Phenylalanine (PKU) neonatal Screening Assay - IBL international
Phenylalanine (PKU) neonatal Screening Assay - IBL international
Phenylalanine (PKU) neonatal Screening Assay - IBL international

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Instructions for Use<br />
<strong>Phenylalanine</strong> (<strong>PKU</strong>)<br />
<strong>neonatal</strong> <strong>Screening</strong><br />
<strong>Assay</strong><br />
Enzymatic <strong>Assay</strong> for the in-vitro-diagnostic quantitative determination<br />
of L-<strong>Phenylalanine</strong> in human newborn blood spots.<br />
For <strong>neonatal</strong> screening on Phenylketonuria.<br />
RE80015 RE80019<br />
480 2400<br />
2-8°C<br />
I B L I N T E R N A T I O N A L G M B H<br />
Flughafenstrasse 52a Phone: +49 (0)40-53 28 91-0 <strong>IBL</strong>@<strong>IBL</strong>-International.com<br />
D-22335 Hamburg, Germany Fax: +49 (0)40-53 28 91-11 www.<strong>IBL</strong>-International.com
<strong>Phenylalanine</strong> (<strong>PKU</strong>) <strong>neonatal</strong> <strong>Screening</strong> <strong>Assay</strong> (RE80015/RE80019)<br />
ENGLISH<br />
1. INTENDED USE<br />
Enzymatic <strong>Assay</strong> for the in-vitro-diagnostic quantitative determination of L-<strong>Phenylalanine</strong> in human newborn<br />
blood spots. For <strong>neonatal</strong> screening on Phenylketonuria.<br />
2. SUMMARY AND EXPLANATION<br />
Phenylketonuria (<strong>PKU</strong>) is one of the most often heriditary diseases of the metabolism of the amino acids. It<br />
is transmitted autosomal recessive to the descendant with an incidence of circa 1:2600 to 1:25000<br />
dependent on the observed population group.<br />
The main cause of the disease – 90 to 99% of all cases – is a decrease or the absence of the activity of the<br />
enzyme complex <strong>Phenylalanine</strong>hydroxylase which is responsible for the transformation of the essential<br />
amino acid <strong>Phenylalanine</strong> into Tyrosine. The latter is a precursor of the Catecholamines, Melanine and the<br />
thyroid hormones. Because of the blocking of this metabolism <strong>Phenylalanine</strong> is transformed by an<br />
alternative pathway to Phenylpyruvate and –acetate which are excreted by the kidneys.<br />
The disease becomes apparent by a mental retardation of the patients beginning in the first weeks of their<br />
life. Responsible for this development is the improper myelinization of the neurons in the brain because of<br />
the change in the protein metabolism. Other signs of the Phenylketonuria are the lacking of pigmentation of<br />
the dermis and its adnexis because of the disturbance of the synthesis of Melanine and therefore its<br />
predisposition of skin diseases.<br />
It is important to make the diagnosis of Phenylketonuria in the newborns because the cerebral damage can<br />
be prevented by a low <strong>Phenylalanine</strong> diet. Therefore a screening test for the detection of elevated<br />
<strong>Phenylalanine</strong> concentrations in the blood has to be made between the 2rd and the 5th day of the infants<br />
life. If this one is positive it is followed by a confirmatory assay to detect the special mutations on the<br />
chromosome 12.<br />
Many screening tests were developed for monitoring patients for Phenylketonuria. The first one called to its<br />
inventor GUTHRIE is based on the neutralization of an growth inhibiting factor of Bacillus subtilis by high<br />
<strong>Phenylalanine</strong> levels.<br />
Because of some disadvantages of this method it is replaced by assays in which the <strong>Phenylalanine</strong> in the<br />
blood of the patients takes part in a chemical reaction developing a fluorescinating or a coloured substance<br />
which can be measured quantitavely. The procedures can be used more conveniently in comparison to the<br />
more sophisticated and more expensive method of the HPLC.<br />
3. TEST PRINCIPLE<br />
The <strong>Phenylalanine</strong> of the blood spots is eluated quantitavely using Trichloracetic acid (3%) from the<br />
cellulose paper. After that the <strong>Phenylalanine</strong> is transformed by the enzyme <strong>Phenylalanine</strong>dehydrogenase to<br />
Phenylpyruvate. This reaction is coupled to the reduction of the coenzyme NAD+, present in the reaction<br />
mixture. The reduced NADH transforms in a redox reaction the added yellow Tetrazolium salt to the violet<br />
substrate Formazane. The amount of Formazane developed is proportional to the concentration of<br />
<strong>Phenylalanine</strong> in the sample. The color of the substrate can be measured with a photometer at 570 nm.<br />
4. WARNINGS AND PRECAUTIONS<br />
1. For in-vitro diagnostic use only. For professional use only.<br />
2. Before starting the assay, read the instructions completely and carefully. Use the valid version of the<br />
package insert provided with the kit. Be sure that everything is understood.<br />
3. In case of severe damage of the kit package please contact <strong>IBL</strong> or your supplier in written form, latest<br />
one week after receiving the kit. Do not use damaged components in test runs, but keep safe for<br />
complaint related issues.<br />
4. Obey lot number and expiry date. Do not mix reagents of different lots. Do not use expired reagents.<br />
5. Follow good laboratory practice and safety guidelines. Wear lab coats, disposable latex gloves and<br />
protective glasses where necessary.<br />
6. Reagents of this kit containing hazardous material may cause eye and skin irritations. See MATERIALS<br />
SUPPLIED and labels for details. Material Safety Data Sheets for this product are available on the <strong>IBL</strong>-<br />
Homepage or upon request directly from <strong>IBL</strong>.<br />
7. Chemicals and prepared or used reagents have to be treated as hazardous waste according to national<br />
biohazard and safety guidelines or regulations.<br />
V2012_01 1 / 7
<strong>Phenylalanine</strong> (<strong>PKU</strong>) <strong>neonatal</strong> <strong>Screening</strong> <strong>Assay</strong> (RE80015/RE80019)<br />
ENGLISH<br />
8. All reagents of this kit containing human serum or plasma have been tested and were found negative for<br />
anti-HIV I/II, HBsAg and anti-HCV. However, a presence of these or other infectious agents cannot be<br />
excluded absolutely and therefore reagents should be treated as potential biohazards in use and for<br />
disposal.<br />
5. STORAGE AND STABILITY<br />
The kit is shipped at ambient temperature and should be stored at 2-8°C. Keep away from heat or direct sun<br />
light. The storage and stability of specimen and prepared reagents is stated in the corresponding chapters.<br />
6. SPECIMEN COLLECTION AND STORAGE<br />
Blood Spots<br />
Blood from the newborn’s heel should be collected only from the medial or lateral section of the plantar<br />
surface. The usual precautions for blood collection should be observed. After puncture of the heel the first<br />
drop of blood should be wiped away with a sterile gauze.<br />
Touch the collection card against a large hanging drop of blood and allow a sufficient quantity of blood to<br />
soak into the filter paper in one step and so to fill the pre-printed circle completely. Repeat the procedure to<br />
fill the required number of pre-printed circles on the collection card.<br />
Allow the blood spots to air-dry for 3 h at room temperature away from direct sunlight.<br />
Because the standards are established with filter cards from Schleicher & Schuell No. 903 and<br />
there is a significant influence of the results by the filter card material (see LIMITATIONS OF THE<br />
PROCEDURE), it is recommended to use these cards also for the patient samples.<br />
Don’t squeeze the puncture site during the collection because this will cause hemolysis or dilution<br />
of the blood with tissue fluid. Don’t apply successive drops of blood to the same pre-printed circles.<br />
Don’t touch or smear the blood spots.<br />
Take care that the blood spot samples are visually okay (e.g. no blood smears, no coagulates, no<br />
finger-prints on the spots).<br />
The optimal collection point of time is 48 to 72 hours after birth. The blood sample should not be<br />
collected before the 36. and not after 72. hour after birth. In this time frame failed sample collection<br />
must be catch up without any further delay.<br />
In case of discharge before the 36. hour after birth or relocation the first sample should be taken.<br />
An earlier determination point of time as the 36. hour after birth raises the risk of false negative<br />
diagnostic findings. In case of discharge before the 36. hour after birth the parents (Care<br />
beneficiary) must be informed about exigency of second laboratory determination in due time.<br />
Extract from German Child Direction (BAnz. Nr. 60).<br />
National and country specific guidelines to sample collection point of time must be considered.<br />
Storage:<br />
2-8°C<br />
Keep away from heat or direct sun light.<br />
Stability:<br />
6 mon<br />
V2012_01 2 / 7
<strong>Phenylalanine</strong> (<strong>PKU</strong>) <strong>neonatal</strong> <strong>Screening</strong> <strong>Assay</strong> (RE80015/RE80019)<br />
ENGLISH<br />
7. MATERIALS SUPPLIED<br />
RE80019 RE80015 Symbol Component<br />
5 x 1 x ENZ LYO<br />
1 x 220 mL 1 x 45 mL ENZDIL<br />
1 x 260 mL 1 x 55 mL SUBS<br />
5 x 5 1 x 5 CAL A-E<br />
5 x 2 1 x 2 CONTROL1+2<br />
1 x 8 mL 1 x 2 mL DYE CONC<br />
Enzyme lyophilized<br />
Contains: phenylalanine dehydrogenase, Coenzyme NAD + , Buffer, stabilizers.<br />
Enzyme Diluent<br />
Ready to use. Contains: diethanolamine, Buffer, 0.01% NaN 3.<br />
Substrate<br />
Ready to use. Contains: tetrazolium salt, citrate buffer.<br />
Standard A-E<br />
~1; ~3; ~5; ~9; ~13 mg/dL<br />
Calibrated against CDC (Center for Disease Control and prevention).<br />
Contains: human blood. Schleicher & Schuell paper No. 903. 15 Blood Spots /<br />
card. Exact concentrations see labels or QC certficate.<br />
Control 1+2<br />
Control 1: ~ 2.0 – 3.0 mg/dL<br />
Control 2: ~ 4.0 – 6.0 mg/dL<br />
Contains: human blood. Schleicher & Schuell paper No. 903. 15 Blood Spots /<br />
card. Concentrations / acceptable ranges see labels or QC Certificate.<br />
Dye Stock Solution Concentrate (51 x)<br />
Contains: Acid Yellow 23 (C.I. 19140).<br />
8. MATERIALS REQUIRED BUT NOT SUPPLIED<br />
1. Micropipettes (Multipette Eppendorf or similar devices, < 3% CV). Volume: 25; 75; 100; 1000 µL<br />
2. Round-bottom polystyrene test tubes (12 x 75 mm)<br />
3. Rack for test tubes<br />
4. Shaker for test tubes<br />
5. Trichloracetic acid (3%; w/v); from 99.5% Trichloracetic acid, p.a. quality (e.g. Fluka, REF 91228)<br />
6. 0.5 M NaOH solution; (e.g. 1 N NaOH Titrisol Sol., Merck, REF 9956)<br />
7. Blood collection cards (Schleicher & Schuell 903 recommended)<br />
8. Blood spot puncher, 5 mm (1/5´´) (e.g. Sauer, Hannover, Germany)<br />
9. Microtiter Plate (flat bottom)<br />
10. Microtiter plate shaker (300-500 rpm; Amplitude 1.5-3.0 mm)<br />
11. Microtiter plate reader capable of reading absorbance at 570 nm (reference wavelength 690 nm)<br />
12. Bidistilled or deionised water<br />
13. Paper towels, pipette tips and timer<br />
9. PROCEDURE NOTES<br />
1. Any improper handling of samples or modification of the test procedure may influence the results. The<br />
indicated pipetting volumes, incubation times, temperatures and pretreatment steps have to be<br />
performed strictly according to the instructions. Use calibrated pipettes and devices only.<br />
2. Once the test has been started, all steps should be completed without interruption. Make sure that<br />
required reagents, materials and devices are prepared ready at the appropriate time. Allow all reagents<br />
and specimens to reach room temperature (18-25°C) and gently swirl each vial of liquid reagent and<br />
sample before use. Mix reagents without foaming.<br />
3. Avoid contamination of reagents, pipettes and wells/tubes. Use new disposable plastic pipette tips for<br />
each component and specimen. Do not interchange caps. Always cap not used vials. Do not reuse<br />
wells/tubes or reagents.<br />
4. Take care that the blood spot samples are visually okay (e.g. no blood smears, no coagulates, no fingerprints<br />
on the spots).<br />
5. It is advised to determine samples in duplicate to be able to identify potential pipetting errors.<br />
6. Use a pipetting scheme to verify an appropriate plate layout.<br />
7. Incubation time affects results. All wells should be handled in the same order and time sequences. It is<br />
recommended to use an 8-channel Micropipettor for pipetting of solutions in all wells.<br />
V2012_01 3 / 7
<strong>Phenylalanine</strong> (<strong>PKU</strong>) <strong>neonatal</strong> <strong>Screening</strong> <strong>Assay</strong> (RE80015/RE80019)<br />
ENGLISH<br />
10. PRE-TEST SETUP INSTRUCTIONS<br />
10.1. Preparation of Enyzme Stock Solution<br />
The Stock Solution is stable for 5 d at 2-8°C. Prepare only the amount of Enzyme Solution that is<br />
needed for the actual test run.<br />
Pipette 12 mL of bidist. water into the vial of the Enzyme, cap the vial and mix gently to dissolve.<br />
Mix 2 min. without foaming.<br />
10.2. Preparation of Enyzme Solution<br />
If you are using several vials of the Enzyme Stock Solution, it is highly recommended to pool the<br />
solution and to establish the ready for use Enzyme Solution from this pool.<br />
The Enzyme Solution is stable for 8 h at 18-25°C.<br />
The stability can not be extended by storing at 2–8 °C.<br />
Recommended amount for the Enzyme ready for use solution:<br />
No. of Microtiter Plates<br />
1 / 2 3 / 3 1 2 3 4 5<br />
Stock Solution (mL) 0.8 1.6 2.4 4.8 7.2 9.6 12<br />
Diluent (mL) 2.7 5.3 8.0 16.0 24.0 32.0 40.0<br />
Dilute Enzyme Stock Solution with Enzyme Diluent according to the table. Mix 2 min carefully<br />
without foaming.<br />
10.3. Preparation of Colored Trichloracetic Acid (3%)<br />
Dilute Dye Stock Solution (51x) with Trichloracetic acid (3%) 1:51 (e.g. add 2 mL Dye<br />
Concentrate to 100 mL of Trichloracetic acid (3%)).<br />
The solution is stable until the expiry date of the kit at 18-25°C.<br />
10.4. Elution of Blood Spots<br />
Punch Blood Spot Standards, Controls and samples (each 5 mm Ø = 1/5´´) and put each disc into<br />
one of the polystyrene tubes. Label all tubes.<br />
Pipette 100 µL of Colored Trichloracetic Acid (3%) into each tube. Assure that each disc is fully<br />
immersed in the liquid.<br />
Incubate 30–60 min at RT (18–25 °C) on an orbital shaker (300–500 U/min.; Amplitude 1.5–3 mm).<br />
11. TEST PROCEDURE<br />
1. Pipette 25 µL of 0.5 M NaOH into each well of the microtiter plate.<br />
2. Pipette 75 µL of each Standard, Control and sample Blood Spot Eluate into the respective wells.<br />
Shortly shake the plate.<br />
3. Pipette 100 µL of freshly prepared Enzyme Solution into each well.<br />
4. Incubate 30 min at RT (18–25°C).<br />
5. Pipette 100 µL of Substrate into each well. Shake plate for 3 min on an orbital shaker (300-500 rpm;<br />
Amplitude 1.5–3 mm).<br />
6. Measure Optical Density with a photometer at 570 nm (Reference-wavelength: 690 nm) within 3-5 min<br />
after pipetting of the Substrate Reagent.<br />
12. QUALITY CONTROL<br />
The test results are only valid if the test has been performed following the instructions. Moreover the user<br />
must strictly adhere to the rules of GLP (Good Laboratory Practice) or other applicable standards/laws. All<br />
kit controls must be found within the acceptable ranges as stated on the labels and the QC certificate. If the<br />
criteria are not met, the run is not valid and should be repeated. Each laboratory should use known samples<br />
as further controls. It is recommended to participate at appropriate quality assessment trials.<br />
In case of any deviation the following technical issues should be proven: Expiration dates of (prepared)<br />
reagents, storage conditions, pipettes, devices, incubation conditions and washing methods.<br />
V2012_01 4 / 7
<strong>Phenylalanine</strong> (<strong>PKU</strong>) <strong>neonatal</strong> <strong>Screening</strong> <strong>Assay</strong> (RE80015/RE80019)<br />
ENGLISH<br />
13. CALCULATION OF RESULTS<br />
The obtained OD of the standards are plotted against their concentration. The standard curve is calculated<br />
by a linear regression or a weighted linear regression function. Using computer programs, the curve is best<br />
described by a 2-point linear regression fit with linear axes.<br />
For the calculation of the regression curve, apply each signal of the standards (one obvious outlier of<br />
duplicates might be omitted and the more plausible single value might be used).<br />
The concentration of the samples can be read directly from the regression function.<br />
Samples showing signals above the highest standard have to be confirmed by a reference method.<br />
Conversion:<br />
1 mg/dL = 60.5 µmol/L<br />
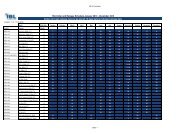
Typical Calibration Curve<br />
(Example. Do not use for calculation!)<br />
Standard <strong>Phenylalanine</strong> (mg/dL) OD Mean<br />
A 1.28 0.036<br />
B 2.73 0.065<br />
C 4.91 0.102<br />
D 9.31 0.179<br />
E 13.67 0.247<br />
OD (570 nm/690 nm ref.)<br />
0.30<br />
0.25<br />
0.20<br />
0.15<br />
0.10<br />
0.05<br />
<strong>Phenylalanine</strong><br />
y = 0.017x + 0.017<br />
R 2 = 0.999<br />
0.00<br />
0 5 10 15<br />
mg/dL<br />
14. INTERPRETATION OF RESULTS<br />
Based on the assumption that the expected values of phenylalanine follow a normal distribution blood spots<br />
with phenylalanine concentrations greater than 2.5 mg/dL (98% percentile) would be subsequently<br />
considered as "presumptive positive". Confirmation of the results would require repetition of the assay of 2%<br />
of the studied population.<br />
If the result of the repeated measurement (in duplicate) is above the threshold of 3.0 mg/dL, a new sample<br />
should be collected and analyzed applying a confirmatory assay.<br />
Based on classification scheme test results in the concentration range of 2.5 mg/dL to 3.0 mg/dL could<br />
potentially be diagnosed false negative and should be affirmed by additional measurement.<br />
Various societies for <strong>neonatal</strong> screening recommend different cut-off values for repetition of the<br />
measurement and the application of confirmatory assays. Depending on the application of samples of<br />
different populations of newborns it is highly recommended that each laboratory establishes its own range of<br />
normal values and that this distribution of values is co-ordinated with the recommendations of the<br />
responsible society of this geographic region.<br />
The results themselves should not be the only reason for any therapeutical consequences. They have to be<br />
correlated to other clinical observations and diagnostic tests.<br />
V2012_01 5 / 7
<strong>Phenylalanine</strong> (<strong>PKU</strong>) <strong>neonatal</strong> <strong>Screening</strong> <strong>Assay</strong> (RE80015/RE80019)<br />
ENGLISH<br />
15. EXPECTED VALUES<br />
Distribution of <strong>Phenylalanine</strong> Concentrations in Arbitrary Blood Spot Samples of Newborns<br />
_<br />
x = 1.6 mg/dL<br />
SD = 0.48 mg/dL<br />
n = 6693<br />
Population = Poland<br />
percentile mg/dL<br />
90% 2.16<br />
95% 2.35<br />
98% 2.51<br />
99% 1.45<br />
It is recommended that each laboratory establishes its own range of normal values.<br />
16. LIMITATIONS OF THE PROCEDURE<br />
Specimen collection has a significant effect on the test results. See SPECIMEN COLLECTION AND<br />
STORAGE for details.<br />
<strong>Screening</strong> Test. Any result with an elevated concentration has to be indicated as ‘presumptive positive’ and<br />
has to be confirmed with further sampling and testing.<br />
A false negative result of this assay cannot be excluded with absolute certainty. Any anamnestic or clinical<br />
hint of Phenylketonuria has to lead to a repeated measurement.<br />
A direct influence of applied drugs to the patients on the phenylalanine results cannot be excluded.<br />
Therefore, it is highly recommended in these cases to review even a normal phenylalanine value with a<br />
confirmation test if there are anamnestic or clinical signs of a phenylketonurie in a patient.<br />
It is recommended to use S&S 903 filter cards for the blood spot samples. When using other filter cards, the<br />
correction factor must be taken into account. For example, results with filter cards 2992 are ca. 20%<br />
different:<br />
Standards (2992) = 1.20 x (S&S 903) + 0.181; r = 0.996; n = 349<br />
For cross-reactivities, see PERFORMANCE.<br />
The following blood components do not have a significant effect on the test results up to the below stated<br />
concentrations:<br />
Hemoglobin<br />
Bilirubin<br />
Triglyceride<br />
5 mg/dL<br />
500 mg/dL<br />
3000 mg/dL<br />
V2012_01 6 / 7
<strong>Phenylalanine</strong> (<strong>PKU</strong>) <strong>neonatal</strong> <strong>Screening</strong> <strong>Assay</strong> (RE80015/RE80019)<br />
ENGLISH<br />
17. PERFORMANCE<br />
Analytical Specificity<br />
(Cross Reactivity)<br />
No cross-reactivities were found with the typical substances tested.<br />
Functional Sensitivity<br />
(Limit of Detection)<br />
1.55 mg/dL Functional Sensitivity, 20%; y = 26.33 x - 0.6304 R 2 = 0.82<br />
Precision Range (mg/dL) CV (%)<br />
Intra-<strong>Assay</strong> 2.68 – 9.60 5.8 – 11.0<br />
Inter-<strong>Assay</strong> 2.79 – 9.36 6.4 – 15.1<br />
Samples showing concentrations above the highest standard have to be confirmed by<br />
Linearity<br />
a reference method. A dilution of the sample is not possible, because there does not<br />
exist a blood without phenylalanine as diluent. Other diluents than extracts of<br />
phenylalanine free blood will probably have matrix effects.<br />
Mean (%) Range (%)<br />
Recovery<br />
107 92 - 127<br />
% Recovery after spiking<br />
Method Comparison<br />
versus Other <strong>Assay</strong><br />
<strong>IBL</strong>-<strong>Assay</strong> = 0.88 x Other <strong>Assay</strong> – 0.21 r = 0.95; n = 98<br />
18. PRODUCT LITERATURE REFERENCES<br />
1 Richtlinien des Bundesausschusses der Ärzte und Krankenkassen über die Früherkennung von<br />
Krankheiten bei Kindern bis zur Vollendung des 6. Lebensjahres („Kinder-Richtlinien“) BAnz. Nr. 60<br />
(2005)<br />
2 Rouse, B. et al. Maternal phenylketonuria syndrome: congenital heart defects, microcephaly and<br />
developmental outcomes. J. Pediat. 136: 57 – 61 (2000)<br />
3 Benit, P. et al. The mutant genotype is the main determinant of the metabolic phenotype in<br />
<strong>Phenylalanine</strong> hydroxylase deficiency. Molec. Genet. Metab. 68: 43 – 47 (1999)<br />
4 Kaufmann, S. A model of human <strong>Phenylalanine</strong> metabolism in normal subjects and in phenylketonuric<br />
patients. Proc. Nat. Acad. Scr. 96: 3160 – 3164 (1999)<br />
5 Sarkissian, C. N. et al. A different approach to treatment of phenylketonuria: <strong>Phenylalanine</strong> degradation<br />
with recombinant <strong>Phenylalanine</strong> ammonia lyase. Proc. Nat. Acad. Sci. 96: 2339 – 2344 (1999)<br />
6 Weglage, J. et al. Regression of neuropsychological deficits in early-treated phenylketonurics during<br />
adolescence. J. Inherit. Metab. Dis. 22: 693 – 705 (1999)<br />
7 Carter, K. C. et al. Mutation at the <strong>Phenylalanine</strong> hadroxylase gene (PAH) and its use to document<br />
population genetic variation: the Quebec experience. Europ. J. Hum. Genet. 6: 61 – 70 (1998)<br />
8 Guldberg, P. et al. A European multicenter study of <strong>Phenylalanine</strong> hydroxylase deficiency: classification<br />
of 105 mutations and a general system for genotype-based prediction of metabolic phenotype. Am. J.<br />
Hum. Genet. 63: 71 – 79 (1998)<br />
9 Van Spronsen, F. J. et al. Phenylketonuria: the in vivo hydroxylation rate of <strong>Phenylalanine</strong> into tyrosine is<br />
decreased. J. Clin. Invest. 101: 2875 – 2880 (1998)<br />
10 Rouse, B. et al. Maternal phenylketonuria collaborative study (M<strong>PKU</strong>CS) offspring: facial anomalies,<br />
malformations and early neurological sequelae. Am. J. Med. Genet. 69: 89 – 95 (1997)<br />
11 Guthrie, R. The introduction of newborn screening for phenylketonuria: a personal history. Europ. J.<br />
Pediat. 155 (suppl. 1): 4 – 5 (1996)<br />
V2012_01 7 / 7
Symbols / Symbole / Symbôles / Símbolos / Símbolos / Σύµβολα<br />
REF<br />
LOT<br />
Cat.-No.: / Kat.-Nr.: / No.- Cat.: / Cat.-No.: / N.º Cat.: / N.–Cat.: / Αριθµός-Κατ.:<br />
Lot-No.: / Chargen-Bez.: / No. Lot: / Lot-No.: / Lote N.º: / Lotto n.: / Αριθµός -Παραγωγή:<br />
Use by: / Verwendbar bis: / Utiliser à: / Usado por: / Usar até: / Da utilizzare entro: /<br />
Χρησιµοποιείται από:<br />
No. of Tests: / Kitgröße: / Nb. de Tests: / No. de Determ.: / N.º de Testes: / Quantità dei tests: /<br />
Αριθµός εξετάσεων:<br />
CONC Concentrate / Konzentrat / Concentré / Concentrar / Concentrado / Concentrato / Συµπύκνωµα<br />
LYO<br />
IVD<br />
Lyophilized / Lyophilisat / Lyophilisé / Liofilizado / Liofilizado / Liofilizzato / Λυοφιλιασµένο<br />
In Vitro Diagnostic Medical Device. / In-vitro-Diagnostikum. / Appareil Médical pour Diagnostics In<br />
Vitro. / Dispositivo Médico para Diagnóstico In Vitro. / Equipamento Médico de Diagnóstico In<br />
Vitro. / Dispositivo Medico Diagnostico In vitro. / Ιατρική συσκευή για In-Vitro ∆ιάγνωση.<br />
Evaluation kit. / Nur für Leistungsbewertungszwecke. / Kit pour évaluation. / Juego de Reactivos<br />
para Evaluació. / Kit de avaliação. / Kit di evaluazione. / Κιτ Αξιολόγησης.<br />
Read instructions before use. / Arbeitsanleitung lesen. / Lire la fiche technique avant emploi. /<br />
Lea las instrucciones antes de usar. / Ler as instruções antes de usar. / Leggere le istruzioni<br />
prima dell’uso. / ∆ιαβάστε τις οδηγίες πριν την χρήση.<br />
Keep away from heat or direct sun light. / Vor Hitze und direkter Sonneneinstrahlung schützen. /<br />
Garder à l’abri de la chaleur et de toute exposition lumineuse. / Manténgase alejado del calor o la<br />
luz solar directa. / Manter longe do calor ou luz solar directa. / Non esporre ai raggi solari. / Να<br />
φυλάσσεται µακριά από θερµότητα και άµεση επαφή µε το φως του ηλίου.<br />
Store at: / Lagern bei: / Stocker à: / Almacene a: / Armazenar a: / Conservare a: / Αποθήκευση<br />
στους:<br />
Manufacturer: / Hersteller: / Fabricant: / Productor: / Fabricante: / Fabbricante: / Παραγωγός:<br />
Caution! / Vorsicht! / Attention! / ¡Precaución! / Cuidado! / Attenzione! / Προσοχή!<br />
Symbols of the kit components see MATERIALS SUPPLIED.<br />
Die Symbole der Komponenten sind im Kapitel KOMPONENTEN DES KITS beschrieben.<br />
Voir MATERIEL FOURNI pour les symbôles des composants du kit.<br />
Símbolos de los componentes del juego de reactivos, vea MATERIALES SUMINISTRADOS.<br />
Para símbolos dos componentes do kit ver MATERIAIS FORNECIDOS.<br />
Per i simboli dei componenti del kit si veda COMPONENTI DEL KIT.<br />
Για τα σύµβολα των συστατικών του κιτ συµβουλευτείτε το ΠΑΡΕΧΟΜΕΝΑ ΥΛΙΚΑ.<br />
<strong>IBL</strong> AFFILIATES WORLDWIDE<br />
<strong>IBL</strong> International GmbH<br />
Flughafenstr. 52A, 22335 Hamburg, Germany<br />
<strong>IBL</strong> International Corp.<br />
194 Wildcat Road, Toronto, Ontario M3J 2N5, Canada<br />
Tel.: + 49 (0) 40 532891 -0 Fax: -11<br />
E-MAIL: <strong>IBL</strong>@<strong>IBL</strong>-International.com<br />
WEB: http://www.<strong>IBL</strong>-International.com<br />
Tel.: +1 (416) 645 -1703 Fax: -1704<br />
E-MAIL: Sales@<strong>IBL</strong>-International.com<br />
WEB: http://www.<strong>IBL</strong>-International.com<br />
LIABILITY: Complaints will be accepted in each mode –written or vocal. Preferred is that the complaint is accompanied with the test performance<br />
and results. Any modification of the test procedure or exchange or mixing of components of different lots could negatively affect the results. These<br />
cases invalidate any claim for replacement. Regardless, in the event of any claim, the manufacturer’s liability is not to exceed the value of the test kit.<br />
Any damage caused to the kit during transportation is not subject to the liability of the manufacturer<br />
Symbols Version 3.5 / 2012-01-20