Spine Questionnaire
Spine Questionnaire
Spine Questionnaire

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
( Please fill out this form and bring it to the appointment Name<br />
MR #<br />
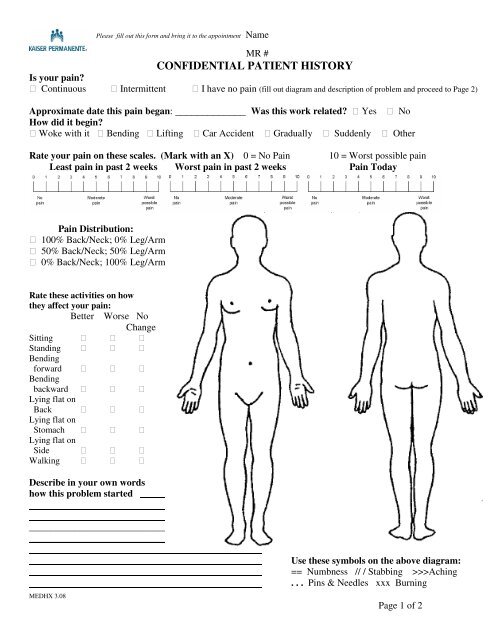
CONFIDENTIAL PATIENT HISTORY<br />
Is your pain?<br />
Continuous Intermittent I have no pain (fill out diagram and description of problem and proceed to Page 2)<br />
Approximate date this pain began: _____________ Was this work related? Yes No<br />
How did it begin?<br />
Woke with it Bending Lifting Car Accident Gradually Suddenly Other<br />
Rate your pain on these scales. (Mark with an X) 0 = No Pain 10 = Worst possible pain<br />
Least pain in past 2 weeks Worst pain in past 2 weeks Pain Today<br />
Pain Distribution:<br />
100% Back/Neck; 0% Leg/Arm<br />
50% Back/Neck; 50% Leg/Arm<br />
0% Back/Neck; 100% Leg/Arm<br />
Rate these activities on how<br />
they affect your pain:<br />
Better Worse No<br />
Change<br />
Sitting <br />
Standing <br />
Bending<br />
forward <br />
Bending<br />
backward <br />
Lying flat on<br />
Back <br />
Lying flat on<br />
Stomach <br />
Lying flat on<br />
Side <br />
Walking <br />
Describe in your own words<br />
how this problem started<br />
______<br />
_____________________________________________________________________________<br />
_____________________________________________<br />
MEDHX 3.08<br />
Use these symbols on the above diagram:<br />
== Numbness // / Stabbing >>>Aching<br />
. . . Pins & Needles xxx Burning<br />
Page 1 of 2
( Please fill out this form and bring it to the appointment Name<br />
MR #<br />
MEDICAL HISTORY. CHECK, CIRCLE & FILL IN BLANKS THAT APPLY TO YOU<br />
Please indicate if you get all of your medications through Kaiser: Yes No<br />
If no, what other medications are you on: _________________________________________<br />
Check if you have or had any of these medical problems:<br />
Heart Attack High Blood Pressure Thyroid Disease<br />
Stroke Diabetes Arthritis<br />
Ulcers Kidney Disease Liver Disease<br />
Cancer ______________________________________________________________________<br />
List Type<br />
Dominant Hand Left Right<br />
SURGICAL HISTORY<br />
List all surgeries and dates:<br />
Type of Surgery Date Type of Surgery Date<br />
SOCIAL HISTORY<br />
Married Divorced<br />
Separated Widowed<br />
Live with significant other Never Married<br />
Habits: (check if you have or have ever had the following habits)<br />
Smoking Cigarettes: Age started ______<br />
Drinking Alcoholic Beverages:<br />
# of packs/day _______<br />
Age started __________<br />
Quit:___________________(when)<br />
Last drink ___________ (when)<br />
# of drinks/week ___________<br />
Are you:<br />
Currently Working Permanently Disabled<br />
Retired Temporarily Disabled<br />
WORK HISTORY<br />
Describe your job:<br />
REVIEW OF SYMPTOMS<br />
Persistent Fevers Night Sweats Weight Loss Joint Aches<br />
Sleep Problems Fatigue Depression Easy Bruising<br />
Excessive Bleeding Persistent Diarrhea Constipation Swollen Ankles<br />
Dark Stools Blood in Stool Difficulty Urinating Incontinence<br />
Explanation of above:<br />
MEDHX 3.08<br />
Page 2 of 2