Nebulized salbutamol with and without ipratropium bromide in the ...
Nebulized salbutamol with and without ipratropium bromide in the ...
Nebulized salbutamol with and without ipratropium bromide in the ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
168 Garrett et al. J ALLERGY CLIN IMMUNOI_<br />
AUGUST 1997<br />
A FEV~<br />
600 r~ Combivent<br />
Salbutamol<br />
500 * * P 1 L [254<br />
patients; 77% Combivent, 74% <strong>salbutamol</strong>]). Patients<br />
<strong>with</strong> an FEV 1 of less than 1 L exhibited only a small<br />
benefit from Combivent (359 _+ 56 ml) compared <strong>with</strong><br />
<strong>salbutamol</strong> alone (337 +_ 66 ml; difference = 22 ml [not<br />
significant]), whereas those <strong>with</strong> an FEVj -> 1 L exhibited<br />
a significant benefit from Combivent (522 _+ 44 ml)<br />
compared <strong>with</strong> <strong>salbutamol</strong> alone (346 + 38 ml; difference<br />
= 176 ml) (p < 0.005) (Fig. 2).<br />
Sixty-six patients <strong>in</strong>dicated no prior use of an <strong>in</strong>haled<br />
[3-agonist. The 41 patients <strong>in</strong> <strong>the</strong> Combivent group had a<br />
mean &FEV~ 90 of 853 -+ 125 ml, which translated to a<br />
treatment difference of 315 + 135 ml <strong>in</strong> favor of<br />
Combivent over <strong>salbutamol</strong> (Fig. 3, A). Patients were<br />
<strong>the</strong>n grouped accord<strong>in</strong>g to <strong>in</strong>haled ~3-agonist <strong>in</strong>take <strong>in</strong><br />
<strong>the</strong> previous 6 hours or serum <strong>salbutamol</strong> levels (patients<br />
tak<strong>in</strong>g bricanyl or fenoterol were excluded from<br />
this analysis In = 50]) at basel<strong>in</strong>e before nebulization of<br />
<strong>the</strong> study drugs (Fig. 3, B). Patients who had consumed<br />
<strong>the</strong> most {3-agonist before ED attendance exhibited a<br />
smaller <strong>in</strong>crease <strong>in</strong> FEV1 after adm<strong>in</strong>istration of nebulized<br />
bronchodilator <strong>and</strong> were least likely to show any<br />
benefit from <strong>the</strong> addition of Combivent (Fig. 3, A <strong>and</strong><br />
B).<br />
Although <strong>in</strong>haled <strong>ipratropium</strong> (7.4% of subjects)<br />
taken <strong>in</strong> <strong>the</strong> 6 hours before ED attendance appeared to<br />
<strong>in</strong>fluence AFEV~ 90 <strong>in</strong> <strong>the</strong> ANCOVA (Table I, model 5)<br />
(p = 0.01), <strong>the</strong> effect was nonsignificant (p = 0.12) when<br />
it was <strong>in</strong>cluded <strong>in</strong> <strong>the</strong> saturated model (model 9). This<br />
was expla<strong>in</strong>ed by <strong>the</strong> strong association between frequent<br />
<strong>in</strong>haled 13-agonist use <strong>and</strong> any <strong>in</strong>haled <strong>ipratropium</strong><br />
use before ED attendance. Oral <strong>the</strong>ophyll<strong>in</strong>e use, serum<br />
<strong>the</strong>ophyll<strong>in</strong>e at basel<strong>in</strong>e (for those tak<strong>in</strong>g <strong>the</strong>ophyll<strong>in</strong>e),<br />
<strong>and</strong> steroid use (<strong>in</strong>haled or oral) did not <strong>in</strong>fluence<br />
AFEV 1 90.<br />
There was no difference <strong>in</strong> mean heart rate, blood<br />
pressure, oxygen saturation, <strong>and</strong> respiratory rate between<br />
<strong>the</strong> treatment groups over <strong>the</strong> 90-m<strong>in</strong>ute study<br />
period; <strong>and</strong> <strong>the</strong>re were no differences <strong>in</strong> frequency of<br />
adverse events, apart from a somewhat greater need for<br />
A FEV 1<br />
(_+ SE) (ml)<br />
A<br />
900<br />
800<br />
700<br />
600<br />
500<br />
400<br />
300<br />
200<br />
100<br />
0<br />
i--i<br />
Nil 1 - 9 puffs _>10 puffs<br />
No. of puffs of <strong>in</strong>haled J3-Agonist <strong>in</strong> 6 hours prior to ED visit<br />
* * ( I Combivent<br />
r--1<br />
700 ~l<br />
6OO<br />
5OO<br />
zX FEV 1<br />
400<br />
(+ SE) (m0<br />
300<br />
B<br />
20O<br />
100<br />
0<br />
0 - 2 mmol/1 >2 mmol/1<br />
Serum Salbutamol level<br />
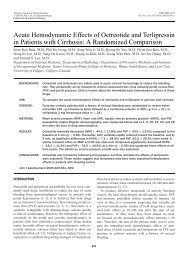
FIG. 3. A, Effect of <strong>in</strong>haled 13-agonist <strong>in</strong> previous 6 hours on response<br />
to Combivent compared <strong>with</strong> <strong>salbutamol</strong> at 90 m<strong>in</strong>utes (a nebulizer<br />
of 13-agonist was def<strong>in</strong>ed as 20 puffs through a metered-dose <strong>in</strong>haler).<br />
B, Effect of serum <strong>salbutamol</strong> level on presentation at ED on<br />
AFEV 1 90 (Combivent vs <strong>salbutamol</strong>) analyzed <strong>in</strong> patients who were<br />
tak<strong>in</strong>g <strong>in</strong>haled <strong>salbutamol</strong> or no 13-agonist (n = 271, 80%).<br />
hospitalization <strong>in</strong> <strong>the</strong> <strong>salbutamol</strong> treatment group<br />
(22.3%) compared <strong>with</strong> <strong>the</strong> Combivent group (15.3%,<br />
not significant).<br />
DISCUSSION<br />
Our data show that a significant improvement <strong>in</strong> lung<br />
function is associated <strong>with</strong> <strong>the</strong> addition of <strong>ipratropium</strong> to<br />
<strong>salbutamol</strong> (2.5 mg) <strong>in</strong> <strong>the</strong> <strong>in</strong>itial management of acute<br />
severe asthma. Fur<strong>the</strong>r, <strong>the</strong> improvement was achieved<br />
<strong>with</strong>out additional side effects or cardiovascular changes,<br />
<strong>in</strong>clud<strong>in</strong>g changes <strong>in</strong> pulse <strong>and</strong> blood pressure.<br />
The majority of previous studies had <strong>the</strong> potential for<br />
a large type II error <strong>and</strong> had wide confidence <strong>in</strong>tervals<br />
for pulmonary function outcome variables. 12 To avoid<br />
this, we estimated a study size of at least 326 patients to<br />
detect at <strong>the</strong> c~ = 0.05 significance level a 150 ml<br />
difference <strong>in</strong> FEV1 <strong>with</strong> 90% probability. The improvement<br />
<strong>in</strong> FEV~ of 113 ml <strong>with</strong> <strong>the</strong> addition of <strong>ipratropium</strong><br />
to <strong>salbutamol</strong> was less than anticipated but never<strong>the</strong>less<br />
atta<strong>in</strong>ed significance (p < 0.05), ma<strong>in</strong>ly as a result of <strong>the</strong><br />
improved accuracy of spirometry, which resulted <strong>in</strong> less<br />
variability <strong>in</strong> <strong>the</strong> measurement of FEV~. Performance of<br />
high-quality lung function test<strong>in</strong>g <strong>in</strong> patients <strong>with</strong> acute<br />
asthma is notoriously difficult <strong>and</strong> was achieved by