APPLICATION FOR CERTIFICATE OF DISABILITY.pdf
APPLICATION FOR CERTIFICATE OF DISABILITY.pdf
APPLICATION FOR CERTIFICATE OF DISABILITY.pdf

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Application No.....................<br />
Token No..............................<br />
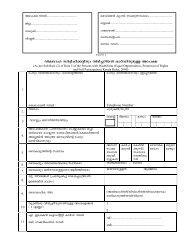
<strong>FOR</strong>M 1/t^mdw 1<br />
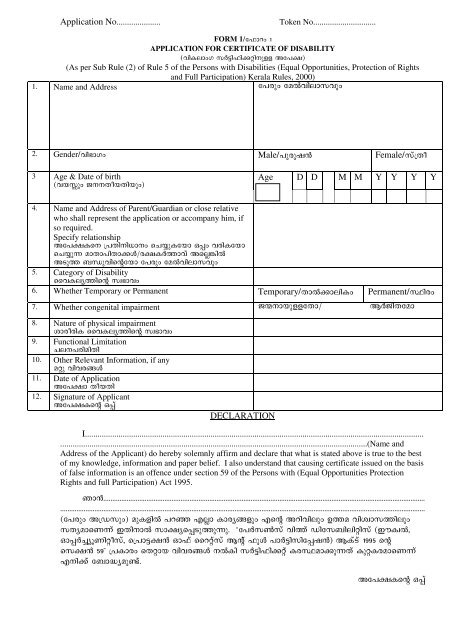
<strong>APPLICATION</strong> <strong>FOR</strong> <strong>CERTIFICATE</strong> <strong>OF</strong> <strong>DISABILITY</strong><br />
(hnIemwK kÀ«n^n¡än\pff At]£)<br />
(As per Sub Rule (2) of Rule 5 of the Persons with Disabilities (Equal Opportunities, Protection of Rights<br />
and Full Participation) Kerala Rules, 2000)<br />
1. Name and Address t]cpw taðhnemkhpw<br />
2. Gender/hn`mKw Male/]pcpj³ Female/kv{Xo<br />
3 Age & Date of birth<br />
(hbÊpw P\\XobXnbpw)<br />
Age D D M M Y Y Y Y<br />
4. Name and Address of Parent/Guardian or close relative<br />
who shall represent the application or accompany him, if<br />
so required.<br />
Specify relationship<br />
At]£Is\ {]Xn\n[m\w sN¿pItbm H¸w hcnItbm<br />
sN¿p amXm]nXm¡Ä/c£IÀ¯mhv Asñ¦nð<br />
ASp¯ _Ôphnsâtbm t]cpw taðhnemkhpw<br />
5. Category of Disability<br />
sshIey¯nsâ kz`mhw<br />
6. Whether Temporary or Permanent Temporary/Xmð¡menIw Permanent/Øncw<br />
7. Whether congenital impairment Pò\mbpfftXm/ BÀPnXtam<br />
8. Nature of physical impairment<br />
imcocnI sshIey¯nsâ kz`mhw<br />
9. Functional Limitation<br />
Ne\]cnanXn<br />
10. Other Relevant Information, if any<br />
aäp hnhc§Ä<br />
11. Date of Application<br />
At]£m XobXn<br />
12. Signature of Applicant<br />
At]£Isâ H¸v<br />
DECLARATION<br />
I..................................................................................................................................................................<br />
...................................................................................................................................................(Name and<br />
Address of the Applicant) do hereby solemnly affirm and declare that what is stated above is true to the best<br />
of my knowledge, information and paper belief. I also understand that causing certificate issued on the basis<br />
of false information is an offence under section 59 of the Persons with (Equal Opportunities Protection<br />
Rights and full Participation) Act 1995.<br />
Rm³...................................................................................................................................................................................<br />
...........................................................................................................................................................................................................<br />
(t]cpw A{Ukpw) apIfnð ]dª Fñm Imcy§fpw Fsâ Adnhnepw D¯a hnizmk¯nepw<br />
kXyamsWv CXn\mð km£ys¸Sp¯pp. “t]Àk¬kv hn¯v Untk_nenänkv (CuIzð,<br />
Hm¸À¨yqWnäokv, s{]m«£³ Hm^v ssdävkv Bâv ^pÄ ]mÀ«nknt¸j³) BIvSv 1995 sâ<br />
sk£³ 59” {]Imcw sXämb hnhc§Ä \ðIn kÀ«n^n¡äv IcØam¡pXv IpäIcamsWv<br />
F\n¡v t_m²yapïv.<br />
At]£Isâ H¸v
ADDITIONAL IN<strong>FOR</strong>MATION<br />
Application No......................................... Place of Medical camp.......................................<br />
District..................................................... Block...................................................................<br />
Thaluk..................................................... Panchayat...........................................................<br />
Village...................................................... Ward (Name).....................................................<br />
Ward (No)..........................................................<br />
Marital Status<br />
(Single/Married/Divorced/Window<br />
Personal Identification Marks<br />
(hyànsb Xncn¨dnbpXn\pff ASbmf§Ä<br />
(2 F®w)<br />
Ration Card No<br />
1.<br />
2.<br />
Voters ID card No<br />
Blood Group<br />
A B AB O<br />
RH factor<br />
+ ve - ve<br />
Educational Qualification<br />
Occupation<br />
Monthly income as per ration card<br />
Employment Registration Yes No<br />
Employment Registration No. and<br />
Name:<br />
Spl. Employment Registration No &<br />
Name:<br />
Vocational rehabilitation Centre<br />
Name: