Authority for Authorised Pharmacist(s) to sign ... - Medicare website
Authority for Authorised Pharmacist(s) to sign ... - Medicare website
Authority for Authorised Pharmacist(s) to sign ... - Medicare website

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
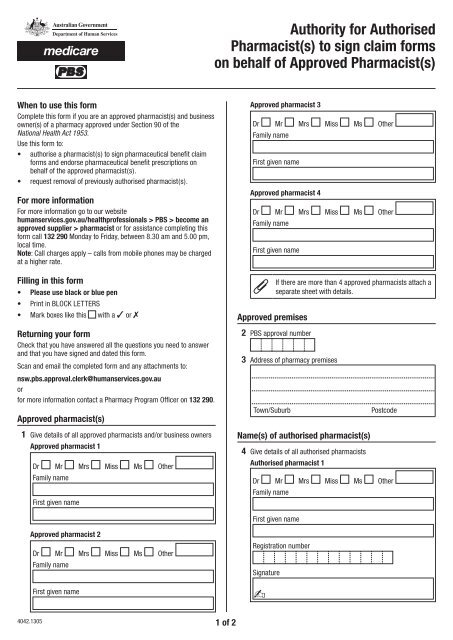
<strong>Authority</strong> <strong>for</strong> <strong>Authorised</strong><br />
<strong>Pharmacist</strong>(s) <strong>to</strong> <strong>sign</strong> claim <strong>for</strong>ms<br />
on behalf of Approved <strong>Pharmacist</strong>(s)<br />
When <strong>to</strong> use this <strong>for</strong>m<br />
Complete this <strong>for</strong>m if you are an approved pharmacist(s) and business<br />
owner(s) of a pharmacy approved under Section 90 of the<br />
National Health Act 1953.<br />
Use this <strong>for</strong>m <strong>to</strong>:<br />
• authorise a pharmacist(s) <strong>to</strong> <strong>sign</strong> pharmaceutical benefit claim<br />
<strong>for</strong>ms and endorse pharmaceutical benefit prescriptions on<br />
behalf of the approved pharmacist(s).<br />
• request removal of previously authorised pharmacist(s).<br />
For more in<strong>for</strong>mation<br />
For more in<strong>for</strong>mation go <strong>to</strong> our <strong>website</strong><br />
humanservices.gov.au/healthprofessionals > PBS > become an<br />
approved supplier > pharmacist or <strong>for</strong> assistance completing this<br />
<strong>for</strong>m call 132 290 Monday <strong>to</strong> Friday, between 8.30 am and 5.00 pm,<br />
local time.<br />
Note: Call charges apply – calls from mobile phones may be charged<br />
at a higher rate.<br />
Filling in this <strong>for</strong>m<br />
• Please use black or blue pen<br />
• Print in BLOCK LETTERS<br />
• Mark boxes like this with a ✓ or 7<br />
Approved pharmacist 3<br />
Dr Mr Mrs Miss Ms Other<br />
Family name<br />
First given name<br />
Approved pharmacist 4<br />
Dr Mr Mrs Miss Ms Other<br />
Family name<br />
First given name<br />
Approved premises<br />
If there are more than 4 approved pharmacists attach a<br />
separate sheet with details.<br />
Returning your <strong>for</strong>m<br />
Check that you have answered all the questions you need <strong>to</strong> answer<br />
and that you have <strong>sign</strong>ed and dated this <strong>for</strong>m.<br />
Scan and email the completed <strong>for</strong>m and any attachments <strong>to</strong>:<br />
nsw.pbs.approval.clerk@humanservices.gov.au<br />
or<br />
<strong>for</strong> more in<strong>for</strong>mation contact a Pharmacy Program Officer on 132 290.<br />
Approved pharmacist(s)<br />
2 PBS approval number<br />
3 Address of pharmacy premises<br />
Town/Suburb<br />
Postcode<br />
1 Give details of all approved pharmacists and/or business owners<br />
Approved pharmacist 1<br />
Dr Mr Mrs Miss Ms Other<br />
Family name<br />
First given name<br />
Name(s) of authorised pharmacist(s)<br />
4 Give details of all authorised pharmacists<br />
<strong>Authorised</strong> pharmacist 1<br />
Dr Mr Mrs Miss Ms Other<br />
Family name<br />
First given name<br />
Approved pharmacist 2<br />
Dr Mr Mrs Miss Ms Other<br />
Family name<br />
First given name<br />
Registration number<br />
Signature<br />
-<br />
4042.1305 1 of 2
<strong>Authorised</strong> pharmacist 2<br />
Dr Mr Mrs Miss Ms Other<br />
Family name<br />
First given name<br />
Registration number<br />
Signature<br />
-<br />
<strong>Authorised</strong> pharmacist 3<br />
Dr Mr Mrs Miss Ms Other<br />
Family name<br />
First given name<br />
Registration number<br />
Signature<br />
-<br />
<strong>Authorised</strong> pharmacist 4<br />
Dr Mr Mrs Miss Ms Other<br />
Family name<br />
First given name<br />
Registration number<br />
<strong>Authorised</strong> pharmacist name<br />
Declaration<br />
If there are more than 4 previously authorised<br />
pharmacists attach a separate sheet with details.<br />
6 I/we declare that:<br />
• the in<strong>for</strong>mation provided in this <strong>for</strong>m is complete and correct.<br />
• the dispensing of drugs and medicinal preparations will be<br />
per<strong>for</strong>med under the direct supervision of a pharmacist at the<br />
premises specified above, in accordance with Part VII of the<br />
National Health Act 1953 (the Act) and the regulation made<br />
under the Act.<br />
I/we understand that:<br />
• giving false or misleading in<strong>for</strong>mation is a serious offence.<br />
I/we authorise the pharmacist(s) whose <strong>sign</strong>ature(s) appear<br />
above, <strong>to</strong>:<br />
• <strong>sign</strong> pharmaceutical benefit claim <strong>for</strong>ms, and<br />
• endorse pharmaceutical benefit prescriptions on my/our behalf.<br />
Approved pharmacist 1<br />
Signature of approved pharmacist 1<br />
-<br />
Date / /<br />
Approved pharmacist 2<br />
Signature of approved pharmacist 2<br />
-<br />
Date / /<br />
Approved pharmacist 3<br />
Signature of approved pharmacist 3<br />
-<br />
Date / /<br />
Signature<br />
-<br />
If there are more than 4 authorised pharmacists attach<br />
a separate sheet with details.<br />
Previously authorised pharmacists<br />
5 Please list here any previously authorised pharmacists you wish<br />
<strong>to</strong> cancel<br />
<strong>Authorised</strong> pharmacist name<br />
<strong>Authorised</strong> pharmacist name<br />
<strong>Authorised</strong> pharmacist name<br />
4042.1305 2 of 2<br />
Approved pharmacist 4<br />
Signature of approved pharmacist 4<br />
-<br />
Date / /<br />
If more than 4 approved pharmacists <strong>sign</strong>atures are<br />
required attach a separate sheet with details.<br />
Privacy notice<br />
Your personal in<strong>for</strong>mation is protected by law, including the<br />
Privacy Act 1988, and is collected <strong>for</strong> a Social Security, Family<br />
Assistance, <strong>Medicare</strong>, Child Support and CRS purpose, depending<br />
on the service or payment concerned. This in<strong>for</strong>mation may be<br />
required by law or collected voluntarily when you apply <strong>for</strong> services or<br />
payments.<br />
Your in<strong>for</strong>mation is used <strong>for</strong> the assessment and administration of<br />
payments and services and may also be used within Human Services,<br />
or disclosed <strong>to</strong> other parties or agencies, where you have provided<br />
consent or it is required or authorised by law.<br />
You can get more in<strong>for</strong>mation about privacy by going <strong>to</strong> our <strong>website</strong><br />
humanservices.gov.au/privacy or requesting a copy of the full<br />
privacy policy at any of our Service Centres.