

wound-healing-reading-chapters
wound-healing-reading-chapters
wound-healing-reading-chapters

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
SRPS Volume 10, Number 7, Part 1<br />
Simmons 224 recommend immediate Z-plasty for the<br />
repair of curved lacerations. Borges 225 disagrees,<br />
arguing that (1) most lacerations go beyond the skin<br />
and therefore it is difficult to decide what may be<br />
viable tissue; (2) patients may not like a zigzag scar<br />
if they have not had an opportunity to compare it<br />
with the scar produced by linear closure; and (3)<br />
the risk of infection or hematoma after a traumatic<br />
laceration is greater than after elective scar revision.<br />
WOUND PREPARATION<br />
Local anesthesia in the face is induced with a<br />
dilute anesthetic solution injected at key points over<br />
the nerve to the <strong>wound</strong>ed area using a 25-gauge or<br />
smaller needle. 226 The syringe should be small and<br />
the pressure on the plunger no more than needed<br />
for a slow but steady flow.<br />
Traumatic <strong>wound</strong>s must be rid of all devitalized<br />
tissue and foreign material. Only minimal debridement<br />
is recommended in the head and neck<br />
because of the ample blood supply of the area and<br />
the mutilating consequences of overly aggressive<br />
debridement. After sharp debridement the <strong>wound</strong><br />
should be thoroughly cleansed with normal saline<br />
or with povidone iodine for antisepsis.<br />
If primary closure is contemplated, the <strong>wound</strong><br />
edges are trimmed to make them perpendicular to<br />
the bed. The exception is in hair-bearing areas,<br />
where they should parallel the hair shafts. Every<br />
effort should be made to preserve key anatomic<br />
landmarks—the vermilion border, eyelid, eyebrow,<br />
nostril, and auricular helix—by precisely aligning<br />
the <strong>wound</strong> edges during closure.<br />
SURGICAL TECHNIQUES<br />
Meticulous surgical technique is required to<br />
obtain an inconspicuous scar. Critical elements<br />
include the obliteration of dead space, layered tissue<br />
closure, and eversion of skin margins.<br />
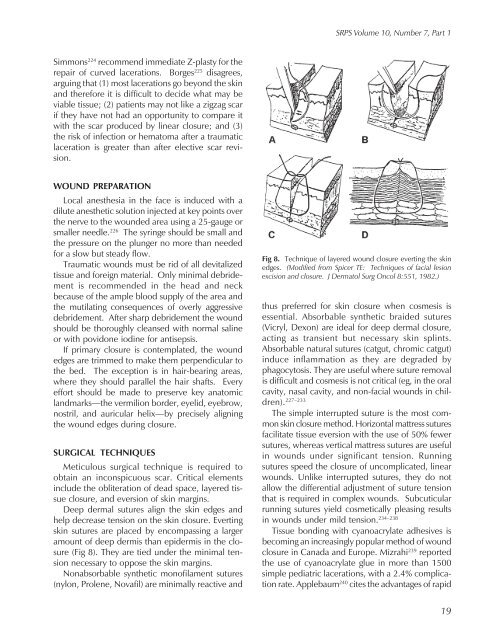
Deep dermal sutures align the skin edges and<br />
help decrease tension on the skin closure. Everting<br />
skin sutures are placed by encompassing a larger<br />
amount of deep dermis than epidermis in the closure<br />
(Fig 8). They are tied under the minimal tension<br />
necessary to oppose the skin margins.<br />
Nonabsorbable synthetic monofilament sutures<br />
(nylon, Prolene, Novafil) are minimally reactive and<br />
Fig 8. Technique of layered <strong>wound</strong> closure everting the skin<br />
edges. (Modified from Spicer TE: Techniques of facial lesion<br />
excision and closure. J Dermatol Surg Oncol 8:551, 1982.)<br />
thus preferred for skin closure when cosmesis is<br />
essential. Absorbable synthetic braided sutures<br />
(Vicryl, Dexon) are ideal for deep dermal closure,<br />
acting as transient but necessary skin splints.<br />
Absorbable natural sutures (catgut, chromic catgut)<br />
induce inflammation as they are degraded by<br />
phagocytosis. They are useful where suture removal<br />
is difficult and cosmesis is not critical (eg, in the oral<br />
cavity, nasal cavity, and non-facial <strong>wound</strong>s in children).<br />
227–233<br />
The simple interrupted suture is the most common<br />
skin closure method. Horizontal mattress sutures<br />
facilitate tissue eversion with the use of 50% fewer<br />
sutures, whereas vertical mattress sutures are useful<br />
in <strong>wound</strong>s under significant tension. Running<br />
sutures speed the closure of uncomplicated, linear<br />
<strong>wound</strong>s. Unlike interrupted sutures, they do not<br />
allow the differential adjustment of suture tension<br />
that is required in complex <strong>wound</strong>s. Subcuticular<br />
running sutures yield cosmetically pleasing results<br />
in <strong>wound</strong>s under mild tension. 234–238<br />
Tissue bonding with cyanoacrylate adhesives is<br />
becoming an increasingly popular method of <strong>wound</strong><br />
closure in Canada and Europe. Mizrahi 239 reported<br />
the use of cyanoacrylate glue in more than 1500<br />
simple pediatric lacerations, with a 2.4% complication<br />
rate. Applebaum 240 cites the advantages of rapid<br />
19