Audiometry Form - Clas News and Publications
Audiometry Form - Clas News and Publications
Audiometry Form - Clas News and Publications

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
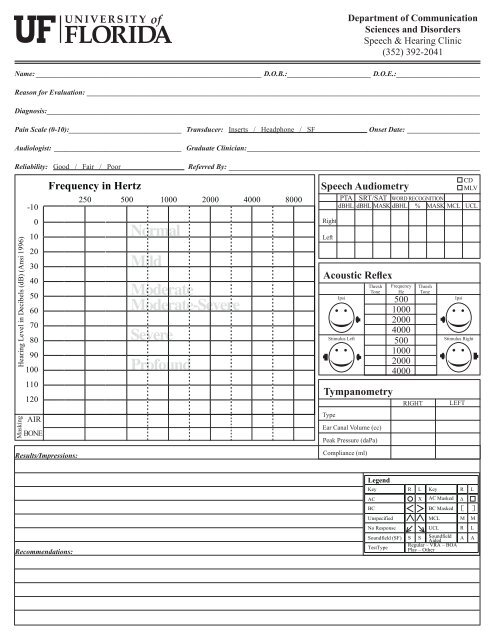
Department of Communication<br />
Sciences <strong>and</strong> Disorders<br />
Speech & Hearing Clinic<br />
(352) 392-2041<br />
Name:_______________________________________________________________ D.O.B.:_______________________ D.O.E.:_______________________<br />
Reason for Evaluation:_____________________________________________________________________________________________________________<br />
Diagnosis:_______________________________________________________________________________________________________________________<br />
Pain Scale (0-10):_______________________________ Transducer: Inserts / Headphone / SF<br />
Onset Date:_ ____________________<br />
Audiologist:_ ___________________________________ Graduate Clinician:_________________________________________________________________<br />
Reliability: Good / Fair / Poor<br />
Referred By:______________________________________________________________________<br />
CD<br />
MLV<br />
PTA SRT/SAT WORD RECOGNITION<br />
dBHL dBHL MASK dBHL % MASK MCL UCL<br />
Speech <strong>Audiometry</strong><br />
Normal<br />
Right<br />
Left<br />
Mild<br />
Moderate<br />
Moderate-Severe<br />
Severe<br />
Profound<br />
Acoustic Reflex<br />
Ipsi<br />
Stimulus Left<br />
Thresh<br />
Tone<br />
Frequency<br />
Hz<br />
500<br />
1000<br />
2000<br />
4000<br />
500<br />
1000<br />
2000<br />
4000<br />
Thresh<br />
Tone<br />
Ipsi<br />
Stimulus Right<br />
Tympanometry<br />
RIGHT<br />
LEFT<br />
Masking<br />
AIR<br />
BONE<br />
Type<br />
Ear Canal Volume (cc)<br />
Peak Pressure (daPa)<br />
Results/Impressions:<br />
Compliance (ml)<br />
Recommendations:
Department of Communication<br />
Sciences <strong>and</strong> Disorders<br />
Hearing & Speech Clinic<br />
(352) 273-0542<br />
Name:_______________________________________________________________ D.O.B.:_______________________ D.O.E.:_______________________<br />
Reason for Evaluation:_____________________________________________________________________________________________________________<br />
Diagnosis:_______________________________________________________________________________________________________________________<br />
Pain Scale (0-10):_______________________________ Transducer: Inserts / Headphone / SF<br />
Onset Date:_ ____________________<br />
Audiologist:_ ___________________________________ Graduate Clinician:_________________________________________________________________<br />
Reliability: Good / Fair / Poor<br />
Referred By:______________________________________________________________________<br />
CD<br />
MLV<br />
PTA SRT/SAT WORD RECOGNITION<br />
dBHL dBHL MASK dBHL % MASK MCL UCL<br />
Speech <strong>Audiometry</strong><br />
Normal<br />
Right<br />
Left<br />
Mild<br />
Moderate<br />
Moderate-Severe<br />
Severe<br />
Profound<br />
Acoustic Reflex<br />
Ipsi<br />
Stimulus Left<br />
Thresh<br />
Tone<br />
Frequency<br />
Hz<br />
500<br />
1000<br />
2000<br />
4000<br />
500<br />
1000<br />
2000<br />
4000<br />
Thresh<br />
Tone<br />
Ipsi<br />
Stimulus Right<br />
Tympanometry<br />
RIGHT<br />
LEFT<br />
Masking<br />
AIR<br />
BONE<br />
Type<br />
Ear Canal Volume (cc)<br />
Peak Pressure (daPa)<br />
Results/Impressions:<br />
Compliance (ml)<br />
Recommendations: