Patient Case History â Cognition & Aphasia
Patient Case History â Cognition & Aphasia
Patient Case History â Cognition & Aphasia

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
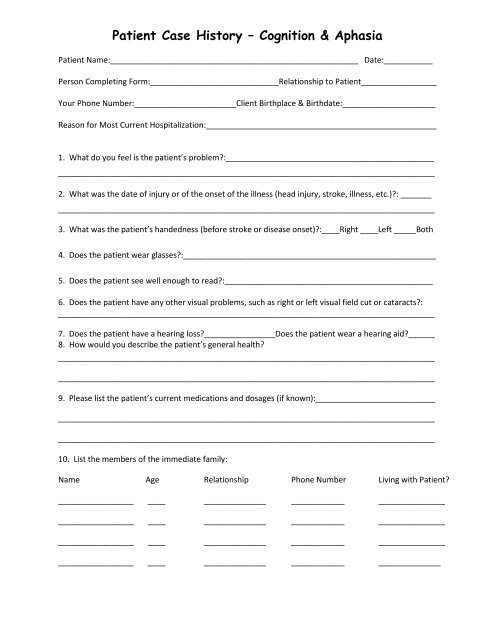
<strong>Patient</strong> <strong>Case</strong> <strong>History</strong> – <strong>Cognition</strong> & <strong>Aphasia</strong><br />
<strong>Patient</strong> Name:________________________________________________________ Date:___________<br />
Person Completing Form:_____________________________Relationship to <strong>Patient</strong>_________________<br />
Your Phone Number:_______________________Client Birthplace & Birthdate:_____________________<br />
Reason for Most Current Hospitalization:____________________________________________________<br />
1. What do you feel is the patient’s problem?:_______________________________________________<br />
_____________________________________________________________________________________<br />
2. What was the date of injury or of the onset of the illness (head injury, stroke, illness, etc.)?: _______<br />
_____________________________________________________________________________________<br />
3. What was the patient’s handedness (before stroke or disease onset)?:____Right ____Left _____Both<br />
4. Does the patient wear glasses?:_________________________________________________________<br />
5. Does the patient see well enough to read?:_______________________________________________<br />
6. Does the patient have any other visual problems, such as right or left visual field cut or cataracts?:<br />
_____________________________________________________________________________________<br />
7. Does the patient have a hearing loss?________________Does the patient wear a hearing aid?______<br />
8. How would you describe the patient’s general health?<br />
_____________________________________________________________________________________<br />
_____________________________________________________________________________________<br />
9. Please list the patient’s current medications and dosages (if known):___________________________<br />
_____________________________________________________________________________________<br />
_____________________________________________________________________________________<br />
10. List the members of the immediate family:<br />
Name Age Relationship Phone Number Living with <strong>Patient</strong>?<br />
_________________ ____ ______________ ____________ _______________<br />
_________________ ____ ______________ ____________ _______________<br />
_________________ ____ ______________ ____________ _______________<br />
_________________ ____ ______________ ____________ ______________
11. Does the patient have a history of the following?<br />
Onset Date and Current Status<br />
Stroke Yes No<br />
<strong>Aphasia</strong> Yes No<br />
Other Communication Disorder Yes No<br />
Right-or-Left-Sided Weakness Yes No<br />
Dementia Yes No<br />
Memory Impairment Yes No<br />
Other Neurological Disease Yes No<br />
Head Injury Yes No<br />
Seizure Disorder Yes No<br />
Clinical Depression Yes No<br />
Psychiatric Problems Yes No<br />
Alcohol Abuse/ Problems Yes No<br />
Other Substance Abuse Yes No<br />
Other Major Illness Yes No<br />
12. If the patient is not living at home, where does he/she live?:_________________________________<br />
13. What is the patient’s native language?: __________________________________________________<br />
If not English, at what age did the patient learn English?:_______________________________________<br />
14. What is the patients highest level of education?:__________________________________________<br />
15. What (is/was) the patient’s primary occupation?:_________________________________________<br />
16. <strong>Patient</strong>’s mother’s name:_______________________Living____________Deceased____________<br />
<strong>Patient</strong>’s father’s name:_________________________Living____________Deceased____________<br />
17. Marital Status: Single___Divorced___Widowed___Separated___Married___Remarried___
18. Does the patient have children or grandchildren? If so, please complete the information below:<br />
Children Age Address (city & state)<br />
________________ __________________ _____ _____________________________________<br />
________________ __________________ _____ _____________________________________<br />
________________ __________________ _____ _____________________________________<br />
________________ __________________ _____ _____________________________________<br />
________________ __________________ _____ _____________________________________<br />
Grandchildren Age Address (city & state)<br />
________________ __________________ _____ _____________________________________<br />
________________ __________________ _____ _____________________________________<br />
________________ __________________ _____ _____________________________________<br />
________________ __________________ _____ _____________________________________<br />
________________ __________________ _____ _____________________________________<br />
19. Does the patient need to be taken care of at all times?:_______ _____________________________<br />
_____________________________________________________________________________________<br />
20. To what extent can the patient care for him/herself (dress, feed, and wash himself)?:_____________<br />
______________________________________________________________________________________<br />
21. Describe the patient’s ability to communicate:_____________________________________________<br />
______________________________________________________________________________________<br />
22. How much does he or she talk or write now (hourly, daily, frequently, occasionally, etc.)?:__________<br />
______________________________________________________________________________________<br />
23. To what degree do other adults understand the patient’s communication?:_____________________<br />
______________________________________________________________________________________<br />
24. What strategies, if any, have you found useful to help with the patient’s communication?:_________<br />
_____________________________________________________________________________________<br />
25. Describe patient’s skills and living situation prior to this illness (e.g. was he/she functioning independently,<br />
living alone, communicating with others, etc.). How has he/she changed?:<br />
______________________________________________________________________________________<br />
______________________________________________________________________________________<br />
______________________________________________________________________________________
26.<br />
Is he or she attempting to communicate verbally? Yes No<br />
Is he or she attempting to communicate in writing? Yes No<br />
Is he or she attempting to communicate using gestures? Yes No<br />
Is his or her speech intelligible? Yes No<br />
Is his or her writing intelligible? Yes No<br />
Is there automatic speech (e.g., “Hello”, “Thank You”, “I’m fine”) Yes No<br />
Have you read or heard anything about aphasia or dementia? Yes No<br />
27. Below are words that describe a person’s personality and behavior. Circle those words that you feel<br />
apply to the patient’s previous status (before illness/accident).<br />
Happy Fights often Sad Enthusiastic <strong>Patient</strong><br />
Very friendly Warm Independent Energetic Intense<br />
Moody Critical Dependent Prefers to be alone Jealous<br />
Authoritarian Supportive Impatient Shy Receptive<br />
Bossy At ease Responsive Cooperative Relaxed<br />
Active Indifferent Distractible Outgoing Directive<br />
Tense Listless Cold Can’t sleep Affectionate<br />
Even tempered Quarrelsome Vigorous Easily fatigued Curious<br />
28. Does the patient watch TV? If so, what are his or her favorite programs?:______________________<br />
_____________________________________________________________________________________<br />
29. Does the patient read much? If so, what type of reading material does he or she enjoy?:__________<br />
_____________________________________________________________________________________<br />
Thank you so much for taking the time to complete this referral packet