

Iatrogenic Left Diaphragmatic Hernia as a Complication of Hydatid ...
Iatrogenic Left Diaphragmatic Hernia as a Complication of Hydatid ...
Iatrogenic Left Diaphragmatic Hernia as a Complication of Hydatid ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
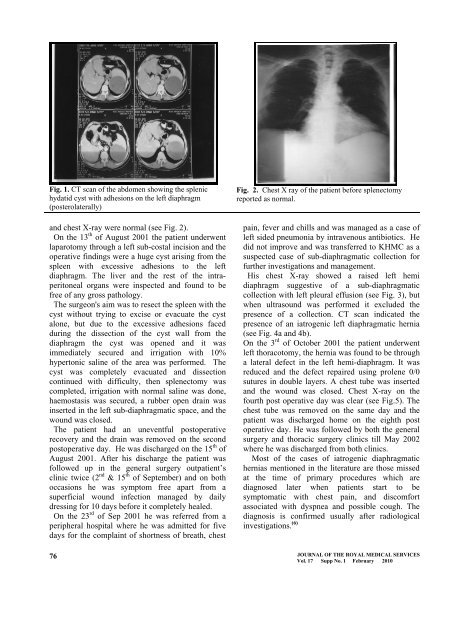
Fig. 1. CT scan <strong>of</strong> the abdomen showing the splenic<br />
hydatid cyst with adhesions on the left diaphragm<br />
(posterolaterally)<br />
and chest X-ray were normal (see Fig. 2).<br />
On the 13 th <strong>of</strong> August 2001 the patient underwent<br />
laparotomy through a left sub-costal incision and the<br />
operative findings were a huge cyst arising from the<br />
spleen with excessive adhesions to the left<br />
diaphragm. The liver and the rest <strong>of</strong> the intraperitoneal<br />
organs were inspected and found to be<br />
free <strong>of</strong> any gross pathology.<br />
The surgeon's aim w<strong>as</strong> to resect the spleen with the<br />
cyst without trying to excise or evacuate the cyst<br />
alone, but due to the excessive adhesions faced<br />
during the dissection <strong>of</strong> the cyst wall from the<br />
diaphragm the cyst w<strong>as</strong> opened and it w<strong>as</strong><br />
immediately secured and irrigation with 10%<br />
hypertonic saline <strong>of</strong> the area w<strong>as</strong> performed. The<br />
cyst w<strong>as</strong> completely evacuated and dissection<br />
continued with difficulty, then splenectomy w<strong>as</strong><br />
completed, irrigation with normal saline w<strong>as</strong> done,<br />
haemost<strong>as</strong>is w<strong>as</strong> secured, a rubber open drain w<strong>as</strong><br />
inserted in the left sub-diaphragmatic space, and the<br />
wound w<strong>as</strong> closed.<br />
The patient had an uneventful postoperative<br />
recovery and the drain w<strong>as</strong> removed on the second<br />
postoperative day. He w<strong>as</strong> discharged on the 15 th <strong>of</strong><br />
August 2001. After his discharge the patient w<strong>as</strong><br />
followed up in the general surgery outpatient’s<br />
clinic twice (2 nd & 15 th <strong>of</strong> September) and on both<br />
occ<strong>as</strong>ions he w<strong>as</strong> symptom free apart from a<br />
superficial wound infection managed by daily<br />
dressing for 10 days before it completely healed.<br />
On the 23 rd <strong>of</strong> Sep 2001 he w<strong>as</strong> referred from a<br />
peripheral hospital where he w<strong>as</strong> admitted for five<br />
days for the complaint <strong>of</strong> shortness <strong>of</strong> breath, chest<br />
Fig. 2. Chest X ray <strong>of</strong> the patient before splenectomy<br />
reported <strong>as</strong> normal.<br />
pain, fever and chills and w<strong>as</strong> managed <strong>as</strong> a c<strong>as</strong>e <strong>of</strong><br />
left sided pneumonia by intravenous antibiotics. He<br />
did not improve and w<strong>as</strong> transferred to KHMC <strong>as</strong> a<br />
suspected c<strong>as</strong>e <strong>of</strong> sub-diaphragmatic collection for<br />
further investigations and management.<br />
His chest X-ray showed a raised left hemi<br />
diaphragm suggestive <strong>of</strong> a sub-diaphragmatic<br />
collection with left pleural effusion (see Fig. 3), but<br />
when ultr<strong>as</strong>ound w<strong>as</strong> performed it excluded the<br />
presence <strong>of</strong> a collection. CT scan indicated the<br />
presence <strong>of</strong> an iatrogenic left diaphragmatic hernia<br />
(see Fig. 4a and 4b).<br />
On the 3 rd <strong>of</strong> October 2001 the patient underwent<br />
left thoracotomy, the hernia w<strong>as</strong> found to be through<br />
a lateral defect in the left hemi-diaphragm. It w<strong>as</strong><br />
reduced and the defect repaired using prolene 0/0<br />
sutures in double layers. A chest tube w<strong>as</strong> inserted<br />
and the wound w<strong>as</strong> closed. Chest X-ray on the<br />
fourth post operative day w<strong>as</strong> clear (see Fig.5). The<br />
chest tube w<strong>as</strong> removed on the same day and the<br />
patient w<strong>as</strong> discharged home on the eighth post<br />
operative day. He w<strong>as</strong> followed by both the general<br />
surgery and thoracic surgery clinics till May 2002<br />
where he w<strong>as</strong> discharged from both clinics.<br />
Most <strong>of</strong> the c<strong>as</strong>es <strong>of</strong> iatrogenic diaphragmatic<br />
herni<strong>as</strong> mentioned in the literature are those missed<br />
at the time <strong>of</strong> primary procedures which are<br />
diagnosed later when patients start to be<br />
symptomatic with chest pain, and discomfort<br />
<strong>as</strong>sociated with dyspnea and possible cough. The<br />
diagnosis is confirmed usually after radiological<br />
investigations. (6) JOURNAL OF THE ROYAL MEDICAL SERVICES<br />
76<br />
Vol. 17 Supp No. 1 February 2010














