Nebulized salbutamol with and without ipratropium bromide in the ...
Nebulized salbutamol with and without ipratropium bromide in the ...
Nebulized salbutamol with and without ipratropium bromide in the ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Nebulized</strong> <strong>salbutamol</strong> <strong>with</strong> <strong>and</strong> <strong>with</strong>out<br />
<strong>ipratropium</strong> <strong>bromide</strong> <strong>in</strong> <strong>the</strong> treatment of<br />
acute asthma<br />
Jeffrey E. Garrett, MBChB, a G. lan Town, IVIBChB, b Peter Rodwell, MBChB, c <strong>and</strong><br />
Ann-Marie Kelly, MBChB d Auckl<strong>and</strong>, Christchurch, <strong>and</strong> Footscmy, New Zeal<strong>and</strong><br />
Background: Rout<strong>in</strong>e addition of <strong>ipratropium</strong> <strong>bromide</strong> to<br />
[g-agonist <strong>the</strong>rapy <strong>in</strong> acute asthma is of uncerta<strong>in</strong> benefit.<br />
Objective: This study was carried out to evaluate: (1)<br />
whe<strong>the</strong>r nebulized <strong>ipratropium</strong> (0.5 mg) plus <strong>salbutamol</strong><br />
(2.5 rag) (Combivent) confers additional bronchodilation<br />
over nebulized <strong>salbutamol</strong> (2.5 rag) alone <strong>in</strong> patients <strong>with</strong><br />
acute asthma <strong>and</strong> (2) whe<strong>the</strong>r adjustment for prognostic<br />
<strong>in</strong>dicators of outcome <strong>in</strong>fluences any benefit seen <strong>with</strong> <strong>ipratropium</strong>.<br />
Methods: A double-bl<strong>in</strong>d, two-center, r<strong>and</strong>omized, s<strong>in</strong>gle-dose<br />
study was performed <strong>in</strong> 338 patients <strong>with</strong> asthma, aged 18 to<br />
55 years, who attended <strong>the</strong> emergency department for treatment<br />
of acute asthma. The primary end po<strong>in</strong>t was FEV l at<br />
90 m<strong>in</strong>utes.<br />
Results: The mean absolute difference <strong>in</strong> FEV 1 at 90 m<strong>in</strong>utes<br />
for Combivent compared <strong>with</strong> <strong>salbutamol</strong> was 113 ml<br />
(SEM -+ 48 mi, p < 0.05). Independent of <strong>the</strong> study drug<br />
received, a poor response to treatment was predicted by<br />
frequent use of <strong>in</strong>haled [3-agonist before presentation (p <<br />
0.0001), severity of <strong>the</strong> attack (p < 0.05), <strong>and</strong> longer duration<br />
of attack (p < 0.05). Subjects who had taken more<br />
than 10 puffs of <strong>in</strong>haled [~-agonist through a metered-dose<br />
<strong>in</strong>haler or who had serum <strong>salbutamol</strong> levels of greater<br />
than 2 mmol/L on presentation demonstrated no benefit<br />
from <strong>the</strong> addition of <strong>ipratropium</strong>. Patients <strong>with</strong> an FEV 1<br />
less than 1 L on presentation also responded less well to<br />
Combivent, which was expla<strong>in</strong>ed by <strong>the</strong> association between<br />
severity of attack <strong>and</strong> greater use of <strong>in</strong>haled 13-agonist<br />
<strong>the</strong>rapy.<br />
Conclusion: A s<strong>in</strong>gle dose of nebulized Combivent confers<br />
additional bronchodilation over <strong>salbutamol</strong> alone (p < 0.05)<br />
<strong>in</strong> acute asthma. Patients who exhibited most benefit from<br />
<strong>the</strong> addition of <strong>ipratropium</strong> were those who had consumed<br />
<strong>the</strong> least <strong>in</strong>haled [3-agonist before presentation, not those<br />
<strong>with</strong> <strong>the</strong> most severe asthma. (J Allergy Cl<strong>in</strong> Immunol 1997;<br />
100:165-70.)<br />
Key words: Ipratropium <strong>bromide</strong>, <strong>salbutamol</strong>, acute severe<br />
asthma<br />
From ~<strong>the</strong> Department of Respirator 3' Services, Green Lane Hospital,<br />
Auckl<strong>and</strong>; bThe Canterbu U Respiratory Research Group, Christchurch;<br />
~Middlemore Hospital Emergency Department, Auckl<strong>and</strong>;<br />
<strong>and</strong> dEmergency Department, Western Hospital, Footscray.<br />
Work conducted <strong>in</strong> <strong>the</strong> Emergency Departments of Middlemore Hospital<br />
<strong>and</strong> Christchurch Hospital, New Zeal<strong>and</strong>.<br />
Supported by Boehr<strong>in</strong>ger Ingelheim Ltd.<br />
Received for publication Feb. 21, 1996; revised Dec. 11, 1996; accepted<br />
for publication Mar. 10, 1997.<br />
Repr<strong>in</strong>t requests: J. E. Garrett, Department of Respiratory Services,<br />
Green Lane Hospital, Private Bag, Auckl<strong>and</strong>, New Zeal<strong>and</strong>.<br />
Copyright © 1997 by Mosby-Year Book, lnc.<br />
0091-6749/97 $5.00 + 0 1/1/81778<br />
Abbreviations used<br />
ANCOVA: Analysis of covariance<br />
AFEV, 90: Change <strong>in</strong> FEV~ at 90 m<strong>in</strong>utes<br />
ED: Emergency department<br />
PEF: Peak expiratory flow<br />
International guidel<strong>in</strong>es recommend nebulized ~-agonist<br />
<strong>the</strong>rapy <strong>and</strong> corticosteroids <strong>in</strong> <strong>the</strong> management of<br />
acute severe asthma) ,2 Antichol<strong>in</strong>ergic drugs can be<br />
added to /3-agonists as <strong>in</strong>itial <strong>the</strong>rapy, particularly for<br />
patients <strong>with</strong> a severe episode, 2 or later if <strong>the</strong> <strong>the</strong>rapy<br />
fails. Several studies <strong>in</strong>dicate that additional bronchodilatation<br />
can be achieved by add<strong>in</strong>g <strong>ipratropium</strong> <strong>bromide</strong><br />
to <strong>salbutamol</strong> (albuterol) or fenoterol, 3q~ though <strong>in</strong> only<br />
four studies was this found to be statistically significant.<br />
12 Three studies have shown that patients <strong>with</strong> more<br />
severe asthma (FEV~ < 1 L, (', 13 peak expiratory flow<br />
[PEF] < 140 L/ra<strong>in</strong> 4) benefit most from <strong>the</strong> addition of<br />
<strong>ipratropium</strong> to ~3-agonist <strong>the</strong>rapy.<br />
The aim of this study was to evaluate <strong>the</strong> effects of<br />
nebulized <strong>ipratropium</strong> <strong>bromide</strong> solution <strong>in</strong> comb<strong>in</strong>ation<br />
<strong>with</strong> <strong>salbutamol</strong> sulfate (Combivent) <strong>in</strong> patients <strong>with</strong><br />
acute asthma, first seen <strong>in</strong> <strong>the</strong> emergency department<br />
(ED), to determ<strong>in</strong>e whe<strong>the</strong>r <strong>ipratropium</strong> augments <strong>the</strong><br />
bronchodilator effect of a s<strong>in</strong>gle dose of <strong>salbutamol</strong>.<br />
Those factors that best predicted extra benefit from <strong>the</strong><br />
addition of <strong>ipratropium</strong> were determ<strong>in</strong>ed, specifically to<br />
assess whe<strong>the</strong>r <strong>the</strong> greatest improvement occurred <strong>in</strong><br />
patients <strong>with</strong> <strong>the</strong> most severe asthma at presentation.<br />
METHODS<br />
Two New Zeal<strong>and</strong> EDs participated <strong>in</strong> a double-bl<strong>in</strong>d,<br />
r<strong>and</strong>omized, active-controlled, parallel-group study compar<strong>in</strong>g<br />
<strong>the</strong> bronchodilat<strong>in</strong>g effect of a fixed comb<strong>in</strong>ation of nebulized<br />
<strong>ipratropium</strong> (0.5 rag) <strong>and</strong> sa/butamol (2.5 rag) (Combjvent)<br />
<strong>with</strong> nebulized salbutamoI (2.5 mg) alone <strong>in</strong> patients <strong>with</strong> acute<br />
severe asthma.<br />
Patients<br />
Study participants were recruited from among patients <strong>with</strong><br />
asthma who attended <strong>the</strong> two participat<strong>in</strong>g EDs. Inclusion<br />
criteria were: age between 18 <strong>and</strong> 55 years, provision of<br />
witnessed <strong>in</strong>formed consent, ability to perform an adequate<br />
forced expiratory maneuver, <strong>and</strong> an FEV~ of less than 70% of<br />
predicted value. Exclusion criteria were: smok<strong>in</strong>g history of<br />
more than 10 pack-years, complicat<strong>in</strong>g medical illnesses such as<br />
chronic obstructive pulmonary disease (American Thoracic<br />
165
166 Garrett et al, J ALLERGY CLIN IMMUNOL<br />
AUGUST 1997<br />
FEV 1<br />
(ml)<br />
500 -<br />
400<br />
300<br />
200<br />
100<br />
Ii<br />
Ii<br />
'7<br />
i !<br />
i i i t I i<br />
15 30 45 60 75 90<br />
Time after start of nebulization (m<strong>in</strong>utes)<br />
* p
J ALLERGY CLIN IMMUNOL Garrett et alo 167<br />
VOLUME 100, NUMBER 2<br />
TABLE II. ANCOVA results<br />
Covariates<br />
Asthma medications <strong>in</strong> previous 6 hours<br />
ANCOVA IB + S Basel<strong>in</strong>e Duration Inhaled Inhaled Oral Inhaled Oral<br />
model no, vs S FEV 1 Age of attack 13-agonist IB <strong>the</strong>ophyll<strong>in</strong>e steroid steroid<br />
1 0.02 0.0007 . . . . . . .<br />
2 0.02 -- 0.05 . . . . . .<br />
3 0.04 -- -- 0.02 . . . . .<br />
4 0.08 -- -- -- 0.0001 . . . .<br />
5 0.03 . . . . 0.01 -- -- --<br />
6 0.03 . . . . . 0.2 -- --<br />
7 0.02 . . . . . . 0.8 --<br />
8 0.03 . . . . . . . O. I3<br />
9 0.21 0.01 0.08 0.02 0.0001 0.12 0.52 0.12 0.9<br />
10 0.16 0.01 0.07 0.02 0.0001 . . . .<br />
Probability (p) values are adjusted for prior asthma medication <strong>and</strong> basel<strong>in</strong>e measurements on AFEv I 90 from add<strong>in</strong>g <strong>ipratropium</strong> to 2.5 mg of<br />
salbutamoI. The analysis identified basel<strong>in</strong>e FEV~, age, [3-agonist use <strong>with</strong><strong>in</strong> 6 hours, <strong>and</strong> duration of attack as hav<strong>in</strong>g a significant impact on response<br />
to <strong>the</strong>rapy. Of <strong>the</strong>se, only [3-agonist use <strong>with</strong><strong>in</strong> 6 hours had any effect on <strong>the</strong> benefit of add<strong>in</strong>g IB to S (reduced top = 0.08).<br />
IB, Ipratropium <strong>bromide</strong>; S, salbutamoI.<br />
on outcome (AFEV!), <strong>and</strong> on <strong>the</strong> differential effect of Combivent<br />
versus <strong>salbutamol</strong> on AFEV~ 90.<br />
Fur<strong>the</strong>r analyses were <strong>the</strong>n undertaken to assess <strong>the</strong> effects<br />
of: (1) serum <strong>the</strong>ophyll<strong>in</strong>e <strong>and</strong> serum <strong>salbutamol</strong> levels <strong>in</strong><br />
patients tak<strong>in</strong>g <strong>the</strong>se medications; (2) an FEVf < 1 L <strong>and</strong> FEVI<br />
>_ 1 L on attendance; <strong>and</strong> (3) <strong>in</strong>haled [3-agonist use <strong>in</strong> <strong>the</strong><br />
previous 6 hours def<strong>in</strong>ed as 0, 1 to 9 puffs, <strong>and</strong> 10 puffs or more<br />
(1 nebulized 13-agonist was considered equivalent to 20 puffs<br />
through a metered-dose <strong>in</strong>haler) on <strong>the</strong> differential effect of<br />
Combivent <strong>and</strong> <strong>salbutamol</strong> on AFEV~ 90.<br />
Paired Student's t tests were used when appropriate to<br />
compare differences between means. Data were analyzed by<br />
us<strong>in</strong>g SAS software (version 6.08, SAS Institute).<br />
RESULTS<br />
A total of 338 of 442 patmnts screened entered <strong>the</strong><br />
study over a 542-day period. One center enrolled 231<br />
patients, <strong>and</strong> <strong>the</strong> o<strong>the</strong>r enrolled 107 patients. The most<br />
common reasons for exclusion of <strong>the</strong> 104 patients were<br />
an FEV~ greater than 70% of predicted value (73%) <strong>and</strong><br />
<strong>in</strong>ability to satisfactorily perform spirometry (19%).<br />
Fifty-n<strong>in</strong>e of 338 patients recruited <strong>in</strong>to <strong>the</strong> study were<br />
<strong>with</strong>drawn before <strong>the</strong> primary outcome measurement of<br />
FEV~ at 90 m<strong>in</strong>utes (AFEV~ 90) was obta<strong>in</strong>ed; 13<br />
requested early <strong>with</strong>drawal, (9 receiv<strong>in</strong>g Combivent <strong>and</strong><br />
4 receiv<strong>in</strong>g <strong>salbutamol</strong>), 45 were <strong>with</strong>drawn early by <strong>the</strong><br />
ED doctor because of a lack of satisfactory improvement<br />
(18 receiv<strong>in</strong>g Combivent <strong>and</strong> 27 receiv<strong>in</strong>g <strong>salbutamol</strong>),<br />
<strong>and</strong> one was <strong>with</strong>drawn before treatment was adm<strong>in</strong>istered<br />
because he was unable to provide blood samples.<br />
The mean age (2 SEM) of <strong>the</strong> 338 patients was 29.5 +<br />
0.7 years; 60.7% were female, 55.9% European, 17.2%<br />
Maori, 24.3% Pacific Isl<strong>and</strong>, <strong>and</strong> 2.6% Asian. There was<br />
no significant difference between <strong>the</strong> treatment groups<br />
for any of <strong>the</strong> demographic or cl<strong>in</strong>ical variables measured<br />
(Table I). FEV~ at basel<strong>in</strong>e revealed a difference<br />
of 40 + 57 ml <strong>in</strong> favor of Combivent (p = 0.4485).<br />
Analysis of change <strong>in</strong> FEV t from basel<strong>in</strong>e, as well as<br />
<strong>in</strong>corporation of basel<strong>in</strong>e FEV l as a covariate <strong>in</strong> <strong>the</strong><br />
statistical model, ensured that <strong>the</strong>re was no effect on <strong>the</strong><br />
primary efficacy end po<strong>in</strong>t from this small difference.<br />
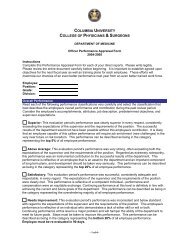
The mean absolute difference <strong>in</strong> change <strong>in</strong> FEV~ at 45<br />
m<strong>in</strong>utes was 93 + 24 ml (p = 0.03) <strong>and</strong> at 90 m<strong>in</strong>utes<br />
113 _+ 18 ml (p = 0.02) <strong>in</strong> favor of <strong>the</strong> Combivent group<br />
when compared <strong>with</strong> <strong>the</strong> <strong>salbutamol</strong> group (Fig. 1).<br />
Most of <strong>the</strong> improvement <strong>in</strong> ei<strong>the</strong>r treatment group<br />
occurred by 45 m<strong>in</strong>utes <strong>with</strong> m<strong>in</strong>imal additional bronchodilation<br />
observed at 90 m<strong>in</strong>utes (37 ml Combivent,<br />
17 ml <strong>salbutamol</strong>).<br />
Eighty percent of patients reported us<strong>in</strong>g medications<br />
<strong>with</strong><strong>in</strong> 6 hours of presentation to <strong>the</strong> ED. Thirteen<br />
percent reported tak<strong>in</strong>g oral corticosteroids, 31.7% <strong>in</strong>haled<br />
corticosteroids (_+ cromolyn 2 ketotifen), 79.9%<br />
<strong>in</strong>haled 13-agonist, 10.1% oral <strong>the</strong>ophyll<strong>in</strong>e, <strong>and</strong> 7.4%<br />
<strong>in</strong>haled antichol<strong>in</strong>ergics.<br />
Independent of <strong>the</strong> study drug received, a poor response<br />
to treatment was predicted by frequent use of<br />
<strong>in</strong>haled [3-agonist <strong>in</strong> <strong>the</strong> 6 hours before presentation<br />
(p < 0.0001), severity of <strong>the</strong> attack (i.e., low basel<strong>in</strong>e<br />
FEV~) (p < 0.007), longer duration of attack (p < 0.05),<br />
<strong>and</strong> older age (p < 0.05) (Table II). Inclusion of<br />
covariates <strong>in</strong> <strong>the</strong> statistical model <strong>in</strong>corporat<strong>in</strong>g prior<br />
asthma medication reduced <strong>the</strong> importance of basel<strong>in</strong>e<br />
FEV~ as a covariate from ap value of 0.007 to ap value<br />
of 0.01 (model 9), even when oral <strong>the</strong>ophyll<strong>in</strong>e, <strong>in</strong>haled<br />
corticosteroids, oral corticosteroids, <strong>and</strong> <strong>in</strong>haled antichol<strong>in</strong>ergics<br />
were removed from analysis (model 10).<br />
Patients <strong>with</strong> more severe asthma on presentation, as<br />
def<strong>in</strong>ed by a lower FEV1, were less likely to show<br />
improvement after ei<strong>the</strong>r of <strong>the</strong> treatment regimens.<br />
Never<strong>the</strong>less, when adjustment was made for basel<strong>in</strong>e<br />
FEV~ <strong>in</strong> <strong>the</strong> ANCOVA model <strong>and</strong> when FEV~ was<br />
treated as a cont<strong>in</strong>uous variable, <strong>the</strong> advantage of Combivent<br />
over <strong>salbutamol</strong> rema<strong>in</strong>ed significant (p = 0.02)<br />
(model 1, Table I). Basel<strong>in</strong>e FEV~ was <strong>the</strong>n treated
168 Garrett et al. J ALLERGY CLIN IMMUNOI_<br />
AUGUST 1997<br />
A FEV~<br />
600 r~ Combivent<br />
Salbutamol<br />
500 * * P 1 L [254<br />
patients; 77% Combivent, 74% <strong>salbutamol</strong>]). Patients<br />
<strong>with</strong> an FEV 1 of less than 1 L exhibited only a small<br />
benefit from Combivent (359 _+ 56 ml) compared <strong>with</strong><br />
<strong>salbutamol</strong> alone (337 +_ 66 ml; difference = 22 ml [not<br />
significant]), whereas those <strong>with</strong> an FEVj -> 1 L exhibited<br />
a significant benefit from Combivent (522 _+ 44 ml)<br />
compared <strong>with</strong> <strong>salbutamol</strong> alone (346 + 38 ml; difference<br />
= 176 ml) (p < 0.005) (Fig. 2).<br />
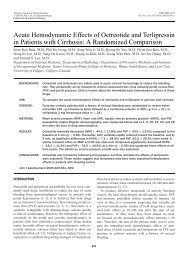
Sixty-six patients <strong>in</strong>dicated no prior use of an <strong>in</strong>haled<br />
[3-agonist. The 41 patients <strong>in</strong> <strong>the</strong> Combivent group had a<br />
mean &FEV~ 90 of 853 -+ 125 ml, which translated to a<br />
treatment difference of 315 + 135 ml <strong>in</strong> favor of<br />
Combivent over <strong>salbutamol</strong> (Fig. 3, A). Patients were<br />
<strong>the</strong>n grouped accord<strong>in</strong>g to <strong>in</strong>haled ~3-agonist <strong>in</strong>take <strong>in</strong><br />
<strong>the</strong> previous 6 hours or serum <strong>salbutamol</strong> levels (patients<br />
tak<strong>in</strong>g bricanyl or fenoterol were excluded from<br />
this analysis In = 50]) at basel<strong>in</strong>e before nebulization of<br />
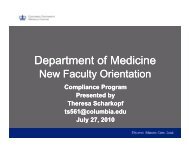
<strong>the</strong> study drugs (Fig. 3, B). Patients who had consumed<br />
<strong>the</strong> most {3-agonist before ED attendance exhibited a<br />
smaller <strong>in</strong>crease <strong>in</strong> FEV1 after adm<strong>in</strong>istration of nebulized<br />
bronchodilator <strong>and</strong> were least likely to show any<br />
benefit from <strong>the</strong> addition of Combivent (Fig. 3, A <strong>and</strong><br />
B).<br />
Although <strong>in</strong>haled <strong>ipratropium</strong> (7.4% of subjects)<br />
taken <strong>in</strong> <strong>the</strong> 6 hours before ED attendance appeared to<br />
<strong>in</strong>fluence AFEV~ 90 <strong>in</strong> <strong>the</strong> ANCOVA (Table I, model 5)<br />
(p = 0.01), <strong>the</strong> effect was nonsignificant (p = 0.12) when<br />
it was <strong>in</strong>cluded <strong>in</strong> <strong>the</strong> saturated model (model 9). This<br />
was expla<strong>in</strong>ed by <strong>the</strong> strong association between frequent<br />
<strong>in</strong>haled 13-agonist use <strong>and</strong> any <strong>in</strong>haled <strong>ipratropium</strong><br />
use before ED attendance. Oral <strong>the</strong>ophyll<strong>in</strong>e use, serum<br />
<strong>the</strong>ophyll<strong>in</strong>e at basel<strong>in</strong>e (for those tak<strong>in</strong>g <strong>the</strong>ophyll<strong>in</strong>e),<br />
<strong>and</strong> steroid use (<strong>in</strong>haled or oral) did not <strong>in</strong>fluence<br />
AFEV 1 90.<br />
There was no difference <strong>in</strong> mean heart rate, blood<br />
pressure, oxygen saturation, <strong>and</strong> respiratory rate between<br />
<strong>the</strong> treatment groups over <strong>the</strong> 90-m<strong>in</strong>ute study<br />
period; <strong>and</strong> <strong>the</strong>re were no differences <strong>in</strong> frequency of<br />
adverse events, apart from a somewhat greater need for<br />
A FEV 1<br />
(_+ SE) (ml)<br />
A<br />
900<br />
800<br />
700<br />
600<br />
500<br />
400<br />
300<br />
200<br />
100<br />
0<br />
i--i<br />
Nil 1 - 9 puffs _>10 puffs<br />
No. of puffs of <strong>in</strong>haled J3-Agonist <strong>in</strong> 6 hours prior to ED visit<br />
* * ( I Combivent<br />
r--1<br />
700 ~l<br />
6OO<br />
5OO<br />
zX FEV 1<br />
400<br />
(+ SE) (m0<br />
300<br />
B<br />
20O<br />
100<br />
0<br />
0 - 2 mmol/1 >2 mmol/1<br />
Serum Salbutamol level<br />
FIG. 3. A, Effect of <strong>in</strong>haled 13-agonist <strong>in</strong> previous 6 hours on response<br />
to Combivent compared <strong>with</strong> <strong>salbutamol</strong> at 90 m<strong>in</strong>utes (a nebulizer<br />
of 13-agonist was def<strong>in</strong>ed as 20 puffs through a metered-dose <strong>in</strong>haler).<br />
B, Effect of serum <strong>salbutamol</strong> level on presentation at ED on<br />
AFEV 1 90 (Combivent vs <strong>salbutamol</strong>) analyzed <strong>in</strong> patients who were<br />
tak<strong>in</strong>g <strong>in</strong>haled <strong>salbutamol</strong> or no 13-agonist (n = 271, 80%).<br />
hospitalization <strong>in</strong> <strong>the</strong> <strong>salbutamol</strong> treatment group<br />
(22.3%) compared <strong>with</strong> <strong>the</strong> Combivent group (15.3%,<br />
not significant).<br />
DISCUSSION<br />
Our data show that a significant improvement <strong>in</strong> lung<br />
function is associated <strong>with</strong> <strong>the</strong> addition of <strong>ipratropium</strong> to<br />
<strong>salbutamol</strong> (2.5 mg) <strong>in</strong> <strong>the</strong> <strong>in</strong>itial management of acute<br />
severe asthma. Fur<strong>the</strong>r, <strong>the</strong> improvement was achieved<br />
<strong>with</strong>out additional side effects or cardiovascular changes,<br />
<strong>in</strong>clud<strong>in</strong>g changes <strong>in</strong> pulse <strong>and</strong> blood pressure.<br />
The majority of previous studies had <strong>the</strong> potential for<br />
a large type II error <strong>and</strong> had wide confidence <strong>in</strong>tervals<br />
for pulmonary function outcome variables. 12 To avoid<br />
this, we estimated a study size of at least 326 patients to<br />
detect at <strong>the</strong> c~ = 0.05 significance level a 150 ml<br />
difference <strong>in</strong> FEV1 <strong>with</strong> 90% probability. The improvement<br />
<strong>in</strong> FEV~ of 113 ml <strong>with</strong> <strong>the</strong> addition of <strong>ipratropium</strong><br />
to <strong>salbutamol</strong> was less than anticipated but never<strong>the</strong>less<br />
atta<strong>in</strong>ed significance (p < 0.05), ma<strong>in</strong>ly as a result of <strong>the</strong><br />
improved accuracy of spirometry, which resulted <strong>in</strong> less<br />
variability <strong>in</strong> <strong>the</strong> measurement of FEV~. Performance of<br />
high-quality lung function test<strong>in</strong>g <strong>in</strong> patients <strong>with</strong> acute<br />
asthma is notoriously difficult <strong>and</strong> was achieved by
J ALLERGY CLIN IMMUNOL Garrett et al. 169<br />
VOLUME 100, NUMBER 2<br />
tra<strong>in</strong><strong>in</strong>g of research nurses <strong>and</strong> performance monitor<strong>in</strong>g<br />
by use of a spirometry quality control program.15 When<br />
possible, patients atta<strong>in</strong>ed a PEF time of less than 85<br />
msec (<strong>in</strong> 68% of <strong>in</strong>stances) <strong>and</strong> performed two measurements<br />
of FEV 1, which were <strong>with</strong><strong>in</strong> 5% or 100 ml of each<br />
o<strong>the</strong>r. As such, <strong>the</strong> spirometry quality control procedures<br />
were considerably more str<strong>in</strong>gent than <strong>the</strong> American<br />
Thoracic Society <strong>and</strong> Epidemiology St<strong>and</strong>ardization<br />
Project recommendations that were available at <strong>the</strong><br />
time of <strong>the</strong> study, is<br />
Three previous studies < (', 13 have shown that patients<br />
<strong>with</strong> <strong>the</strong> most severe asthma (PEF < 140 L/ra<strong>in</strong> 4, FEV 1<br />
< 1 L < 13) benefit more from <strong>the</strong> addition of <strong>ipratropium</strong><br />
<strong>bromide</strong>. Conversely, Roeseler et al. 3 found that patients<br />
<strong>with</strong> a PEF of less than 60 L/m<strong>in</strong> did not benefit as much.<br />
Our study shows that patients <strong>with</strong> <strong>the</strong> most severe<br />
asthma (FEV 1 < 1 L) derive less benefit from <strong>the</strong><br />
addition of <strong>ipratropium</strong> <strong>bromide</strong> to <strong>salbutamol</strong> (Fig. 2).<br />
This discrepancy is best expla<strong>in</strong>ed by differences <strong>in</strong> study<br />
design. Two of <strong>the</strong> earlier studies < 6 excluded patients<br />
who had received prior nebulized [3-agonist <strong>the</strong>rapy.<br />
Twenty-eight percent of our patients had been adm<strong>in</strong>istered<br />
a 13-agonist through a nebulizer before ED attendance,<br />
<strong>and</strong> <strong>the</strong>ir <strong>in</strong>clusion reflected a more pragmatic<br />
study design. Those who had used a nebulized 13-agonist<br />
<strong>with</strong><strong>in</strong> 6 hours of an ED visit not only had <strong>the</strong> most<br />
severe asthma on presentation I9 but were also less likely<br />
to benefit from <strong>the</strong> addition of any fur<strong>the</strong>r nebulized<br />
bronchodilator (Combivent or <strong>salbutamol</strong>) (Fig. 3, A<br />
<strong>and</strong> B).<br />
The majority of our patients had received asthma<br />
<strong>the</strong>rapy at home. This would be expected to <strong>in</strong>fluence<br />
<strong>the</strong> results of treatment received <strong>in</strong> <strong>the</strong> ED. Although<br />
plasma levels of <strong>the</strong>rophyll<strong>in</strong>e t3~2°,zl <strong>and</strong> 13-agonist2O,<br />
22.23 have been estimated at <strong>the</strong> time of arrival <strong>in</strong><br />
<strong>the</strong> ED <strong>in</strong> previous studies, little is known about <strong>the</strong> way<br />
<strong>the</strong> medication taken before arrival affects <strong>the</strong> outcome<br />
of acute asthma treatment. Although one study 22 <strong>in</strong>dicated<br />
no difference <strong>in</strong> <strong>the</strong> emergency treatment between<br />
patients who had or had not taken ~3-agonists before<br />
hospitalization, ano<strong>the</strong>r suggested that patients <strong>with</strong> <strong>the</strong><br />
highest plasma levels of {3-agonist on arrival do less well<br />
<strong>with</strong> nebulized 13-agonist <strong>the</strong>rapy than those <strong>with</strong> lower<br />
levels. 23 Patients who were tak<strong>in</strong>g oral <strong>the</strong>ophyll<strong>in</strong>e had<br />
<strong>the</strong> most severe asthma at presentation to <strong>the</strong> ED <strong>in</strong> our<br />
study. 19 The majority of patients who were tak<strong>in</strong>g <strong>the</strong>ophyll<strong>in</strong>e<br />
had sub<strong>the</strong>rapeutic levels <strong>and</strong> <strong>the</strong>ophyll<strong>in</strong>e use<br />
did not affect response to treatment (Table II). Conversely,<br />
those who had consumed <strong>the</strong> most <strong>in</strong>haled<br />
13-agonist <strong>and</strong> who had <strong>the</strong> highest serum 13-agonist<br />
levels not only had more severe asthma on arrival <strong>in</strong> <strong>the</strong><br />
ED 19 as Janson et al. 24 have shown but were also less<br />
likely to experience improvement <strong>with</strong> nebulized bronchodilator<br />
(ei<strong>the</strong>r Combivent or <strong>salbutamol</strong>) (Fig. 3, A<br />
<strong>and</strong> B, Table II). Fur<strong>the</strong>r, patients who had consumed<br />
more <strong>in</strong>haled 13-agonist before an ED visit derived less<br />
additional benefit from <strong>ipratropium</strong>, <strong>and</strong> this suggests<br />
that <strong>the</strong>re is a dose-response curve to <strong>in</strong>haled bronchodilators,<br />
whe<strong>the</strong>r <strong>ipratropium</strong> or <strong>salbutamol</strong>. This rema<strong>in</strong>s<br />
<strong>the</strong> most logical explanation for <strong>the</strong> smaller improvement<br />
<strong>in</strong> FEV 1 <strong>with</strong> <strong>the</strong> addition of <strong>ipratropium</strong> to<br />
<strong>salbutamol</strong> (113 ml) <strong>in</strong> our study than was predicted (150<br />
ml) from <strong>the</strong> study by Rebuck et al. ~ from which patients<br />
were excluded if <strong>the</strong>y had received nebulized 13-agonist<br />
before attendance. Presumably, those patients who still<br />
exhibit airway obstruction despite consum<strong>in</strong>g large doses<br />
of [3-agonist have an element of fixed airway obstruction<br />
or moderate to severe bronchial wall edema <strong>and</strong> airway<br />
mucus plugg<strong>in</strong>g <strong>and</strong> <strong>the</strong>refore ga<strong>in</strong> little extra benefit<br />
from <strong>the</strong> addition of <strong>ipratropium</strong>. One would have<br />
expected a muscar<strong>in</strong>ic receptor antagonist such as <strong>ipratropium</strong><br />
to confer additional benefit to those patients<br />
who had ga<strong>in</strong>ed maximum benefit from frequent adm<strong>in</strong>istration<br />
of <strong>in</strong>haled 13-agonists. However, this was not<br />
observed, <strong>and</strong> <strong>the</strong>refore our results do not support <strong>the</strong><br />
<strong>the</strong>ory that chol<strong>in</strong>ergic mechanisms are of greater importance<br />
<strong>in</strong> acute exacerbations of asthma. 25<br />
Conclusion<br />
Ipratropium augments <strong>the</strong> bronchodilator effect of a<br />
s<strong>in</strong>gle dose of <strong>salbutamol</strong> (2.5 rag). Patients who are first<br />
seen <strong>with</strong> severe acute asthma (low basel<strong>in</strong>e FEVI) <strong>and</strong><br />
who have consumed <strong>the</strong> greatest amount of <strong>in</strong>haled [3-agonist<br />
are least likely to derive benefit from <strong>the</strong> addition of<br />
<strong>ipratropium</strong>, which does not support <strong>the</strong> use of <strong>ipratropium</strong><br />
as second-l<strong>in</strong>e treatment if patients fail to respond<br />
adequately to treatment <strong>with</strong> high-dose <strong>in</strong>haled [3-agonist.<br />
More studies exam<strong>in</strong><strong>in</strong>g multiple dos<strong>in</strong>g of <strong>ipratropium</strong> <strong>in</strong><br />
addition to <strong>salbutamol</strong> need to be performed to assess<br />
whe<strong>the</strong>r <strong>the</strong> improvement <strong>in</strong> lung function from a s<strong>in</strong>gle<br />
dose translates <strong>in</strong>to cl<strong>in</strong>ically important differences <strong>in</strong> outcome<br />
such as hospitalization.<br />
We thank <strong>the</strong> research nurses at <strong>the</strong> Middlemore Hospital<br />
<strong>and</strong> Christchurch Hospital Emergency Departments for <strong>the</strong>ir<br />
careful collection of data. We also thank Larry Johnson, PhD,<br />
for devis<strong>in</strong>g <strong>the</strong> computerized quality assurance program used<br />
<strong>in</strong> perform<strong>in</strong>g spirometry <strong>in</strong> <strong>the</strong> ED, Ms. Helen ReiIIy from<br />
Boehr<strong>in</strong>ger [ngelheim Ltd. for her professional guidance as<br />
Trials Monitor, <strong>and</strong> Ms. Margaret McK<strong>in</strong>lay for secretarial<br />
assistance.<br />
REFERENCES<br />
1. British Thoracic Society. Guidel<strong>in</strong>es for management of asthma.<br />
Thorax 1993;48:SI-24.<br />
2. Asthma Management H<strong>and</strong>book 1996. National Asthma Campaign<br />
Ltd. Australia. p. 32-5.<br />
3. Roeseler J, Reynaert MS. A comparison of fenoterol <strong>and</strong> fenoterol<strong>ipratropium</strong><br />
nebulisation treatment <strong>in</strong> acute asthma. Acta Therapeutica<br />
1987;13:5714.<br />
4. O'Driscoll BR, Taylor RJ, Horsley MG, Chambers DK, Bernste<strong>in</strong> A.<br />
Nebulised salbutamoI <strong>with</strong> <strong>and</strong> <strong>with</strong>out <strong>ipratropium</strong> <strong>bromide</strong> <strong>in</strong><br />
acute airflow obstruction. Lancet 1989;1:1418-20.<br />
5. Watson WTA, Becker AB, Simons FER. Comparison of <strong>ipratropium</strong><br />
solution, fenoterol solution <strong>and</strong> <strong>the</strong>ir comb<strong>in</strong>ation adm<strong>in</strong>istered<br />
by nebulizer <strong>and</strong> free mask to children <strong>with</strong> acute asthma. J<br />
Allergy Cl<strong>in</strong> lmmunol 1988;82:1012-8.<br />
6. Rebuck AS, Chapman KR, Aboud R, Pare PD, Kreisman H,<br />
Wolkove N, Vickerson F. Nebulised antichoI<strong>in</strong>ergic <strong>and</strong> sympathomimetic<br />
treatment of asthma <strong>and</strong> chronic obstructive airways disease<br />
<strong>in</strong> <strong>the</strong> emergency room. Am J Med 1987;82:59-64.
170 Garrett et al. J ALLERGY CLIN IMMUNOL<br />
AUGUST 1997<br />
7. Leahy B, Gomm SA, Cullen SC. Comparison of nebulised salbutatool<br />
<strong>with</strong> nebulised <strong>ipratropium</strong> <strong>bromide</strong> <strong>in</strong> acute asthma. Br J Dis<br />
Chest 1983;77:159-63.<br />
8. Higg<strong>in</strong>s RM, Stradl<strong>in</strong>g JR, Lane DM. Should <strong>ipratropium</strong> <strong>bromide</strong><br />
be added to beta-agonists <strong>in</strong> <strong>the</strong> treatment of acute severe asthma?<br />
Chest 1988;94:718+22.<br />
9. Summers QA, Tarala R. Nebulised <strong>ipratropium</strong> <strong>in</strong> <strong>the</strong> treatment of<br />
acute asthma. Chest 1990;97:430-4.<br />
10. Ward MJ, Fentem PH, Smith WHR, Davies D. lpratropium <strong>bromide</strong><br />
<strong>in</strong> acute asthma. Br Med J I981;282:598-600.<br />
11. Bryant D. Nebulised <strong>ipratropium</strong> <strong>bromide</strong> <strong>in</strong> <strong>the</strong> treatment of acute<br />
asthma. Chest 1988;88:24-8.<br />
12. Ward MJ. The role of antichol<strong>in</strong>ergic drugs <strong>in</strong> acute asthma. In:<br />
Cross NJ, editor. Antichol<strong>in</strong>ergic <strong>the</strong>rapy <strong>in</strong> obstructive airways<br />
disease. London: Frankl<strong>in</strong> Scientific Publications; 1993. p. 155-62.<br />
13. Ross<strong>in</strong>g TH, Fanta CH, McFadden ER. A controlled trial of <strong>the</strong> use<br />
of s<strong>in</strong>gle versus comb<strong>in</strong>ed drug <strong>the</strong>rapy <strong>in</strong> <strong>the</strong> treatment of acute<br />
episodes of asthma. Am Rev Respir Dis 198l;123:190-4.<br />
14. St<strong>and</strong>ards for <strong>the</strong> diagnosis <strong>and</strong> care of patients <strong>with</strong> chronic<br />
obstructive pulmonary disease (COPD) <strong>and</strong> asthma. Am Rev Respir<br />
Dis 1987;136:225-44.<br />
15. Enright PL, Johnson LR, Connett JE, Voelker H, Buist AS. Spirometry<br />
<strong>in</strong> <strong>the</strong> Lung Health Study. 1. Methods <strong>and</strong> quality control. Am<br />
Rev Respir Dis 1991;143:1215-23.<br />
16. Crapo RO, Morris AH, Gardner RM. Reference spirometric values<br />
us<strong>in</strong>g techniques <strong>and</strong> equipment that meet ATS recommendations.<br />
Am Rev Respir Dis 1981;123:659-64.<br />
17. Macfie AE, Harris EA, Whitlock RML. The maximal expiratory<br />
flow/volume curve <strong>in</strong> 197 healthy New Zeal<strong>and</strong>ers: a comparison<br />
<strong>with</strong> recent American st<strong>and</strong>ards. Aust N Z J Med 1981;11:517-21.<br />
18. Gardner RM, Hunk<strong>in</strong>son JL, Clausen JE, Crapo RO, Epler GR.<br />
St<strong>and</strong>ardization of spirometry: 1987 update. Official statement of<br />
<strong>the</strong> American Thoracic Society. Am Rev Respir Dis 1987;136:<br />
1285-98.<br />
19. Garrett J, Frankel A, Lanes S, Rodwell P, Kelly AM, Town GI.<br />
Factors predict<strong>in</strong>g severity <strong>and</strong> response to <strong>the</strong>rapy <strong>in</strong> acute asthma<br />
[abstract]. Am J Respir Crit Care Med 1995;151:A380.<br />
20. Boe J, Ljungholm K. Drug <strong>in</strong>take <strong>and</strong> plasma concentrations <strong>in</strong><br />
acute asthma. Respiration 1984;45:430-7.<br />
21. Fanta CH, Ross<strong>in</strong>g TH, McFadden ER. Emergency treatment of<br />
asthma. Am Med J 1982;72:416-22.<br />
22. Ross<strong>in</strong>g TH, Fanta CH, McFadden ER. The effect of outpatient<br />
treatment of asthma <strong>with</strong> beta-agonists on <strong>the</strong> response to sympathomimetics<br />
<strong>in</strong> an emergency room. Am J Med 1983;75:781-4.<br />
23. Boe J, Carlsson LG, Hetta L, Karlson B, Ljungholm K. Acute<br />
asthma-plasma levels <strong>and</strong> effect of terbutal<strong>in</strong>e IV <strong>in</strong>jections. Eur J<br />
Respir Dis 1985;67:261-8.<br />
24. Janson C, Boe J, Boman G, Mossberg B, Svedmyr N. Bronchodilator<br />
<strong>in</strong>take <strong>and</strong> plasma levels on admission for severe acute asthma. Eur<br />
Respir J 1992;5:80-5.<br />
25. Barns P, Belvisi MG, Mak JCW, Haddad EB, O'Connor B.<br />
Tiotropium <strong>bromide</strong>, a novel long-act<strong>in</strong>g muscar<strong>in</strong>ic antagonist<br />
for <strong>the</strong> treatment of obstructive airways disease. Life Sci 1995;56:<br />
853-9.<br />
Availability of Journal Back Issues<br />
As a service to our subscribers, copies of back issues of The Journal of Allergy <strong>and</strong> Cl<strong>in</strong>ical<br />
Immunology for <strong>the</strong> preced<strong>in</strong>g 5 years are ma<strong>in</strong>ta<strong>in</strong>ed <strong>and</strong> are available for purchase until<br />
<strong>in</strong>ventory is depleted from Mosby at a cost of $11.50 per issue. The follow<strong>in</strong>g quantity discounts are<br />
available: 25% off on quantities of 12 to 23, <strong>and</strong> one third off on quantities of 24 or more. Please<br />
write to Mosby-Year Book, Inc., Subscription Services, 11830 Westl<strong>in</strong>e Industrial Dr., St. Louis,<br />
MO 63146-3318, or call (800) 453-4351 or (314) 453-4351 for <strong>in</strong>formation on availability of<br />
particular issues. If unavailable from <strong>the</strong> publisher, photocopies of complete issues may be<br />
purchased from UMI, 300 N. Zeeb Rd., Ann Arbor, MI 48106 (313) 761-4700.