Compliance Notification Form - Office of the State Comptroller - CT.gov
Compliance Notification Form - Office of the State Comptroller - CT.gov
Compliance Notification Form - Office of the State Comptroller - CT.gov

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>State</strong> <strong>of</strong> Connecticut<br />
Health Enhancement Program<br />
CO-1316 Revised 5/2012<br />
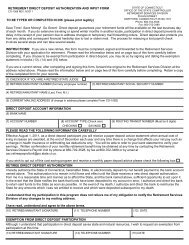
COMPLIANCE NOTIFICATION FORM<br />
<strong>State</strong> Of Connecticut<br />
<strong>Office</strong> <strong>of</strong> <strong>the</strong> <strong>State</strong> <strong>Comptroller</strong><br />
Healthcare Policy & Benefit Services Division<br />
55 Elm Street<br />
Hartford, <strong>CT</strong> 06106-1775<br />
www.osc.ct.<strong>gov</strong><br />
Important Information<br />
The Health Enhancement Program rewards members for taking steps to help maintain good health or to achieve greater<br />
health. One important step for members to remain eligible for program participation is to complete <strong>the</strong>ir regular health<br />
screenings. There may be times when claims data is not available to identify a member’s completion <strong>of</strong> a requirement.<br />
This form should be used to report information for those times where data was unavailable, but a requirement was in fact<br />
already completed. There may also be times when a requirement cannot be completed due to medical reasons. If a<br />
requirement cannot be met due to a special circumstance medical condition (for example, pregnancy, etc.) or if it is<br />
medically unadvisable, you may also use this form to request an exemption.<br />
If you were not notified <strong>of</strong> missing HEP requirements, <strong>the</strong>n you do not need to use this form. Your health plan will<br />
be able to automatically identify your completion <strong>of</strong> a requirement through claims submitted by your physician or provider.<br />
INSTRU<strong>CT</strong>IONS FOR MEMBERS: Please complete <strong>the</strong> Member Information and <strong>the</strong> Provider Information sections <strong>of</strong> this<br />
form. Please self-report your completion or scheduled completion <strong>of</strong> a physician visit or screening on page 2. Once<br />
completed, please submit forms as noted below. Your form will be processed within 15 business days from receipt as<br />
long as all required information is submitted. If you have questions regarding this form or <strong>the</strong> HEP program, please<br />
contact your <strong>State</strong>-dedicated Member Services Department on <strong>the</strong> back <strong>of</strong> your medical carrier’s ID card.<br />
Submit completed <strong>Compliance</strong> <strong>Notification</strong> forms to: Healthcare Analysis Unit, <strong>Office</strong> <strong>of</strong> <strong>the</strong> <strong>State</strong> <strong>Comptroller</strong>, 55<br />
Elm Street, Hartford, <strong>CT</strong> 06106 or fax to: (860) 702-3556.<br />
If your reported screening was processed through insurance outside <strong>of</strong> your state-sponsored health coverage or<br />
if you are requesting an exemption you MUST also submit a Physician <strong>Notification</strong> form to your medical carrier.<br />
Member Information (Required and must match exactly to what is listed on your Medical/Dental Plan ID card.)<br />
Employee ID<br />
Employee Last Name Employee First Name Middle Initial Date <strong>of</strong> Birth (MM/DD/YYYY)<br />
/ /<br />
Spouse Last Name Spouse First Name Middle Initial<br />
Home Address – Number and Street Name City <strong>State</strong> Zip Code<br />
Telephone<br />
( ) -<br />
Email Address<br />
Medical Provider Information (Required)<br />
Provider Name / Name <strong>of</strong> Clinic Provider ID # (If Applicable) Telephone Fax<br />
( ) - ( ) -<br />
<strong>Office</strong> Address – Number and Street Name City <strong>State</strong> Zip Code<br />
Dental Provider Information (If Applicable)<br />
Dentist / Provider <strong>Office</strong> Name Provider ID # (If Applicable) Telephone Fax<br />
( ) - ( ) -<br />
<strong>Office</strong> Address – Number and Street Name City <strong>State</strong> Zip Code
<strong>State</strong> <strong>of</strong> Connecticut – HEP – <strong>Compliance</strong> <strong>Notification</strong> <strong>Form</strong><br />
Page 2 <strong>of</strong> 2<br />
Employee/Spouse Last Name Employee/Spouse First Name Middle Initial Date <strong>of</strong> Birth (MM/DD/YYYY)<br />
/ /<br />
Place Check Mark in Each<br />
Applicable Box<br />
Service or<br />
Appointment<br />
Date<br />
(MM/DD/YY)<br />
Completed/Scheduled Screening<br />
Future<br />
Appointment<br />
Scheduled<br />
Already<br />
Completed<br />
Already Completed<br />
Processed With Coverage<br />
Outside <strong>of</strong> <strong>State</strong>-Sponsored<br />
Medical or Dental Insurance<br />
Exempted<br />
from<br />
Screening<br />
Preventive Well Visit Exam<br />
Cholesterol Screening<br />
Once every: 5 years (ages 20-29),<br />
3 years (ages 30-39), 2 years<br />
(ages 40-49) and every year (ages<br />
50+)<br />
/ /<br />
/ /<br />
I understand that I am responsible for submitting a<br />
completed Physician <strong>Notification</strong> <strong>Form</strong> to be<br />
considered compliant with HEP requirements.<br />
I understand that I am responsible for submitting a<br />
completed Physician <strong>Notification</strong> <strong>Form</strong> to be<br />
considered compliant with HEP requirements.<br />
Vision Exam<br />
(Adults 19 and older, every o<strong>the</strong>r<br />
year)<br />
Clinical Breast Exam<br />
(Females Only)<br />
Adults 18 and older, once every 3<br />
years<br />
Mammography<br />
Required for every female<br />
between <strong>the</strong> ages <strong>of</strong> 35 and 39 or<br />
as recommended by Physician<br />
/ /<br />
/ /<br />
/ /<br />
I understand that I am responsible for submitting a<br />
completed Physician <strong>Notification</strong> <strong>Form</strong> to be<br />
considered compliant with HEP requirements.<br />
I understand that I am responsible for submitting a<br />
completed Physician <strong>Notification</strong> <strong>Form</strong> to be<br />
considered compliant with HEP requirements.<br />
I understand that I am responsible for submitting a<br />
completed Physician <strong>Notification</strong> <strong>Form</strong> to be<br />
considered compliant with HEP requirements.<br />
Colorectal Cancer Screening<br />
Fecal Occult annually or<br />
Colonoscopy every 10 years<br />
Cervical Cancer Screening<br />
(ages 21+)<br />
One screening required every 3<br />
years<br />
/ /<br />
/ /<br />
I understand that I am responsible for submitting a<br />
completed Physician <strong>Notification</strong> <strong>Form</strong> to be<br />
considered compliant with HEP requirements.<br />
I understand that I am responsible for submitting a<br />
completed Physician <strong>Notification</strong> <strong>Form</strong> to be<br />
considered compliant with HEP requirements.<br />
Dental Cleaning(s)<br />
(If enrolled in a <strong>State</strong> dental plan)<br />
/ /<br />
I understand that I am responsible for submitting a<br />
completed Physician <strong>Notification</strong> <strong>Form</strong> to be<br />
considered compliant with HEP requirements.<br />
Employee/Spouse or Parent/Legal Guardian Signature<br />
Date<br />
X_____________________________________________________________<br />
/ /