

Evaluating the Adult with Cerebral Palsy for ... - Physical Therapy
Evaluating the Adult with Cerebral Palsy for ... - Physical Therapy
Evaluating the Adult with Cerebral Palsy for ... - Physical Therapy

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
PRACTICE<br />
limited number of clients, who often have low muscle tone<br />
ra<strong>the</strong>r than high muscle tone.<br />
Therapists should assess <strong>the</strong> foot-support system in <strong>the</strong><br />
fitting chair. Because many clients <strong>for</strong> adaptive seating have<br />
hamstring spasticity or knee flexion contractures beyond 75<br />
degrees, footrests extended in front of <strong>the</strong> casters in <strong>the</strong> usual<br />
position are not appropriate. To prevent <strong>the</strong> hamstrings from<br />
functioning as hip extensors, a foot box or leng<strong>the</strong>ned foot<br />
support may be used to allow 90 degrees or more of flexion<br />
at <strong>the</strong> knees (Fig. 2). The foot box should extend <strong>for</strong>ward<br />
beyond <strong>the</strong> reach of <strong>the</strong> heels and back under <strong>the</strong> seat as<br />
needed. Calf panels or pads should not be used <strong>with</strong> this type<br />
of foot box to avoid hamstring facilitation.<br />
When <strong>the</strong> client is seated fully upright, a tray may be<br />
suitable <strong>for</strong> support much <strong>the</strong> way we use a table or desk top.<br />
Plans <strong>for</strong> <strong>the</strong> tray should usually be determined during <strong>the</strong><br />
assessment process. The fit, height, and tilt of <strong>the</strong> tray are<br />
important in achieving <strong>the</strong> best posture and muscle tone. A<br />
tilted tray may help to maintain hands in midline and in<br />
contact <strong>with</strong> each o<strong>the</strong>r. A tray may also be essential <strong>for</strong><br />
clients whose muscle tone decreases excessively when <strong>the</strong> hips<br />
and trunk are at a 90-degree angle. The tray may be provided<br />
<strong>with</strong> a high inner rim <strong>for</strong> trunk support, or it may provide<br />
support only through <strong>the</strong> arms as <strong>the</strong> elbows rest on <strong>the</strong> tray.<br />
Fig. 1. Optimal angle of <strong>the</strong> seating unit can be determined by<br />
placing a wedge beneath front casters to observe varying angles of<br />
tilt.<br />
DISCUSSION<br />
Bergen and Colangelo noted that "a majority of clients <strong>with</strong><br />
disorders of tone show a posterior pelvic tilt when sitting"<br />
because of "overactivity of hip extensors. " 2(p5) They also noted<br />
that <strong>the</strong> posterior tilt leads to <strong>the</strong> full extension pattern. The<br />
pelvis must, <strong>the</strong>re<strong>for</strong>e, approximate as nearly as possible <strong>the</strong><br />
normal anterior tilt position in sitting. Wedging <strong>the</strong> seat<br />
invariably increases <strong>the</strong> posterior tilt in clients who lack full<br />
hip mobility. This loss of <strong>the</strong> anterior tilt is <strong>the</strong> reason that<br />
wedging of <strong>the</strong> seat has often been unsuccessful in correcting<br />
<strong>the</strong> problem of extensor spasticity in sitting.<br />
Underlying <strong>the</strong> practice of wedging is <strong>the</strong> firm belief that<br />
reducing <strong>the</strong> angle of <strong>the</strong> hips to 90 degrees or less inhibits<br />
extensor spasticity. That premise is not in question here. If<br />
<strong>the</strong> pelvis is tilted posteriorly, however, <strong>the</strong> hip angle may<br />
only appear to be 90 degrees. The true angle of <strong>the</strong> hip will<br />
often be significantly greater than 90 degrees. The true angle<br />
determines whe<strong>the</strong>r spasticity will be inhibited.<br />
The reclining position, often used <strong>with</strong> a wedged seat <strong>for</strong><br />
severely spastic clients, is successful only in a passive sense.<br />
As spasticity subsides and <strong>the</strong> client relaxes, he may sink back<br />
into <strong>the</strong> seat ra<strong>the</strong>r than extending out of <strong>the</strong> wheelchair.<br />
Moreover, extensor activity is not reduced by reclining and<br />
may actually increase. In <strong>the</strong> a<strong>for</strong>ementioned EMG study by<br />
Nwaobi et al, reclining <strong>the</strong> back as little as 15 degrees <strong>with</strong><br />
<strong>the</strong> hips maintained at 90 degrees flexion produced more low<br />
back extensor myoelectric activity than when <strong>the</strong> back was<br />
straight upright. 7 At 30 degrees of a reclined position, <strong>with</strong><br />
<strong>the</strong> hips maintained at 90 degrees, extensor tone was still<br />
higher. The results of this study suggest that reclining a client<br />
ei<strong>the</strong>r elicits <strong>the</strong> supine tonic labyrinthine reflex, or contact<br />
of <strong>the</strong> back or <strong>the</strong> head <strong>with</strong> a headrest initiates <strong>the</strong> extensor<br />
response. Nwaobi et al do not speculate on ei<strong>the</strong>r of <strong>the</strong>se<br />
reactions as possible contributing factors. 7 In ei<strong>the</strong>r event, we<br />
must be aware of <strong>the</strong> results of this study and carefully assess<br />
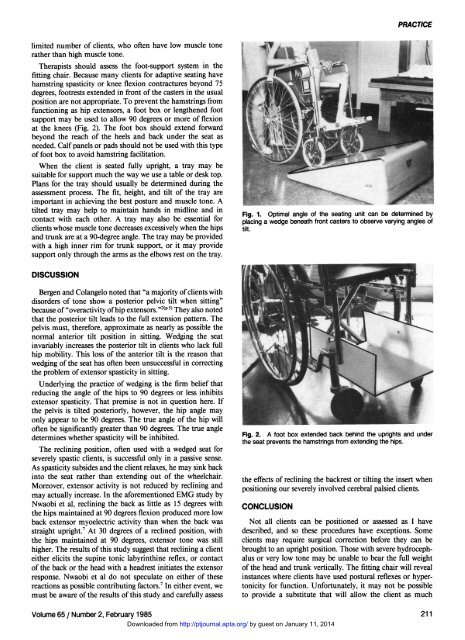
Fig. 2. A foot box extended back behind <strong>the</strong> uprights and under<br />
<strong>the</strong> seat prevents <strong>the</strong> hamstrings from extending <strong>the</strong> hips.<br />
<strong>the</strong> effects of reclining <strong>the</strong> backrest or tilting <strong>the</strong> insert when<br />
positioning our severely involved cerebral palsied clients.<br />
CONCLUSION<br />
Not all clients can be positioned or assessed as I have<br />
described, and so <strong>the</strong>se procedures have exceptions. Some<br />
clients may require surgical correction be<strong>for</strong>e <strong>the</strong>y can be<br />
brought to an upright position. Those <strong>with</strong> severe hydrocephalus<br />
or very low tone may be unable to bear <strong>the</strong> full weight<br />
of <strong>the</strong> head and trunk vertically. The fitting chair will reveal<br />
instances where clients have used postural reflexes or hypertonicity<br />
<strong>for</strong> function. Un<strong>for</strong>tunately, it may not be possible<br />
to provide a substitute that will allow <strong>the</strong> client as much<br />
Volume 65 / Number 2, February 1985 211<br />
Downloaded from http://ptjournal.apta.org/ by guest on January 11, 2014













