health<br />
4<br />
[ 4 ]
Be<strong>for</strong>e a cardiovascular event<br />
Identifying people at risk <strong>of</strong> CVD<br />
Early identification <strong>of</strong> people at risk <strong>of</strong> CVD<br />
helps prevent the disease developing. Many<br />
people do not realise they are at risk until it is<br />
too late.<br />
There is strong support <strong>for</strong> a national risk<br />
assessment program to identify Australians at<br />
a higher risk <strong>of</strong> CVD. Those consulted stressed<br />
that such a program should cover other chronic<br />
illnesses, not just cardiovascular disease.<br />
Benefits <strong>of</strong> a national risk assessment program<br />
could include:<br />
• earlier identification <strong>of</strong> cardiovascular risk<br />
and cardiovascular disease<br />
• early targeting <strong>of</strong> specific risk factors<br />
• reducing mortality from CVD, improving<br />
quality <strong>of</strong> life, and potentially reducing the<br />
severity <strong>of</strong> cardiovascular events<br />
• lowering the financial burden <strong>of</strong><br />
CVD on consumers, families and the<br />
Australian community<br />
• creating greater predictability in health<br />
budgets and resource use by improved<br />
cost effectiveness.<br />
The main barriers to comprehensive risk<br />
assessment identified in this project were:<br />
• motivating Australians—particularly men—to<br />
go to a health pr<strong>of</strong>essional <strong>for</strong> an assessment<br />
• generating enough time <strong>for</strong> health<br />
pr<strong>of</strong>essionals to carry out a comprehensive<br />
risk assessment<br />
• funding.<br />
Encouraging consumers<br />
A barrier to improving treatment outcomes is<br />
that many Australians believe ‘doctor knows<br />
best’, and leave important decisions to their<br />
health pr<strong>of</strong>essionals. There is good evidence<br />
that consumers can achieve better health<br />
outcomes and quality <strong>of</strong> life if they actively take<br />
part in treatment decisions.<br />
Consumers should be encouraged to:<br />
• discuss their health, medical history and<br />
illnesses with their health pr<strong>of</strong>essionals<br />
• discuss their willingness to try various<br />
management options (such as better<br />
nutrition, physical activity, smoking<br />
cessation, and use <strong>of</strong> medicines)<br />
• provide health pr<strong>of</strong>essionals with accurate<br />
in<strong>for</strong>mation about all their medicines—<br />
including prescription, over-the-counter and<br />
complementary medicines<br />
• discuss costs and other constraints be<strong>for</strong>e<br />
selecting treatment options.<br />
Enabling General Practitioners<br />
There is already a great deal <strong>of</strong> in<strong>for</strong>mation<br />
and training materials on cardiovascular health<br />
<strong>for</strong> consumers and health pr<strong>of</strong>essionals. But,<br />
while these resources exist, they can be hard<br />
to find. Many documents, training courses,<br />
and educational resources are not available in<br />
an electronic <strong>for</strong>mat and there<strong>for</strong>e cannot be<br />
accessed online. Working out whether medical<br />
in<strong>for</strong>mation is evidence-based, up¬to-date and<br />
accurate can also be difficult <strong>for</strong> consumers and<br />
health care pr<strong>of</strong>essionals alike.<br />
One way to improve access to in<strong>for</strong>mation<br />
is to develop a portal <strong>for</strong> all cardiovascular<br />
in<strong>for</strong>mation, which brings together:<br />
Be<strong>for</strong>e a cardiovascular event<br />
• educational materials<br />
• clinical evidence<br />
• clinical practice guidelines<br />
• research<br />
• projects underway and completed<br />
• health services<br />
• support groups.<br />
[ 5 ]
Be<strong>for</strong>e a cardiovascular event (cont.)<br />
Be<strong>for</strong>e a cardiovascular event<br />
The bulk <strong>of</strong> cardiovascular risk assessment<br />
and prescribing is done in general practice.<br />
However, general practice is under significant<br />
pressure. A particular problem <strong>for</strong> GPs is the<br />
growing volume <strong>of</strong> clinical evidence and<br />
guidelines they are expected to know. The<br />
amount is far greater than they have to time<br />
read, and the volume too large to remember.<br />
GPs find keeping up to date difficult, especially<br />
when their patients have several conditions or<br />
are taking several medicines. The in<strong>for</strong>mation<br />
available to guide GPs is very fragmented<br />
and difficult to access as a whole. There is<br />
growing evidence that guidelines are not being<br />
translated into clinical practice.<br />
More effective ways need to be found to<br />
provide GPs with in<strong>for</strong>mation in ways that are<br />
manageable and memorable. Where effective<br />
methods have been found, they need to be<br />
more widely used.<br />
Counselling and education<br />
Some patients do not understand what their<br />
doctor tells them about cardiovascular disease or<br />
their treatment. Research has shown that patient<br />
confusion is responsible <strong>for</strong> nearly two-thirds<br />
<strong>of</strong> medicine-related problems after discharge<br />
from hospital. Research has also found that,<br />
while consumers are generally satisfied with<br />
their doctor’s technical knowledge, they felt that<br />
GPs’ greatest weakness is in communicating.<br />
The problem is not just a matter <strong>of</strong> doctors’<br />
skill, but also a lack <strong>of</strong> time to counsel patients,<br />
particularly when managing chronic diseases.<br />
Possible solutions include:<br />
• providing doctors with training on how to<br />
communicate with their patients<br />
• making greater use <strong>of</strong> nurses in general<br />
practice and hospitals to ‘interpret’ doctors’<br />
directions <strong>for</strong> patients and carers<br />
[ 6 ]<br />
Initiating medicines<br />
There is evidence that some doctors are underprescribing<br />
medicines which have been shown<br />
to be effective in reducing the risk <strong>of</strong> CVD.<br />
These include ACE inhibitors, beta-blockers and<br />
lipid-modifying drugs. Doctors would benefit<br />
from advice and training on:<br />
• the degree <strong>of</strong> current under-prescribing<br />
• risks posed by under-use <strong>of</strong> these medicines<br />
• appropriate use <strong>of</strong> these medicines<br />
• appropriate target doses<br />
Some <strong>of</strong> the common medicines used to reduce<br />
risk <strong>of</strong> cardiovascular disease can have side<br />
effects initially, and it may take doctors some<br />
time to find a <strong>for</strong>mulation or combination<br />
<strong>of</strong> medicines that is well-tolerated by the<br />
patient. This might involve switching between<br />
medicines, as well as titrating doses up and<br />
down. Many patients do not understand the<br />
reasons <strong>for</strong> these changes. Because <strong>of</strong> this, and<br />
the side effects, some patients refuse treatment.<br />
Some doctors need help explaining to<br />
consumers —be<strong>for</strong>e commencing a new<br />
medicine—why switching and changing doses<br />
is <strong>of</strong>ten necessary initially, and how long it may<br />
take to find a suitable medicine or combination<br />
<strong>of</strong> medicines.<br />
• greater counselling by pharmacists when<br />
dispensing medicines.<br />
Consumer medicine in<strong>for</strong>mation<br />
An important tool <strong>for</strong> educating consumers<br />
about their medicines is the Consumer<br />
Medicine In<strong>for</strong>mation (CMI) sheet. By law, all<br />
prescription and pharmacist-only medicines<br />
must have CMI. Topics that CMIs cover include:<br />
– the purpose <strong>of</strong> the medicine<br />
– issues to consider be<strong>for</strong>e taking the medicine<br />
– how to take the medicine correctly<br />
– what to do while taking the medicine<br />
– side effects<br />
– a description <strong>of</strong> the medicine.<br />
CMI is the only standardised consumer<br />
in<strong>for</strong>mation prepared <strong>for</strong> each individual<br />
medicine. They are normally provided<br />
by pharmacists at the time the medicine<br />
is dispensed.<br />
A 2004 review <strong>of</strong> pharmacies found that only<br />
12 per cent <strong>of</strong> consumers received a CMI when<br />
dispensed a prescription medicine. Also, many<br />
health pr<strong>of</strong>essionals, including nurses and<br />
specialist doctors, do not know that CMI exist.<br />
There is a widespread belief that consumers do<br />
not know to ask <strong>for</strong> CMI.
Consumers and health pr<strong>of</strong>essionals need to<br />
be further educated about CMI. Consumers<br />
should be encouraged to ask <strong>for</strong> CMI when<br />
collecting medicines.<br />
Adherence in the longer term<br />
There is evidence that once a person has started<br />
taking medicines, their adherence is likely to be<br />
poor—particularly to long-term management <strong>of</strong><br />
chronic disease.<br />
Adherence to preventative treatments is<br />
particularly low among patients without<br />
symptoms. Since many <strong>of</strong> the medicines<br />
prescribed <strong>for</strong> cardiovascular disease require<br />
minimum concentration levels to have any<br />
effect, low adherence means the medicine has<br />
either limited or no effect.<br />
Strategies shown to improve adherence include:<br />
• prescribing fewer daily doses (the more<br />
doses a person has to take, the more likely<br />
they are to miss one)<br />
• helping patients develop a schedule <strong>for</strong> their<br />
medicines<br />
• helping patients select reminders and<br />
• cues to take their medicines.<br />
Research shows that, while these strategies<br />
might work in the short term, few have been<br />
proved effective <strong>for</strong> long-term treatment. This is<br />
important <strong>for</strong> CVD, where the condition <strong>of</strong>ten<br />
requires long-term medicine use. Further work<br />
to promote long-term adherence to medication<br />
is needed.<br />
Home Medicine Reviews<br />
One tool to improve the use, effectiveness<br />
and safety <strong>of</strong> medicines is the Home Medicine<br />
Review (HMR). During an HMR, a pharmacist<br />
visits a patient’s home, to:<br />
– check that medicines are being used<br />
appropriately<br />
– identify problems with use<br />
– track medicine use<br />
– identify potential interactions<br />
– check <strong>for</strong> expired medicines<br />
Once completed, the pharmacist reports the<br />
results <strong>of</strong> the HMR to the referring doctor.<br />
HMRs are seen as particularly valuable after<br />
discharge from hospital, when they can help<br />
increase patient adherence and improve<br />
medication management.<br />
More pharmacists need to be trained to carry<br />
out HMRs, and doctors encouraged to request<br />
them when appropriate. Giving specialist<br />
doctors authority to order HMRs may also<br />
be helpful.<br />
Be<strong>for</strong>e a cardiovascular event<br />
[ 7 ]
During a cardiovascular event<br />
During a cardiovascular event<br />
Getting people to hospital<br />
When a cardiovascular event occurs, it is<br />
crucial to get treatment as soon as possible. A<br />
quarter <strong>of</strong> Australians die within an hour <strong>of</strong> their<br />
first symptoms, and the risk is greater <strong>for</strong> people<br />
who have already experienced a heart attack.<br />
Un<strong>for</strong>tunately, many people do not seek<br />
help early enough. They either die or sustain<br />
permanent damage. Currently, half <strong>of</strong> all<br />
heart attack deaths occur be<strong>for</strong>e the person<br />
reaches hospital.<br />
People at risk <strong>of</strong> CVD and their families need to<br />
be educated about:<br />
• recognising the symptoms <strong>of</strong> acute<br />
cardiovascular events<br />
• what to do if a cardiovascular event occurs<br />
—and how quickly action is required.<br />
Admission to hospital<br />
A major barrier to QUM in hospitals is<br />
inaccuracies in the medicine records developed<br />
at admission. Developing this record is <strong>of</strong>ten<br />
difficult because:<br />
• many patients cannot accurately remember<br />
what medicines they are using<br />
• the patient may be unable to speak<br />
• most patients do not keep a medicines list<br />
with them<br />
• patients or family members may not think to<br />
bring medicines when they come to hospital,<br />
and <strong>of</strong>ten do not bring packages with them,<br />
making identification difficult<br />
Further complications result from differences<br />
between hospitals. Each hospital has different<br />
processes <strong>for</strong> developing medicine lists.<br />
Hospitals also vary in how they record<br />
in<strong>for</strong>mation <strong>for</strong> future reference—especially<br />
<strong>for</strong> discharge.<br />
Possible solutions include:<br />
• creating a transferable or centralised<br />
electronic medicine record<br />
• developing a standard procedure <strong>for</strong><br />
recording patients’ medicine details<br />
at admission<br />
• asking people—particularly those at risk <strong>of</strong><br />
an acute cardiovascular event—to keep an<br />
up-to-date record <strong>of</strong> their medicines with<br />
them at all times.<br />
Engaging specialist physicians<br />
In the community, general practitioners make<br />
most decisions about the management <strong>of</strong> CVD,<br />
including use <strong>of</strong> medicines. In the last decade,<br />
there have been many programs to help GPs<br />
achieve <strong>Quality</strong> <strong>Use</strong> <strong>of</strong> <strong>Medicines</strong>.<br />
In hospitals, the key decisions about prescribing<br />
cardiovascular medicines are made by<br />
cardiologists. Compared with GPs, there have<br />
been few QUM programs designed specifically<br />
<strong>for</strong> specialists. New programs are needed <strong>for</strong><br />
specialist doctors, including cardiologists—<br />
especially as they are reported to be a major<br />
influence on GPs’ prescribing behaviour.<br />
• many patients do not mention overthe¬counter<br />
or complementary medicines.<br />
[ 8 ]
After a cardiovascular event<br />
Discharge: from hospital to home<br />
A major source <strong>of</strong> problems in the use <strong>of</strong><br />
cardiovascular medicines—and <strong>for</strong> the<br />
ongoing management <strong>of</strong> cardiovascular<br />
disease generally —is in the transition from<br />
hospital to home or residential care. Less than<br />
a third <strong>of</strong> GPs are told that their patients have<br />
been to hospital, or receive in<strong>for</strong>mation from<br />
the hospital.<br />
A particular object <strong>of</strong> criticism is the hospital<br />
discharge letter. Problems include:<br />
• many patients are not given a letter<br />
• many patients do not have a doctor to give<br />
the letter to<br />
• each hospital has its own discharge letter,<br />
leading to inconsistencies and omissions<br />
• many letters do not explain which medicines<br />
are to be reduced after discharge<br />
• many letters do not supply contact details in<br />
case <strong>of</strong> questions<br />
• letters frequently contain errors.<br />
One potential solution to this problem is to<br />
better align the PBS and hospital <strong>for</strong>mularies.<br />
Hospital pharmacists can also help by advising<br />
specialists on the availability and cost <strong>of</strong><br />
medicines <strong>for</strong> consumers after discharge.<br />
Increasing use <strong>of</strong> rehabilitation<br />
<strong>Medicines</strong> are only one part <strong>of</strong> management<br />
after a cardiovascular event. There is also a<br />
range <strong>of</strong> services to help people recover from a<br />
cardiovascular event, including rehabilitation,<br />
physiotherapy, specialised gymnasium<br />
programs, and community health centres. These<br />
are <strong>of</strong>ten poorly coordinated and in<strong>for</strong>mation<br />
about such programs can be difficult <strong>for</strong> both<br />
consumers and health pr<strong>of</strong>essionals to obtain.<br />
There is evidence <strong>of</strong> under-referral <strong>of</strong> patients to<br />
cardiac rehabilitation programs. This is because:<br />
• referral to rehabilitation is <strong>of</strong>ten not<br />
standard practice<br />
• rehabilitation is not accessible <strong>for</strong> all<br />
Australians, especially those in rural and<br />
remote areas<br />
After a cardiovascular event<br />
There is broad agreement that electronic<br />
or transferable health records would be the<br />
best way to reduce the loss <strong>of</strong> in<strong>for</strong>mation at<br />
discharge. In the absence <strong>of</strong> electronic records,<br />
an alternative is to improve and standardise<br />
discharge communication processes.<br />
<strong>Medicines</strong> at discharge<br />
Hospital pharmacies are funded separately<br />
from the PBS, and each hospital has its own<br />
<strong>for</strong>mulary. As a consequence:<br />
• hospitals may use medicines not listed on<br />
the PBS<br />
• hospitals and specialists may use medicines<br />
that are difficult or expensive <strong>for</strong> consumers<br />
to obtain after discharge.<br />
As a result, after a patient is discharged, their<br />
GP may need to change medicines prescribed<br />
in hospital. Some patients, however, can<br />
be unwilling to change from the medicines<br />
prescribed by their specialist. This can lead to<br />
unnecessarily high costs, patients not filling<br />
scripts, double-dosing, and lower adherence.<br />
• rehabilitation is not sufficiently attractive<br />
<strong>for</strong> Indigenous Australians, older women,<br />
people who do not speak English, and other<br />
disadvantaged groups.<br />
Ways to improve use <strong>of</strong> rehabilitation services,<br />
and there<strong>for</strong>e improve health outcomes <strong>for</strong><br />
those recovering from a cardiovascular event,<br />
include:<br />
• updating and promoting the <strong>Heart</strong><br />
Foundation’s register <strong>of</strong> cardiac rehabilitation<br />
centres and their services<br />
• developing and publicising a directory <strong>of</strong><br />
service providers, including physiotherapists,<br />
certified gymnasium instructors, and<br />
community health centres<br />
• encouraging GPs and cardiologists to<br />
make greater use <strong>of</strong> rehabilitation services<br />
where appropriate<br />
• encouraging patients to attend and complete<br />
rehabilitation courses.<br />
[ 9 ]
Supporting environment<br />
Supporting environment<br />
In<strong>for</strong>mation <strong>for</strong> consumers<br />
There is a substantial amount <strong>of</strong> in<strong>for</strong>mation<br />
available on topics such as healthy eating and<br />
physical activity <strong>for</strong> consumers and health<br />
pr<strong>of</strong>essionals. However, it is highly fragmented<br />
and <strong>of</strong>ten inconsistent. This can confuse<br />
consumers and discourage them from making<br />
positive changes to their lifestyle.<br />
Much existing lifestyle advice does not take into<br />
account the differing dietary requirements <strong>of</strong><br />
people with chronic diseases (such as limiting<br />
fluids or reducing salt intake). Some in<strong>for</strong>mation<br />
fails to explain how to balance competing<br />
demands <strong>for</strong> people with co-morbidities.<br />
Likewise, physical activity programs tend to<br />
focus on the impact <strong>of</strong> activity on individual<br />
diseases, but ignore the contributions <strong>of</strong> exercise<br />
to general well-being and mental health.<br />
There is a need <strong>for</strong> groups providing health<br />
advice to work together in order to develop<br />
consistent advice on nutrition and physical<br />
activity <strong>for</strong> people with CVD.<br />
Linking health consumer organisations<br />
Different health consumer organisations have<br />
much to learn from one another and to gain by<br />
pooling their skills. Greater collaboration could<br />
lead to:<br />
• better advocacy<br />
• better coordination<br />
• development and dissemination <strong>of</strong> consistent<br />
health messages<br />
• better services <strong>for</strong> rural and remote areas,<br />
where resources are scarce.<br />
Practice nurses<br />
To date, the health pr<strong>of</strong>essionals who have<br />
received the most attention in QUM programs<br />
have been doctors and pharmacists.<br />
Nurses also have an important role to play, but<br />
many are unaware <strong>of</strong> the basic QUM principles<br />
and lack access to key resources (such as<br />
CMI). Areas where nurses might play a greater<br />
role include:<br />
• undertaking cardiovascular risk assessments<br />
• follow-up after hospital discharge<br />
• checking adherence and medicine use<br />
• managing medical records<br />
• providing counselling and in<strong>for</strong>mation to<br />
consumers and families<br />
• translating medical advice <strong>for</strong> consumers<br />
and carers.<br />
IT, connectivity and data exchange<br />
Treating cardiovascular diseases involves<br />
long-term treatment, <strong>of</strong>ten by many health<br />
pr<strong>of</strong>essions in several health settings. Treatments<br />
frequently evolve over the patient’s lifetime.<br />
Management <strong>of</strong> many chronic diseases would<br />
be easier with electronic health records.<br />
There is strong support <strong>for</strong> electronic health<br />
records, either as a portable medical record<br />
or in a centrally-maintained database. It is<br />
believed that this will:<br />
• reduce error rates<br />
• reduce uncertainty when transferring patients<br />
between health care settings<br />
• reduce duplication <strong>of</strong> ef<strong>for</strong>t<br />
• allow tracking <strong>of</strong> medicine use.<br />
Ultimately, all <strong>of</strong> these things will help improve<br />
health outcomes.<br />
Greater use <strong>of</strong> IT connectivity may also improve<br />
communication between health pr<strong>of</strong>essionals<br />
and aid their decision-making.<br />
Tracking medicine use<br />
It is very difficult to track the use <strong>of</strong> medicines.<br />
This affects all levels <strong>of</strong> the health system. For<br />
example, at the practice level, it may be difficult<br />
<strong>for</strong> a doctor to know whether patients are filling<br />
their scripts and using their medicines. At the<br />
national level, there is currently little linkage<br />
between medication use and health outcomes,<br />
so it is difficult to assess the efficacy, safety and<br />
cost-effectiveness <strong>of</strong> treatment in everyday life.<br />
Identifying interactions and reasons <strong>for</strong> nonadherence<br />
is also difficult. More coordinated<br />
tracking <strong>of</strong> medicine use could help develop<br />
better policies and programs.<br />
[ 10 ]<br />
• giving advice to patients on nutrition and<br />
physical activity
Missing in action<br />
Hospital administrators and private<br />
health insurers<br />
Private health insurers fund a large part <strong>of</strong><br />
health spending. They are well placed to<br />
influence the uptake <strong>of</strong> QUM, particular by<br />
hospital health pr<strong>of</strong>essionals. They are in a<br />
position to encourage health service providers<br />
to adopt methods that provide QUM—such<br />
as early risk assessment and continuity <strong>of</strong> care<br />
plans. They also have the potential to link<br />
funding across different health settings in order<br />
to support ongoing care.<br />
Hospital administrators have not been drawn<br />
into QUM. Without their involvement, changes<br />
in hospital practice are unlikely.<br />
Carers<br />
Carers have proved difficult to draw into<br />
QUM. Other stakeholders recognise that they<br />
have a large role to play in helping patients<br />
make decisions about medicines and adhere<br />
to treatment. Lack <strong>of</strong> engagement is a barrier<br />
to QUM.<br />
Carers have needs <strong>of</strong> their own, which can<br />
be quite unlike those <strong>of</strong> patients. In particular<br />
they can need help to deal with the stress,<br />
social isolation, depression and anxiety that<br />
<strong>of</strong>ten results from supporting a person who<br />
is living with chronic CVD or has suffered an<br />
acute event.<br />
Carers’ needs include:<br />
Missing in action<br />
• in<strong>for</strong>mation on the cardiovascular disease<br />
affecting the person they are caring <strong>for</strong><br />
• knowledge about the treatments—<br />
particularly how to help people adhere to<br />
their medicines and lifestyle changes<br />
• psychological, social and emotional support.<br />
[ 11 ]
Notes<br />
Notes<br />
[ 12 ]
Australian Capital<br />
Territory<br />
Canberra<br />
15 Denison Street<br />
Deakin ACT 2600<br />
T: (02) 6282 5744<br />
New South Wales<br />
Sydney<br />
Level 3, 80 William Street<br />
Sydney NSW 2011<br />
T: (02) 9219 2444<br />
Northern Territory<br />
Darwin<br />
Darwin Central Offices<br />
3rd Floor, 21 Knuckey Street<br />
Darwin NT 0800<br />
T: (08) 8981 1966<br />
Queensland<br />
Brisbane<br />
557 Gregory Terrace<br />
Fortitude Valley QLD 4006<br />
T: (07) 3872 2500<br />
Tasmania<br />
Hobart<br />
86 Hampden Road<br />
Battery Point TAS 7004<br />
T: (03) 6224 2722<br />
Northern Tasmania<br />
Kings Meadows Community<br />
<strong>Health</strong> Centre, McHugh Street<br />
Kings Meadows TAS w7249<br />
T: (03) 6336 5116<br />
Victoria<br />
<strong>Heart</strong> Foundation Offices<br />
Newcastle<br />
Suite 5, OTP House<br />
Brad<strong>for</strong>d Close<br />
Kotara NSW 2289<br />
T: (02) 4952 4699<br />
Illawarra<br />
Kiama Hospital and<br />
Community <strong>Health</strong> Service<br />
Bonaira Street<br />
Kiama NSW 2533<br />
T: (02) 4232 0122<br />
Townsville<br />
Suite 7B, 95 Denham Street<br />
Townsville QLD 4810<br />
T: (07) 4721 4686<br />
South Australia<br />
Adelaide<br />
155-159 Hutt Street<br />
Adelaide SA 5000<br />
T: (08) 8224 2888<br />
Melbourne<br />
Level 12, 500 Collins Street<br />
Melbourne VIC 3000<br />
T: (03) 9329 8511<br />
Western Australia<br />
Perth<br />
334 Rokeby Road<br />
Subiaco WA 6008<br />
T: (08) 9388 3343<br />
[ 13 ]
<strong>Quality</strong> <strong>Use</strong> <strong>of</strong> <strong>Medicines</strong> <strong>for</strong> <strong>Cardiovascular</strong> <strong>Health</strong><br />
An initiative <strong>of</strong> the <strong>Heart</strong> Foundation Pharmacies Rountable<br />
Executive Summary<br />
<strong>Cardiovascular</strong> diseases are the greatest cause<br />
<strong>of</strong> death and disability in Australia, and they are<br />
becoming more common.<br />
Along with healthy lifestyle changes, medications<br />
are the main treatment <strong>for</strong> cardiovascular<br />
diseases. The Australian community spends over<br />
$1.5 billion a year on cardiovascular medicines.<br />
There is agreement that many are not being used<br />
to their best effect. Some are under prescribed.<br />
Many patients do not remain on long-term<br />
treatments. There are great losses <strong>of</strong> medicine<br />
in<strong>for</strong>mation when patients move between<br />
health care settings particularly into and out<br />
<strong>of</strong> hospitals. Providing consumers, carers and<br />
health pr<strong>of</strong>essionals with medicine in<strong>for</strong>mation is<br />
a continuing problem.<br />
In 2005, stakeholders were asked what was<br />
needed to achieve <strong>Quality</strong> <strong>Use</strong> <strong>of</strong> <strong>Medicines</strong><br />
(QUM) in cardiovascular health. Consumers,<br />
policy-makers, health pr<strong>of</strong>essionals and<br />
manufacturers all contributed.<br />
The result, presented in this report, was 128<br />
practical suggestions <strong>for</strong> action, along with a rich<br />
description <strong>of</strong> the problems and goals <strong>of</strong> those<br />
concerned with cardiovascular disease, and an<br />
outline <strong>of</strong> groups still to be engaged in QUM.<br />
The <strong>Heart</strong> Foundation Parmaceutical Roundtable members:<br />
HFN0490 JUL10<br />
©2010 <strong>National</strong> <strong>Heart</strong> Foundation <strong>of</strong> Australia ACN 008 419 761