010401 Allergy and Allergic Diseases
010401 Allergy and Allergic Diseases
010401 Allergy and Allergic Diseases

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
The New Engl<strong>and</strong> Journal of Medicine<br />
Review Articles<br />
Advances in Immunology<br />
I AN R. MACKAY, M.D., AND FRED S. ROSEN, M.D.,<br />
Editors<br />
ALLERGY AND ALLERGIC DISEASES<br />
First of Two Parts<br />
A.B. KAY, M.D., PH.D.<br />
ALLERGIC rhinitis, asthma, <strong>and</strong> atopic eczema<br />
are among the commonest causes of chronic<br />
ill health. These diseases are increasing in prevalence,<br />
<strong>and</strong> they add considerably to the burden of<br />
health care costs. In Sweden, for example, the number<br />
of children with allergic rhinitis, asthma, or eczema<br />
roughly doubled over a 12-year period, 1 <strong>and</strong><br />
in the United States the annual cost of treating asthma<br />
is about $6 billion. 2<br />
The term “allergy” was introduced in 1906 by<br />
von Pirquet, who recognized that in both protective<br />
immunity <strong>and</strong> hypersensitivity reactions, antigens had<br />
induced changes in reactivity. 3 With the passage of<br />
time the word has become corrupted <strong>and</strong> is now frequently<br />
used synonymously with IgE-mediated allergic<br />
disease. It was von Pirquet’s intent that the term<br />
should apply to the “uncommitted” biologic response,<br />
which may lead either to immunity (a beneficial effect)<br />
or allergic disease (a harmful effect).<br />
The term “atopy” (from the Greek atopos, meaning<br />
out of place) is often used to describe IgE-mediated<br />
diseases. Persons with atopy have a hereditary predisposition<br />
to produce IgE antibodies against common<br />
environmental allergens <strong>and</strong> have one or more atopic<br />
diseases (i.e., allergic rhinitis, asthma, <strong>and</strong> atopic eczema).<br />
Some allergic diseases, such as contact dermatitis<br />
<strong>and</strong> hypersensitivity pneumonitis, develop<br />
through IgE-independent mechanisms <strong>and</strong> in this<br />
sense can be considered nonatopic allergic conditions.<br />
This article reviews the basis of atopic allergy, the<br />
diseases with which it is associated, <strong>and</strong> approaches<br />
to treatment.<br />
ATOPY AND TYPE 2 HELPER T CELLS<br />
All of us inhale aeroallergens derived from pollen,<br />
house-dust mites, <strong>and</strong> cat d<strong>and</strong>er. In general, adults<br />
From the Imperial College School of Medicine, National Heart <strong>and</strong><br />
Lung Institute, London.<br />
<strong>and</strong> children without atopy mount a low-grade immunologic<br />
response; they produce allergen-specific<br />
IgG1 <strong>and</strong> IgG4 antibodies, 4 <strong>and</strong> in vitro their T cells<br />
respond to the allergen with a moderate degree of proliferation<br />
<strong>and</strong> the production of interferon-g by type 1<br />
helper T (Th1) cells. 5-7 Persons with atopy, by contrast,<br />
have an exaggerated response characterized by<br />
the production of allergen-specific IgE antibodies;<br />
they have elevated serum levels of IgE antibodies <strong>and</strong><br />
positive reactions to extracts of common aeroallergens<br />
on skin-prick tests. T cells from their blood respond<br />
to allergens in vitro by inducing cytokines produced<br />
by type 2 helper T (Th2) cells (i.e., interleukin-4, 5,<br />
<strong>and</strong> 13), 5,7 rather than cytokines produced by Th1<br />
cells (interferon-g <strong>and</strong> interleukin-2). There are many<br />
exceptions to this rule, but the immunopathological<br />
hallmark of allergic disease is the infiltration of affected<br />
tissue by Th2 cells. 8-10<br />
In utero, T cells of the fetus are primed by common<br />
environmental allergens that cross the placenta.<br />
As a result, the immune response of virtually all newborn<br />
infants is dominated by Th2 cells. 11 It has been<br />
proposed that during subsequent development the<br />
normal (i.e., nonatopic) infant’s immune system shifts<br />
in favor of a Th1-mediated response to inhaled allergens<br />
(a process termed “immune deviation”), 12 whereas<br />
in the potentially atopic infant there is a further<br />
increase in Th2 cells that were primed in utero. Microbes<br />
are probably the chief stimuli of protective<br />
Th1-mediated immunity. Macrophages that engulf<br />
microbes secrete interleukin-12, which induces Th1<br />
cells <strong>and</strong> natural killer cells to produce interferon-g,<br />
thereby shifting the immune system into an “allergyprotective”<br />
Th1-mediated response. Other factors may<br />
also influence whether Th1 or Th2 cells dominate<br />
the response, including the amount of allergen, the<br />
duration of exposure to the allergen, <strong>and</strong> the avidity<br />
of allergen-specific interactions between T cells <strong>and</strong><br />
antigen-presenting cells 13,14 (Fig. 1).<br />
RISING INCIDENCE OF ALLERGIC<br />
DISEASE<br />
The marked increase in the prevalence of atopic<br />
disease in western Europe, the United States, <strong>and</strong><br />
Australasia during recent years indicates the importance<br />
of environmental influences. An informative<br />
example is the change in the incidence of seasonal<br />
allergic rhinitis <strong>and</strong> asthma after the reunification of<br />
Germany. These disorders were less common in East<br />
Germany than West Germany before reunification, 16<br />
whereas since reunification, the prevalence of atopy<br />
<strong>and</strong> hay fever, but not asthma, has increased among<br />
children who spent their early childhood in East Ger-<br />
30 · N Engl J Med, Vol. 344, No. 1 · January 4, 2001 · www.nejm.org<br />
Downloaded from www.nejm.org by VASSILAKOPOULOS THEODOROS MD on April 1, 2009 .<br />
Copyright © 2001 Massachusetts Medical Society. All rights reserved.
ADVANCES IN IMMUNOLOGY<br />
GATA-3<br />
c-maf<br />
PGE 2<br />
Nitric oxide<br />
Th2<br />
IFN-g<br />
High-affinity<br />
interactions<br />
between T cells <strong>and</strong><br />
antigen-presenting cells<br />
<br />
Large amount<br />
of antigen<br />
<br />
Interleukin-4 Interleukin-10 <strong>and</strong> TGF-b Interleukin-12<br />
Interleukin-18 <br />
Low-affinity<br />
interactions<br />
between T cells <strong>and</strong> <br />
antigen-presenting cells<br />
<br />
Small amount<br />
of antigen<br />
<br />
Th1<br />
CpG repeats from<br />
bacterial antigens<br />
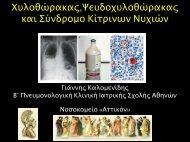
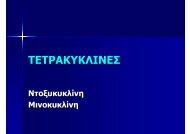
Figure 1. Immunologic <strong>and</strong> Cellular Factors Regulating the Expression of Th1 <strong>and</strong> Th2 Cells.<br />
Whether the immune response is dominated by Th1 or Th2 cells is dependent on interleukin-12 <strong>and</strong> interleukin-4, respectively, as<br />
well as on the avidity of interactions between T cells <strong>and</strong> antigen-presenting cells <strong>and</strong> the amount of allergen to which the immune<br />
system is exposed (antigen). 13,14 In addition, the presence of cytidine–phosphate–guanosine (CpG) repeats derived from bacteria<br />
favors the Th1 phenotype, whereas the presence of transcription factors such as GATA-3 favors the Th2 phenotype, 15 as does the<br />
presence of c-maf <strong>and</strong> prostagl<strong>and</strong>in E 2<br />
(PGE 2<br />
). Nitric oxide favors the expression of Th2 cells by being less inhibitory to Th2 cells<br />
than Th1 cells, whereas in humans interleukin-10 <strong>and</strong> transforming growth factor b (TGF-b) generally dampen the responses of both<br />
types of cells. Interferon-g (IFN-g) inhibits Th2-mediated responses; both interleukin-12 <strong>and</strong> interleukin-18 release interferon-g from<br />
T cells. Interleukin-4 inhibits the expression of Th1 cells <strong>and</strong> promotes Th2-mediated responses. Green arrows indicate stimulatory<br />
effects, <strong>and</strong> red arrows inhibitory effects, of the cytokines.<br />
many. 17 This phenomenon raises the possibility that<br />
a Western lifestyle accounts for the increases in prevalence.<br />
Perhaps in Western countries the developing<br />
immune system is deprived of the microbial antigens<br />
that stimulate Th1 cells, because the environment is<br />
relatively clean <strong>and</strong> the use of antibiotics for minor<br />
illnesses in early life is widespread. 18<br />
The results of epidemiologic studies support this<br />
theory. Evidence that the bacteria that colonize the<br />
gastrointestinal tract prevent atopic sensitization was<br />
found in studies of one-year-old infants in countries<br />
with a low prevalence of atopy (Estonia) <strong>and</strong> a high<br />
prevalence (Sweden). Lactobacilli <strong>and</strong> eubacteria predominated<br />
in Estonian infants, whereas clostridia were<br />
more frequent in Swedish infants. 19 When studied one<br />
year later, the children with atopy were colonized<br />
less often by lactobacilli <strong>and</strong> had higher levels of aerobic<br />
bacteria (such as coliforms <strong>and</strong> Staphylococcus aureus)<br />
than children without atopy. 20 Moreover, atopy<br />
<strong>and</strong> allergic asthma were less frequent in populations<br />
exposed to Helicobacter pylori, Toxoplasma gondii, <strong>and</strong><br />
hepatitis A virus. By producing an environment rich<br />
in interleukin-12, these microbes could drive a Th1-<br />
mediated response. This mechanism may explain why<br />
in Europe <strong>and</strong> Africa, farming or living in a rural<br />
community, which increases the likelihood of exposure<br />
to bacteria found in barns, protects against atopic<br />
disease. 21<br />
Other factors that may favor the Th2 phenotype<br />
in infants include diet <strong>and</strong> being born when pollen<br />
counts are high. 22 Furthermore, atopic allergic diseases<br />
are less common in younger children who have<br />
three or more older siblings <strong>and</strong> among children who<br />
have had measles or hepatitis A — another indication<br />
that repeated immune stimulation may protect against<br />
atopic allergy. 23 This view is supported by the study<br />
by Ball et al., who provided evidence that exposure<br />
of young children to older children at home or to<br />
other children at day-care centers protected against<br />
the development of asthma <strong>and</strong> frequent wheezing<br />
in childhood. 24<br />
This “hygiene” hypothesis is not easily reconciled<br />
N Engl J Med, Vol. 344, No. 1 · January 4, 2001 · www.nejm.org · 31<br />
Downloaded from www.nejm.org by VASSILAKOPOULOS THEODOROS MD on April 1, 2009 .<br />
Copyright © 2001 Massachusetts Medical Society. All rights reserved.
The New Engl<strong>and</strong> Journal of Medicine<br />
with the increased prevalence among poor blacks in<br />
the United States of atopic asthma associated with<br />
sensitization to cockroaches <strong>and</strong> house-dust mites. 25,26<br />
However, we need more data on the rates of infection<br />
by foodborne <strong>and</strong> orofecal microbes in inner<br />
cities in the United States: the compounding effect<br />
of gut flora that does not protect against atopy <strong>and</strong><br />
heavy exposure to allergens may explain this paradox.<br />
The development of specific allergic diseases may<br />
be related to alterations in the target organ. For example,<br />
the cofactors required for an asthma attack<br />
may include respiratory virus infections <strong>and</strong> exposure<br />
to allergens, tobacco smoke, <strong>and</strong> air pollutants. 27 These<br />
factors, alone or in combination, may alter immunoregulatory<br />
mechanisms at mucosal surfaces in ways<br />
that promote a Th2-mediated allergic inflammatory<br />
response (Fig. 2).<br />
ALLERGENS<br />
Many allergens are soluble proteins that function<br />
in their natural state as enzymes, by, for example, inducing<br />
proteolysis. Allergenic properties may be related<br />
to the enzymatic activity (e.g., increased mucosal<br />
permeability) <strong>and</strong> to aerodynamic properties, which<br />
in turn depend on the size of the particle. The major<br />
allergens of Western developed countries are Der p 1<br />
<strong>and</strong> Der p 2, from the house-dust mite (Dermatophagoides<br />
pteronyssinus); Fel d 1, from the cat (Felis domesticus);<br />
several tree allergens, including Bet v 1 from<br />
the birch tree (Betula verrucosa); <strong>and</strong> many grasses,<br />
such as Phl p 1 <strong>and</strong> Phl p 5 from timothy (Phleum<br />
pratense). The ragweed allergens Amb a 1, 2, 3, 5,<br />
<strong>and</strong> 6 from short ragweed (Ambrosia artemisiifolia)<br />
<strong>and</strong> Amb t 5 from giant ragweed (Ambrosia trifida)<br />
are important seasonal allergens in North America.<br />
Allergies to Hev b 1 through 7 from latex, the milky<br />
sap harvested from the rubber tree (Hevea brasiliensis),<br />
<strong>and</strong> Ara h 1, 2, <strong>and</strong> 3, which are highly allergenic peanut<br />
proteins, are increasingly important problems. 28<br />
GENETICS<br />
Atopic allergic diseases are familial <strong>and</strong> have a genetic<br />
basis. The difficulties of conducting genetic studies<br />
of allergy are due in part to the multiple markers<br />
for atopy <strong>and</strong> allergic diseases. For instance, atopy<br />
(manifested by positive skin-prick tests <strong>and</strong> elevated<br />
serum IgE levels) <strong>and</strong> asthma (manifested by airway<br />
hyperresponsiveness) are not always inherited togeth-<br />
Genetic Factors<br />
Presence of specific HLA alleles<br />
Polymorphisms of FceRI-b<br />
Polymorphisms of the interleukin-4 <br />
family of cytokine genes <br />
Polymorphism of CD14<br />
Polymorphisms at other loci<br />
<br />
Environmental Factors<br />
Allergen sensitization<br />
Having few siblings<br />
Excessive hygiene<br />
Receipt of antibiotics in first <br />
2 years of life<br />
Vaccination <strong>and</strong> prevention of disease<br />
<br />
Atopy<br />
Defects in Target Organs<br />
Bronchial epithelium<br />
Skin<br />
Gut<br />
Triggers<br />
Viral infections<br />
Exposure to allergens<br />
Tobacco smoke<br />
Indoor <strong>and</strong> outdoor pollutants<br />
Th2-mediated allergic inflammation<br />
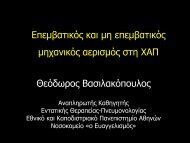
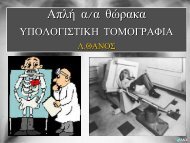
Figure 2. Factors Influencing the Development of Atopy <strong>and</strong> <strong>Allergic</strong> Inflammation Mediated by Th2 Cells (Atopic <strong>Allergic</strong> Disease).<br />
The induction of atopy is dependent on interactions between genes <strong>and</strong> the environment. The induction of atopic allergic disease<br />
may require further interactions between defects in the target organ <strong>and</strong> various environmental triggers. FceRI-b denotes the gene<br />
for the b chain of the high-affinity receptor for IgE.<br />
32 · N Engl J Med, Vol. 344, No. 1 · January 4, 2001 · www.nejm.org<br />
Downloaded from www.nejm.org by VASSILAKOPOULOS THEODOROS MD on April 1, 2009 .<br />
Copyright © 2001 Massachusetts Medical Society. All rights reserved.
ADVANCES IN IMMUNOLOGY<br />
er. Techniques used to identify genes that are relevant<br />
to allergy <strong>and</strong> asthma include the c<strong>and</strong>idate-gene approach,<br />
which depends on the identification of polymorphisms<br />
in a known gene, <strong>and</strong> positional cloning,<br />
which links the inheritance of a specific chromosomal<br />
region with the inheritance of a disease. 22 Such studies<br />
have linked several loci to atopy, but the clinical<br />
relevance of these findings is unclear. Examples are<br />
the associations between an allele of the HLA-DR<br />
locus <strong>and</strong> reactivity to the ragweed allergen Ra 5 29<br />
<strong>and</strong> the linkage of atopy to a polymorphism of the<br />
gene for the b chain of the high-affinity receptor for<br />
IgE (FceRI-b) 30 <strong>and</strong> to the interleukin-4 family of<br />
cytokine genes on chromosome 5. 31 By contrast, certain<br />
alleles of the tumor necrosis factor gene complex,<br />
although linked to asthma, are independent of<br />
serum IgE levels <strong>and</strong> other measures of atopy. 32<br />
Polymorphisms of the FceRI-b gene appear to be<br />
associated with equal frequency to severe atopy, asthma,<br />
<strong>and</strong> eczema. Also, positional cloning indicates<br />
that chromosomes 2q, 5q, 6q, 12q, <strong>and</strong> 13q contain<br />
loci linked to both asthma <strong>and</strong> atopy. 22 Polymorphisms<br />
in the gene encoding the high-affinity receptor<br />
for bacterial lipopolysaccharide (CD14) have been<br />
linked to total serum IgE levels <strong>and</strong> may help explain<br />
the association between childhood infections <strong>and</strong> the<br />
development of atopy. 33<br />
Several of the genes <strong>and</strong> genetic regions that have<br />
been linked to atopy <strong>and</strong> asthma have also been implicated<br />
in rheumatoid arthritis (chromosome 2) <strong>and</strong> inflammatory<br />
bowel disease (chromosomes 2 <strong>and</strong> 12). 22<br />
There has been recent interest in loci with pharmacologic<br />
relevance. Polymorphisms within the promoter<br />
region of the 5-lipoxygenase gene 34 <strong>and</strong> in the b-adrenergic<br />
receptor gene may regulate the response to inhibitors<br />
of 5-lipoxygenase or b-adrenergic agonists,<br />
respectively. 22,34 These findings raise the possibility that<br />
genotyping will become useful in planning therapy<br />
for asthma <strong>and</strong> other allergic diseases.<br />
IgE AND ITS RECEPTORS<br />
Acute allergic reactions result from the release of<br />
preformed granule-associated mediators, membranederived<br />
lipids, cytokines, <strong>and</strong> chemokines when an allergen<br />
interacts with IgE that is bound to mast cells<br />
or basophils by the a chain of the high-affinity IgE<br />
receptor (FceRI-a). 35 This receptor also occurs on<br />
antigen-presenting cells, where it can facilitate the<br />
IgE-dependent trapping <strong>and</strong> presentation of allergen<br />
to T cells. 36 Eosinophils also possess FceRI-a, but in<br />
these cells it is almost entirely intracellular; after being<br />
released by degranulation of the eosinophil, it may<br />
help regulate local levels of IgE. 37<br />
The most important inducers of the production of<br />
IgE are interleukin-4 <strong>and</strong> interleukin-13. These cytokines<br />
initiate transcription of the gene for the epsilon<br />
class of the constant region (C e<br />
) of the immunoglobulin<br />
heavy chain. The production of IgE also<br />
requires two transcription factors, nuclear factor kB<br />
<strong>and</strong> STAT-6; the former pathway involves the costimulatory<br />
molecules CD40 <strong>and</strong> the CD40 lig<strong>and</strong><br />
(CD154), <strong>and</strong> the latter is activated when interleukin-4<br />
binds to the high-affinity a chain of the interleukin-4<br />
receptor. 38<br />
Allergens, including the products of some infectious<br />
microorganisms (e.g., Aspergillus fumigatus) <strong>and</strong><br />
helminthic parasites, evoke Th2-mediated responses<br />
that are characterized by high serum levels of IgE,<br />
whereas other bacterial antigens (such as those associated<br />
with Listeria monocytogenes <strong>and</strong> Mycobacterium<br />
tuberculosis) elicit a Th1-mediated response that<br />
is dominated by cellular immunity (the appearance<br />
of cytotoxic T cells <strong>and</strong> delayed hypersensitivity). In<br />
this latter class of organisms, the DNA contains repeating<br />
sequences of cytosine <strong>and</strong> guanosine nucleosides<br />
called CpG repeats. These CpG repeats can<br />
bind to receptors on antigen-presenting cells <strong>and</strong> trigger<br />
the release of interleukin-12. This cytokine, which<br />
is produced almost exclusively by antigen-presenting<br />
cells, drives <strong>and</strong> maintains the Th1-mediated response.<br />
Furthermore, the interferon-g produced by activated<br />
Th1 cells 39 <strong>and</strong> interleukin-18, produced by macrophages,<br />
39 join forces to suppress the production of<br />
IgE antibodies. 40 Therefore, at least theoretically, interferon-g,<br />
interleukin-12, <strong>and</strong> interleukin-18, either<br />
alone or in combination, have therapeutic potential<br />
for inhibiting the synthesis of IgE. Furthermore (as<br />
discussed below), CpG repeats may redirect allergens<br />
to produce a Th1-mediated, rather than a Th2-mediated,<br />
immune response.<br />
The physiologic relevance of the low-affinity IgE<br />
receptor (CD23) remains speculative. It may be involved<br />
in antigen trapping <strong>and</strong> presentation, thereby<br />
augmenting the production of interleukin-4 or interleukin-13.<br />
41 It can, however, override the positive<br />
effects of antigen presentation by combining with excess<br />
IgE <strong>and</strong> antigen under conditions in which high<br />
levels of interleukin-4 have caused the up-regulation<br />
of this type of receptor. 42<br />
ALLERGIC INFLAMMATION<br />
In a person with atopy, exposure of the skin, nose,<br />
or airway to a single dose of allergen produces a cutaneous<br />
wheal-<strong>and</strong>-flare reaction, sneezing <strong>and</strong> runny<br />
nose, or wheezing within minutes. Depending on the<br />
amount of the allergen, these immediate hypersensitivity<br />
reactions are followed by a late-phase reaction,<br />
which reaches a peak six to nine hours after exposure<br />
to the allergen <strong>and</strong> then slowly resolves. In the skin,<br />
late-phase reactions are characterized by an edematous,<br />
red, <strong>and</strong> slightly indurated swelling; in the nose,<br />
by sustained blockage; <strong>and</strong> in the lung, by further<br />
wheezing.<br />
Immediate hypersensitivity is the basis of acute allergic<br />
reactions. It is caused by molecules released by<br />
mast cells when an allergen interacts with membrane-<br />
N Engl J Med, Vol. 344, No. 1 · January 4, 2001 · www.nejm.org · 33<br />
Downloaded from www.nejm.org by VASSILAKOPOULOS THEODOROS MD on April 1, 2009 .<br />
Copyright © 2001 Massachusetts Medical Society. All rights reserved.
The New Engl<strong>and</strong> Journal of Medicine<br />
TABLE 1. THE ROLE OF CYTOKINES PRODUCED BY Th2 CELLS IN CHRONIC ALLERGIC INFLAMMATION.<br />
EVENT Th2-TYPE CYTOKINES INVOLVED OTHER FACTORS INVOLVED<br />
Production of IgE<br />
Development <strong>and</strong> accumulation of<br />
eosinophils <strong>and</strong> basophils<br />
Development of mast cells<br />
Interleukin-4, interleukin-9, <strong>and</strong><br />
interleukin-13<br />
Interleukin-4, interleukin-5, interleukin-9,<br />
<strong>and</strong> interleukin-13<br />
Interleukin-4, interleukin-9, <strong>and</strong> interleukin-13<br />
Interferon-g, interleukin-12, <strong>and</strong> interleukin-18<br />
Interleukin-3, granulocyte–macrophage<br />
colony-stimulating factor,<br />
eotaxin-1, eotaxin-2, eotaxin-3,<br />
RANTES, monocyte chemotactic<br />
protein 3, monocyte chemotactic<br />
protein 4, <strong>and</strong> vascular-cell adhesion<br />
molecule 1<br />
Interleukin-3 <strong>and</strong> stem-cell factor<br />
Airway hyperresponsiveness Interleukin-9 <strong>and</strong> interleukin-13 Interleukin-11 <strong>and</strong> growth factors involved<br />
in remodeling<br />
Overproduction of mucus<br />
Interleukin-4, interleukin-9, <strong>and</strong> interleukin-13<br />
Histamine, leukotriene C 4<br />
, leukotriene<br />
D 4<br />
, substance P, <strong>and</strong> calcitonin-gene–related<br />
peptide<br />
bound IgE. The complex of allergen, IgE, <strong>and</strong> FceRI<br />
on the surface of the mast cell triggers a noncytotoxic,<br />
energy-dependent release of preformed, granuleassociated<br />
histamine <strong>and</strong> tryptase <strong>and</strong> the membranederived<br />
lipid mediators leukotrienes, prostagl<strong>and</strong>ins,<br />
<strong>and</strong> platelet-activating factor. These mast-cell mediators<br />
have a critical role in anaphylaxis, rhinoconjunctivitis,<br />
<strong>and</strong> urticaria. The role of histamine in chronic<br />
asthma <strong>and</strong> eczema is probably minimal, however, as<br />
shown by the relative ineffectiveness of histamine antagonists<br />
in controlling these conditions.<br />
Mast cells produce the three cysteinyl leukotrienes<br />
C 4<br />
, D 4<br />
, <strong>and</strong> E 4<br />
, which cause the contraction of smooth<br />
muscles, vasodilatation, increased vascular permeability,<br />
<strong>and</strong> the hypersecretion of mucus when they bind<br />
to specific receptors. 43<br />
Eosinophils, macrophages, <strong>and</strong> monocytes are also<br />
major sources of cysteinyl leukotrienes. Mast cells also<br />
contain tryptase, a four-chain neutral protease that<br />
activates the protease-activated receptors on endothelial<br />
<strong>and</strong> epithelial cells. The activation of these receptors<br />
initiates a cascade of events, including the up-regulation<br />
of adhesion molecules that selectively attract<br />
eosinophils <strong>and</strong> basophils. 27<br />
In the cutaneous late-phase reaction, eosinophils<br />
<strong>and</strong> neutrophils accumulate, <strong>and</strong> then CD4+ T cells<br />
<strong>and</strong> basophils infiltrate the site. 44 Late-phase asthmatic<br />
45 <strong>and</strong> nasal 10 reactions have a similar pattern of<br />
cellular infiltration, although basophils are not prominent<br />
in the lower airways. 46<br />
Depending on the target organ, late-phase reactions<br />
can be provoked by the activation of mast cells or<br />
T cells. In the skin of atopic subjects <strong>and</strong> normal subjects,<br />
cross-linking of mast-cell–bound IgE with an<br />
antibody against IgE provokes both immediate hypersensitivity<br />
<strong>and</strong> late-phase reactions. 47 Late-phase reactions<br />
can be induced in patients with atopic asthma in<br />
the absence of immediate hypersensitivity involving<br />
mast cells. These reactions were induced in patients<br />
with asthma who were allergic to cats by an intradermal<br />
injection of peptides derived from a cat allergen. 48<br />
The fact that these late-phase reactions were independent<br />
of IgE <strong>and</strong> were major-histocompatibility-complex<br />
(MHC)–restricted indicates that the activation<br />
of T cells alone is sufficient to initiate airway narrowing<br />
in patients with allergic asthma.<br />
Antigen-presenting cells are critical in initiating<br />
<strong>and</strong> controlling allergic inflammation. Dendritic cells<br />
<strong>and</strong> cutaneous Langerhans’ cells are particularly important<br />
in asthma <strong>and</strong> atopic eczema, respectively.<br />
They present antigen to CD4+ Th2 cells in an MHC<br />
class II–restricted fashion. Overproduction of the<br />
granulocyte–macrophage colony-stimulating factor in<br />
the airway mucosa of patients with asthma enhances<br />
antigen presentation <strong>and</strong> increases the local accumulation<br />
of macrophages. 12 Alveolar macrophages obtained<br />
from patients with asthma by bronchoalveolar<br />
lavage present allergen to CD4+ T cells <strong>and</strong> stimulate<br />
the production of Th2-type cytokines, 49 whereas alveolar<br />
macrophages from control subjects do not.<br />
Th2-type cytokines such as interleukin-4, 5, 9,<br />
<strong>and</strong> 13 influence a wide range of events associated<br />
with chronic allergic inflammation. Interleukin-4 <strong>and</strong><br />
interleukin-13 stimulate the production of IgE <strong>and</strong><br />
vascular-cell adhesion molecule 1; interleukin-5 <strong>and</strong> interleukin-9<br />
are involved in the development of eosinophils;<br />
interleukin-4 <strong>and</strong> interleukin-9 promote<br />
the development of mast cells; interleukin-9 <strong>and</strong> interleukin-13<br />
help promote airway hyperresponsiveness 50 ;<br />
<strong>and</strong> interleukin-4, interleukin-9, <strong>and</strong> interleukin-13<br />
34 · N Engl J Med, Vol. 344, No. 1 · January 4, 2001 · www.nejm.org<br />
Downloaded from www.nejm.org by VASSILAKOPOULOS THEODOROS MD on April 1, 2009 .<br />
Copyright © 2001 Massachusetts Medical Society. All rights reserved.
ADVANCES IN IMMUNOLOGY<br />
Membrane-bound IgE<br />
Histamine, leukotrienes,<br />
platelet-activating factor<br />
Mast cell<br />
Interleukin-4<br />
Interleukin-5<br />
Acute <strong>Allergic</strong><br />
Reaction<br />
Wheezing<br />
Urticaria<br />
Sneezing, rhinorrhea,<br />
conjunctivitis<br />
B cell<br />
Allergen<br />
IgE production<br />
Eosinophil<br />
Basic proteins,<br />
leukotrienes,<br />
platelet-activating <br />
factor<br />
Interleukin-4<br />
Dendritic<br />
<br />
cell<br />
Th2<br />
Interleukin-5<br />
Chronic <strong>Allergic</strong><br />
Reaction<br />
MHC class II<br />
molecule<br />
T-cell receptor<br />
Histamine-releasing<br />
factor, neuropeptides<br />
Neurotrophins<br />
Mast cell<br />
Histamine,<br />
lipids, <br />
cytokines<br />
Further wheezing<br />
Sustained blockage<br />
of the nose<br />
Eczema<br />
<br />
Neuropeptides<br />
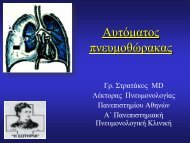
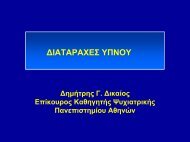
Figure 3. Pathways Leading to Acute <strong>and</strong> Chronic <strong>Allergic</strong> Reactions.<br />
Acute allergic reactions are due to the antigen-induced release of histamine <strong>and</strong> lipid mediators from mast cells. In the skin <strong>and</strong><br />
upper airways, basophils (not shown) may also participate in allergic tissue reactions. Chronic allergic reactions, including the latephase<br />
reaction, may depend on a combination of pathways, including the recruitment of eosinophils, the liberation of mast-cell<br />
products by histamine-releasing factors, 62 <strong>and</strong> neurogenic inflammation involving neurotrophins <strong>and</strong> neuropeptides. MHC denotes<br />
major histocompatibility complex.<br />
promote the overproduction of mucus (Table 1). Eosinophils<br />
can injure mucosal surfaces by releasing toxic<br />
basic proteins, cysteinyl leukotrienes, <strong>and</strong> plateletactivating<br />
factor. They also damage inhibitory M2<br />
muscarinic receptors, which may allow unchecked cholinergic<br />
responses in patients with asthma. 51 By contrast,<br />
eosinophils may also repair damage, since they<br />
produce fibrogenic growth factors <strong>and</strong> matrix metalloproteinase,<br />
which remodel airway tissue in asthma. 52<br />
Interleukin-5 releases both mature <strong>and</strong> immature<br />
eosinophils from the bone marrow, 53 regulates the expression<br />
of the transmembrane isoform of its own receptor,<br />
54 <strong>and</strong> is essential for the terminal differentiation<br />
of committed eosinophil precursors. 55 The preferential<br />
accumulation of eosinophils occurs through the interactions<br />
between selective adhesion molecules (a 4<br />
b 1<br />
integrin <strong>and</strong> vascular-cell adhesion molecule), the migration<br />
of eosinophils toward receptors for CC chemokines<br />
as a result of recruitment by eotaxin-1, eotaxin-2,<br />
eotaxin-3, RANTES, monocyte chemotactic<br />
protein (MCP) 3 <strong>and</strong> MCP-4; prolonged survival (delayed<br />
apoptosis) under the influence of interleukin-5,<br />
interleukin-3, <strong>and</strong> granulocyte–macrophage colonystimulating<br />
factor; <strong>and</strong> the local differentiation of tis-<br />
N Engl J Med, Vol. 344, No. 1 · January 4, 2001 · www.nejm.org · 35<br />
Downloaded from www.nejm.org by VASSILAKOPOULOS THEODOROS MD on April 1, 2009 .<br />
Copyright © 2001 Massachusetts Medical Society. All rights reserved.
The New Engl<strong>and</strong> Journal of Medicine<br />
sue-infiltrating eosinophil precursors induced by interleukin-5.<br />
56<br />
<strong>Allergic</strong> inflammation may also follow the release<br />
of neuropeptides from nerve cells by the action of<br />
nerve growth factor, brain-derived neurotrophic factor,<br />
<strong>and</strong> neurotrophin-3. 57,58 These neurotrophins are secreted<br />
by macrophages, T cells, eosinophils, <strong>and</strong> mast<br />
cells. 58 Neuropeptides, particularly substance P, calcitonin-gene–related<br />
peptide, <strong>and</strong> neurokinin A (all<br />
of which are located predominantly in sensory neurons,<br />
but also in inflammatory cells), cause characteristic<br />
features of allergic inflammation, including vasodilatation,<br />
increased vascular permeability, <strong>and</strong> in the<br />
lung, contraction of the smooth muscles of the airway<br />
<strong>and</strong> hypersecretion of mucus. 59 They also release<br />
histamine from mast cells in the lungs. 60 Tryptase can<br />
also trigger nerve cells to release neuropeptides by<br />
binding to protease-activated receptors. Further amplifications<br />
of chronic allergic reactions may be mediated<br />
by histamine-releasing factor or factors. 61 Pathways<br />
leading to acute <strong>and</strong> chronic allergic reactions<br />
are shown in Figure 3.<br />
REFERENCES<br />
1. Aberg N, Hesselmar B, Aberg B, Eriksson B. Increase of asthma, allergic<br />
rhinitis <strong>and</strong> eczema in Swedish schoolchildren between 1979 <strong>and</strong> 1991.<br />
Clin Exp <strong>Allergy</strong> 1995;25:815-9.<br />
2. Smith DH, Malone DC, Lawson KA, Okamoto LJ, Battista C, Saunders<br />
WB. A national estimate of the economic costs of asthma. Am J Respir<br />
Crit Care Med 1997;156:787-93.<br />
3. von Pirquet C. <strong>Allergy</strong>. In: Gell PGH, Coombs RRA, eds. Clinical aspects<br />
of immunology. Oxford, Engl<strong>and</strong>: Blackwell Scientific, 1963.<br />
4. Kemeny DM, Urbanek R, Ewan P, et al. The subclass of IgG antibody<br />
in allergic disease. II. The IgG subclass of antibodies produced following<br />
natural exposure to dust mite <strong>and</strong> grass pollen in atopic <strong>and</strong> non-atopic individuals.<br />
Clin Exp <strong>Allergy</strong> 1989;19:545-9.<br />
5. Romagnani S. Human TH1 <strong>and</strong> TH2 subsets: doubt no more. Immunol<br />
Today 1991;12:256-7.<br />
6. Ebner C, Schenk S, Najafian N, et al. Nonallergic individuals recognize<br />
the same T cell epitopes of Bet v 1, the major birch pollen allergen, as atopic<br />
patients. J Immunol 1995;154:1932-40.<br />
7. Till S, Durham S, Dickason R, et al. IL-13 production by allergen-stimulated<br />
T cells is increased in allergic disease <strong>and</strong> associated with IL-5 but<br />
not IFN-gamma expression. Immunology 1997;91:53-7.<br />
8. Kay AB, Ying S, Varney V, et al. Messenger RNA expression of the cytokine<br />
gene cluster interleukin 3 (IL-3), IL-4, IL-5 <strong>and</strong> granulocyte/macrophage<br />
colony-stimulating factor, in allergen-induced late-phase cutaneous<br />
reactions in atopic subjects. J Exp Med 1991;173:775-8.<br />
9. Robinson DS, Hamid Q, Ying S, et al. Predominant T H2<br />
-type bronchoalveolar<br />
T-lymphocyte population in atopic asthma. N Engl J Med 1992;<br />
326:298-304.<br />
10. Durham SR, Ying S, Varney VA, et al. Cytokine messenger RNA expression<br />
for IL-3, IL-4, IL-5 <strong>and</strong> granulocyte/macrophage-colony-stimulating<br />
factor in the nasal mucosa after local allergen provocation: relationship<br />
to tissue eosinophilia. J Immunol 1992;148:2390-4.<br />
11. Prescott S, Macaubas C, Holt BJ, et al. Transplacental priming of the<br />
human immune system to environmental allergens: universal skewing of<br />
initial T cell responses toward the Th2 cytokine profile. J Immunol 1998;<br />
160:4730-7.<br />
12. Holt PG, Macaubas C, Stumbles PA, Sly PD. The role of allergy in the<br />
development of asthma. Nature 1999;402:Suppl:B12-B17.<br />
13. Constant SL, Bottomly K. Induction of Th1 <strong>and</strong> Th2 CD4+ T cell responses:<br />
the alternative approaches. Annu Rev Immunol 1997;15:297-322.<br />
14. Rogers PR, Croft M. Peptide dose, affinity, <strong>and</strong> time of differentiation<br />
can contribute to the Th1/Th2 cytokine balance. J Immunol 1999;163:<br />
1205-13.<br />
15. Caramori G, Lim S, Ciaccia A, Fabbri LM, Barnes PJ, Adcock IM.<br />
GATA transcription factors expression in T cells, monocytes <strong>and</strong> bronchial<br />
biopsies of normal <strong>and</strong> asthmatic subjects. Am J Respir Crit Care Med<br />
1999;157:Suppl:A908. abstract.<br />
16. von Mutius E, Martinez FD, Fritzsch C, Nicolai T, Roell G, Thiemann<br />
HH. Prevalence of asthma <strong>and</strong> atopy in two areas of East <strong>and</strong> West Germany.<br />
Am J Respir Crit Care Med 1994;149:358-64.<br />
17. von Mutius E, Weil<strong>and</strong> SK, Fritzsch C, Duhme H, Keil U. Increasing<br />
prevalence of hay fever <strong>and</strong> atopy among children in Leipzig, East Germany.<br />
Lancet 1998;351:862-6.<br />
18. Rook GA, Stanford JL. Give us this day our daily germs. Immunol Today<br />
1998;19:113-6.<br />
19. Sepp E, Julge K, Vasar M, Naaber P, Bjorksten B, Mikelsaar M. Intestinal<br />
microflora of Estonian <strong>and</strong> Swedish infants. Acta Paediatr 1997;86:<br />
956-61.<br />
20. Bjorksten B, Naaber P, Sepp E, Mikelsaar M. The intestinal microflora<br />
in allergic Estonian <strong>and</strong> Swedish 2-year-old children. Clin Exp <strong>Allergy</strong><br />
1999;29:342-6. [Erratum, Clin Exp <strong>Allergy</strong> 2000;30:1047.]<br />
21. Braun-Fahrländer C, Gassner M, Grize L, et al. Prevalence of hay fever<br />
<strong>and</strong> allergic sensitization in farmer’s children <strong>and</strong> their peers living in the<br />
same rural community. Clin Exp <strong>Allergy</strong> 1999;29:28-34.<br />
22. Cookson W. The alliance of genes <strong>and</strong> environment in asthma <strong>and</strong> allergy.<br />
Nature 1999;402:Suppl:B5-B11.<br />
23. Openshaw PJM, Hewitt C. Protective <strong>and</strong> harmful effects of viral infections<br />
in childhood on wheezing disorders <strong>and</strong> asthma. Am J Respir Crit<br />
Care Med 2000;162:Suppl:S40-S43.<br />
24. Ball TM, Castro-Rodriguez JA, Griffith KA, Holberg CJ, Martinez<br />
FD, Wright AL. Siblings, day-care attendance, <strong>and</strong> the risk of asthma <strong>and</strong><br />
wheezing during childhood. N Engl J Med 2000;343:538-43.<br />
25. Schwartz J, Gold D, Dockery DW, Weiss ST, Speizer FE. Predictors of<br />
asthma <strong>and</strong> persistent wheeze in a national sample of children in the United<br />
States: association with social class, perinatal events, <strong>and</strong> race. Am Rev<br />
Respir Dis 1990;142:555-62.<br />
26. Call RS, Smith TF, Morris E, Chapman MD, Platts-Mills TA. Risk factors<br />
for asthma in inner city children. J Pediatr 1992;121:862-6.<br />
27. Holgate ST. The epidemic of allergy <strong>and</strong> asthma. Nature 1999;402:<br />
Suppl:B2-B4.<br />
28. Burks W, Sampson HA, Bannon GA. Peanut allergens. <strong>Allergy</strong> 1998;<br />
53:725-30.<br />
29. Marsh DG, Hsu SH, Roebber M, et al. HLA-Dw2: a genetic marker<br />
for human immune response to short ragweed pollen allergen Ra 5. I. Response<br />
resulting primarily from natural antigenic exposure. J Exp Med<br />
1982;155:1439-51.<br />
30. Hill MR, Cookson WOCM. A new variant of the b subunit of the<br />
high-affinity receptor for immunoglobulin E (FceRI-b E237G): associations<br />
with measures of atopy <strong>and</strong> bronchial hyper-responsiveness. Hum<br />
Mol Genet 1996;5:959-62.<br />
31. Marsh DG, Neely JD, Breazeale DR, et al. Linkage analysis of IL4 <strong>and</strong><br />
other chromosome 5q31.1 markers <strong>and</strong> total serum immunoglobulin E<br />
concentrations. Science 1994;264:1152-6.<br />
32. Moffatt MF, Cookson WOCM. Tumour necrosis factor haplotypes <strong>and</strong><br />
asthma. Hum Mol Genet 1997;6:551-4.<br />
33. Baldini M, Lohman IC, Halonen M, Erickson RP, Holt PG, Martinez<br />
FD. A polymorphism in the 5'-flanking region of the CD14 gene is associated<br />
with circulating soluble CD14 levels <strong>and</strong> with total serum immunoglobulin<br />
E. Am J Respir Cell Mol Biol 1999;20:976-83.<br />
34. Drazen JM, Y<strong>and</strong>ava CN, Dube L, et al. Pharmacogenetic association<br />
between ALOX5 promoter genotype <strong>and</strong> the response to anti-asthma<br />
treatment. Nat Genet 1999;22:168-70.<br />
35. Kinet JP. The high-affinity IgE receptor (Fc epsilon RI): from physiology<br />
to pathology. Annu Rev Immunol 1999;17:931-72.<br />
36. Stingl G, Maurer D. IgE-mediated allergen presentation via FceRI on<br />
antigen-presenting cells. Int Arch <strong>Allergy</strong> Immunol 1997;113:24-9.<br />
37. Smith SJ, Ying S, Meng Q, et al. Blood eosinophils from atopic donors<br />
express messenger RNA for the a, b <strong>and</strong> g subunits of the high-affinity<br />
IgE receptor (FceRI) <strong>and</strong> intracellular, but not cell surface, a subunit protein.<br />
J <strong>Allergy</strong> Clin Immunol 2000;105:309-17.<br />
38. Corry DB, Kheradm<strong>and</strong> F. Induction <strong>and</strong> regulation of the IgE response.<br />
Nature 1999;402:Suppl:B18-B23.<br />
39. Robinson D, Shibuya K, Mui A, et al. IGIF does not drive Th1 development<br />
but synergizes with IL-12 for interferon-g production <strong>and</strong> activates<br />
IRAK <strong>and</strong> NFkB. Immunity 1997;7:571-81.<br />
40. Yoshimoto T, Nagai N, Ohkusu K, Ueda H, Okamura H, Nakanishi<br />
K. LPS-stimulated SJL macrophages produce IL-12 <strong>and</strong> IL-18 that inhibit<br />
IgE production in vitro by induction of IFN-gamma production from<br />
CD3intIL-2Rb+ T cells. J Immunol 1998;161:1483-92.<br />
41. Squire CM, Studer EJ, Lees A, Finkelman FD, Conrad DH. Antigen<br />
presentation is enhanced by targeting antigen to the FceRII by antigenanti-FceRII<br />
conjugates. J Immunol 1994;152:4388-96.<br />
42. Gustavsson S, Hjulstrom S, Liu T, Heyman B. CD23/IgE-mediated<br />
regulation of the specific antibody response in vivo. J Immunol 1994;152:<br />
4793-800.<br />
43. Drazen JM, Israel E, O’Byrne PM. Treatment of asthma with drugs<br />
modifying the leukotriene pathway. N Engl J Med 1999;340:197-206.<br />
[Errata, N Engl J Med 1999;340:663, 341:1632.]<br />
36 · N Engl J Med, Vol. 344, No. 1 · January 4, 2001 · www.nejm.org<br />
Downloaded from www.nejm.org by VASSILAKOPOULOS THEODOROS MD on April 1, 2009 .<br />
Copyright © 2001 Massachusetts Medical Society. All rights reserved.
ADVANCES IN IMMUNOLOGY<br />
44. Ying S, Robinson DS, Meng Q, et al. C-C chemokines in allergeninduced<br />
late-phase cutaneous responses in atopic subjects: association of<br />
eotaxin with early 6-hour eosinophils, <strong>and</strong> of eotaxin-2 <strong>and</strong> monocyte chemoattractant<br />
protein-4 with the later 24-hour tissue eosinophilia, <strong>and</strong> relationship<br />
to basophils <strong>and</strong> other C-C chemokines (monocyte chemoattractant<br />
protein-3 <strong>and</strong> RANTES). J Immunol 1999;163:3976-84.<br />
45. Robinson DS, Hamid Q, Bentley A, Ying S, Kay AB, Durham SR. Activation<br />
of CD4+ T cells, increased TH2-type cytokine mRNA expression,<br />
<strong>and</strong> eosinophil recruitment in bronchoalveolar lavage after allergen inhalation<br />
challenge in patients with atopic asthma. J <strong>Allergy</strong> Clin Immunol<br />
1993;92:313-24.<br />
46. Macfarlane AJ, Kon OM, Smith SJ, et al. Basophils, eosinophils, <strong>and</strong><br />
mast cells in atopic <strong>and</strong> nonatopic asthma <strong>and</strong> in late-phase allergic reactions<br />
in the lung <strong>and</strong> skin. J <strong>Allergy</strong> Clin Immunol 2000;105:99-107.<br />
47. Dolovich J, Hargreave FE, Chalmers R, Shier KJ, Gauldie J, Bienenstock<br />
J. Late cutaneous allergic responses in isolated IgE-dependent reactions.<br />
J <strong>Allergy</strong> Clin Immunol 1973;52:38-46.<br />
48. Haselden BM, Kay AB, Larché M. Immunoglobulin E-independent<br />
major histocompatibility complex-restricted T cell peptide epitope-induced<br />
late asthmatic reactions. J Exp Med 1999;189:1885-94.<br />
49. Larché M, Till SJ, Haselden BM, et al. Costimulation through CD86<br />
is involved in airway antigen-presenting cell <strong>and</strong> T cell responses to allergen<br />
in atopic asthmatics. J Immunol 1998;161:6375-82.<br />
50. Wills-Karp M, Luyimbazi J, Xu X, et al. Interleukin-13: central mediator<br />
of allergic asthma. Science 1998;282:2258-61.<br />
51. Adamko DJ, Yost BL, Gleich GJ, Fryer AD, Jacoby DB. Ovalbumin<br />
sensitization changes the inflammatory response to subsequent parainfluenza<br />
infection: eosinophils mediate airway hyperresponsiveness, m(2) muscarinic<br />
receptor dysfunction, <strong>and</strong> antiviral effects. J Exp Med 1999;190:<br />
1465-78.<br />
52. Levi-Schaffer F, Garbuzenko E, Rubin A, et al. Human eosinophils<br />
regulate human lung- <strong>and</strong> skin-derived fibroblast properties in vitro: a role<br />
for transforming growth factor beta (TGF-b). Proc Natl Acad Sci U S A<br />
1999;96:9660-5.<br />
53. Palframan RT, Collins PD, Severs NJ, Rothery S, Williams TJ, Rankin<br />
SM. Mechanisms of acute eosinophil mobilization from the bone marrow<br />
stimulated by interleukin 5: the role of specific adhesion molecules <strong>and</strong><br />
phosphatidylinositol 3-kinase. J Exp Med 1998;188:1621-32.<br />
54. Tavernier J, Van der Heyden J, Verhee A, et al. Interleukin 5 regulates<br />
the isoform expression of its own receptor a-subunit. Blood 2000;95:<br />
1600-7.<br />
55. Clutterbuck EJ, Hirst EM, S<strong>and</strong>erson CJ. Human interleukin-5<br />
(IL-5) regulates the production of eosinophils in human bone marrow<br />
cultures: comparison <strong>and</strong> interaction with IL-1, IL-3, IL-6, <strong>and</strong> GMCSF.<br />
Blood 1989;73:1504-12.<br />
56. Denburg JA. Hemopoietic progenitors <strong>and</strong> cytokines in allergic inflammation.<br />
<strong>Allergy</strong> 1998;53:Suppl:22-6.<br />
57. Bonini S, Lambiase A, Bonini S, Levi-Schaffer F, Aloe L. Nerve<br />
growth factor: an important molecule in allergic inflammation <strong>and</strong> tissue<br />
remodeling. Int Arch <strong>Allergy</strong> Immunol 1999;118:159-62.<br />
58. Braun A, Lommatzsch M, Renz H. The role of neurotrophins in allergic<br />
bronchial asthma. Clin Exp <strong>Allergy</strong> 2000;30:178-86.<br />
59. Belvisi MG, Fox AJ. Neuropeptides. In: Kay AB, ed. <strong>Allergy</strong> <strong>and</strong> allergic<br />
diseases. Vol. 1. Oxford, Engl<strong>and</strong>: Blackwell Scientific, 1997:447-80.<br />
60. Forsythe P, McGarvey LPA, Heaney LG, MacMahon J, Ennis M. Sensory<br />
neuropeptides induce histamine release from bronchoalveolar lavage<br />
cells in both nonasthmatic coughers <strong>and</strong> cough variant asthmatics. Clin<br />
Exp <strong>Allergy</strong> 2000;30:225-32.<br />
61. Steinhoff M, Vergnolle N, Young SH, et al. Agonists of proteinaseactivated<br />
receptor 2 induce inflammation by a neurogenic mechanism. Nat<br />
Med 2000;6:151-8.<br />
62. MacDonald SM, Rafnar T, Langdon J, Lichtenstein LM. Molecular<br />
identification of an IgE-dependent histamine-releasing factor. Science<br />
1995;269:688-90.<br />
Copyright © 2001 Massachusetts Medical Society.<br />
N Engl J Med, Vol. 344, No. 1 · January 4, 2001 · www.nejm.org · 37<br />
Downloaded from www.nejm.org by VASSILAKOPOULOS THEODOROS MD on April 1, 2009 .<br />
Copyright © 2001 Massachusetts Medical Society. All rights reserved.