

Amputation surgery in the lower extremity
Amputation surgery in the lower extremity
Amputation surgery in the lower extremity

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
procedure. The author's preference is for an The posterior tibial vessels are secured,<br />
osteomyoplasty technique (Ertl, 1949) <strong>in</strong> all<br />
conditions o<strong>the</strong>r than vascular deficiency. In<br />
isolated and divided, and <strong>the</strong> nerve divided<br />
cleanly under light tension. The posterolater<br />
<strong>the</strong> dysvascular patient <strong>the</strong> posterior flap upon itself and sutured to a small cuff of<br />
procedure, Ghormley (1946), Burgess (1969), is periosteum elevated from <strong>the</strong> fibula. The<br />
appropriate to most cases. Increas<strong>in</strong>g experience is antero-medial likely to demonstrate osteo-periosteal <strong>the</strong> value flap of is <strong>the</strong>n<br />
<strong>the</strong> sagittal flap technique of Persson (1974)<br />
and o<strong>the</strong>r flaps designed <strong>in</strong>dividually for <strong>the</strong><br />
brought over <strong>the</strong> end of <strong>the</strong> tibia and sutured<br />
to <strong>the</strong> fibular periosteal cuff. Suture of <strong>the</strong> two<br />
patient.<br />
flaps is now completed form<strong>in</strong>g a ra<strong>the</strong>r firm<br />
osteo-periosteal tube bridg<strong>in</strong>g both bones<br />
(Figure 3). The anterior and posterior muscle<br />
Osteomyoplasty<br />
flaps are <strong>the</strong>n cut to length, trimmed, contoured and suture<br />
The procedure employed by <strong>the</strong> author is In <strong>the</strong> process <strong>the</strong> rema<strong>in</strong><strong>in</strong>g vessels and<br />
almost precisely that described by Loon (1962). nerves are isolated and dealt with. It is essential<br />
The level of operation when <strong>the</strong> pathology will that both groups of muscles are separately<br />
allow is usually just above <strong>the</strong> musculotend<strong>in</strong>ous anchored junction to <strong>the</strong> of periosteum <strong>the</strong> calf muscles. of <strong>the</strong> tibia Vertical and<br />
<strong>in</strong>cisions are made on <strong>the</strong> antero-lateral and<br />
postero-medial aspects of <strong>the</strong> stump distally<br />
to <strong>the</strong> base of <strong>the</strong> bridge. The two sk<strong>in</strong> flaps are<br />
now carefully tailored and sutured over <strong>the</strong><br />
from a po<strong>in</strong>t about 25 mm above <strong>the</strong> anticipated muscles level of of <strong>the</strong> bone stump. section. Closed With suction <strong>the</strong> need dra<strong>in</strong>age to<br />
expose some 75-100 mm of tibia below <strong>the</strong> is employed, <strong>the</strong> wound dressed and a rigid<br />
anticipated level of ultimate bone section two cast applied.<br />
vertical <strong>in</strong>cisions are carried down far enough<br />
to permit this and are jo<strong>in</strong>ed by a circular<br />
<strong>in</strong>cision. The two flaps thus formed are elevated<br />
subcutaneously to ensure an <strong>in</strong>tact deep fascia<br />
and muscle aponeurosis. A vertical cut is made<br />
through <strong>the</strong> deep fascia of <strong>the</strong> limb just lateral<br />
to <strong>the</strong> anterior tibial crest avoid<strong>in</strong>g <strong>the</strong><br />
periosteum. A fur<strong>the</strong>r vertical <strong>in</strong>cision is made<br />
through <strong>the</strong> deep fascia overly<strong>in</strong>g <strong>the</strong> fibula.<br />
The whole of <strong>the</strong> anterior lateral group of<br />
muscles <strong>in</strong>clud<strong>in</strong>g <strong>the</strong> peroneals is <strong>the</strong>n elevated<br />
by sharp dissection from <strong>the</strong> distal part of <strong>the</strong><br />
operative field from <strong>the</strong> bed formed by <strong>the</strong><br />
tibia with its overly<strong>in</strong>g periosteum, <strong>in</strong>terosseous<br />
membrane and fibula, to a po<strong>in</strong>t just proximal<br />
to <strong>the</strong> level of bone section. The posterior<br />
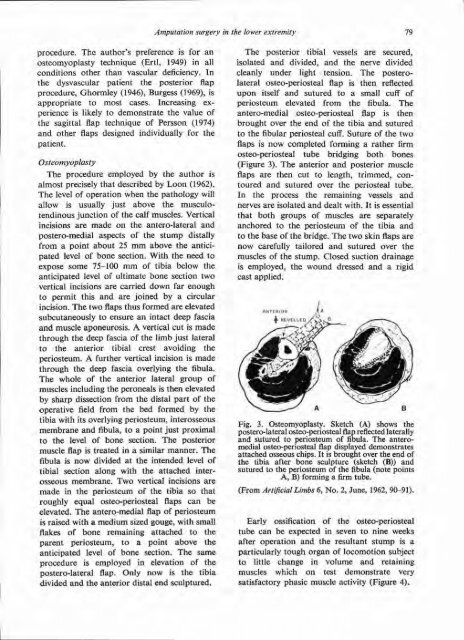
muscle flap is treated <strong>in</strong> a similar manner. The Fig. 3. Osteomyoplasty. Sketch (A) shows <strong>the</strong><br />
fibula is now divided at <strong>the</strong> <strong>in</strong>tended level of<br />
postero-lateral osteo-periosteal flap reflected laterally<br />
and sutured to periosteum of fibula. The anterome<br />
tibial section along with <strong>the</strong> attached <strong>in</strong>terosseous attached chips. membrane. It is brought Two over vertical <strong>the</strong> end <strong>in</strong>cisions of are<br />
made <strong>in</strong> <strong>the</strong> periosteum of <strong>the</strong> tibia so that<br />
roughly equal osteo-periosteal flaps can be<br />
elevated. The antero-medial flap of periosteum<br />
is raised with a medium sized gouge, with small<br />
flakes of bone rema<strong>in</strong><strong>in</strong>g attached to <strong>the</strong><br />
parent periosteum, to a po<strong>in</strong>t above <strong>the</strong><br />
anticipated level of bone section. The same<br />
procedure is employed <strong>in</strong> elevation of <strong>the</strong><br />
postero-lateral flap. Only now is <strong>the</strong> tibia<br />
divided and <strong>the</strong> anterior distal end sculptured.<br />
<strong>the</strong> tibia after bone sculpture (sketch (B)) and<br />
sutured to <strong>the</strong> periosteum of <strong>the</strong> fibula (note po<strong>in</strong>ts<br />
A, B) form<strong>in</strong>g a firm tube.<br />
(From Artificial Limbs 6, No. 2, June, 1962, 90-91).<br />
Early ossification of <strong>the</strong> osteo-periosteal<br />
tube can be expected <strong>in</strong> seven to n<strong>in</strong>e weeks<br />
after operation and <strong>the</strong> resultant stump is a<br />
particularly tough organ of locomotion subject<br />
to little change <strong>in</strong> volume and reta<strong>in</strong><strong>in</strong>g<br />
muscles which on test demonstrate very<br />
satisfactory phasic muscle activity (Figure 4).













