Late Withdrawal Form - St. Cloud State University
Late Withdrawal Form - St. Cloud State University
Late Withdrawal Form - St. Cloud State University

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
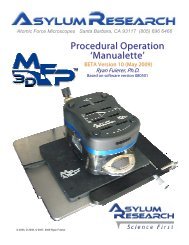
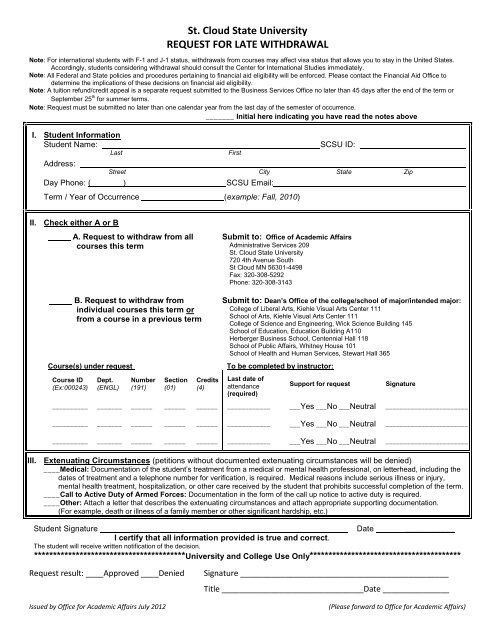
<strong>St</strong>. <strong>Cloud</strong> <strong>St</strong>ate <strong>University</strong><br />
REQUEST FOR LATE WITHDRAWAL<br />
Note: For international students with F-1 and J-1 status, withdrawals from courses may affect visa status that allows you to stay in the United <strong>St</strong>ates.<br />
Accordingly, students considering withdrawal should consult the Center for International <strong>St</strong>udies immediately.<br />
Note: All Federal and <strong>St</strong>ate policies and procedures pertaining to financial aid eligibility will be enforced. Please contact the Financial Aid Office to<br />
determine the implications of these decisions on financial aid eligibility.<br />
Note: A tuition refund/credit appeal is a separate request submitted to the Business Services Office no later than 45 days after the end of the term or<br />
September 25 th for summer terms.<br />
Note: Request must be submitted no later than one calendar year from the last day of the semester of occurrence.<br />
_______ Initial here indicating you have read the notes above<br />
I. <strong>St</strong>udent Information<br />
<strong>St</strong>udent Name:<br />
Last<br />
Address:<br />
First<br />
SCSU ID:<br />
<strong>St</strong>reet City <strong>St</strong>ate Zip<br />
Day Phone: ( ) SCSU Email:<br />
Term / Year of Occurrence (example: Fall, 2010)<br />
II. Check either A or B<br />
A. Request to withdraw from all<br />
courses this term<br />
Submit to: Office of Academic Affairs<br />
Administrative Services 209<br />
<strong>St</strong>. <strong>Cloud</strong> <strong>St</strong>ate <strong>University</strong><br />
720 4th Avenue South<br />
<strong>St</strong> <strong>Cloud</strong> MN 56301-4498<br />
Fax: 320-308-5292<br />
Phone: 320-308-3143<br />
B. Request to withdraw from<br />
individual courses this term or<br />
from a course in a previous term<br />
Course(s) under request<br />
Course ID<br />
(Ex:000243)<br />
Dept.<br />
(ENGL)<br />
Number<br />
(191)<br />
Section<br />
(01)<br />
Credits<br />
(4)<br />
Submit to: Dean’s Office of the college/school of major/intended major:<br />
College of Liberal Arts, Kiehle Visual Arts Center 111<br />
School of Arts, Kiehle Visual Arts Center 111<br />
College of Science and Engineering, Wick Science Building 145<br />
School of Education, Education Building A110<br />
Herberger Business School, Centennial Hall 118<br />
School of Public Affairs, Whitney House 101<br />
School of Health and Human Services, <strong>St</strong>ewart Hall 365<br />
To be completed by instructor:<br />
Last date of<br />
attendance<br />
(required)<br />
Support for request<br />
Signature<br />
__________ _______ ______ ______ ______ ____________ ___Yes ___No ___Neutral _______________________<br />
__________ _______ ______ ______ ______ ____________ ___Yes ___No ___Neutral _______________________<br />
__________ _______ ______ ______ ______ ____________ ___Yes ___No ___Neutral _______________________<br />
III. Extenuating Circumstances (petitions without documented extenuating circumstances will be denied)<br />
____Medical: Documentation of the student’s treatment from a medical or mental health professional, on letterhead, including the<br />
dates of treatment and a telephone number for verification, is required. Medical reasons include serious illness or injury,<br />
mental health treatment, hospitalization, or other care received by the student that prohibits successful completion of the term.<br />
____Call to Active Duty of Armed Forces: Documentation in the form of the call up notice to active duty is required.<br />
____Other: Attach a letter that describes the extenuating circumstances and attach appropriate supporting documentation.<br />
(For example, death or illness of a family member or other significant hardship, etc.)<br />
<strong>St</strong>udent Signature Date ___________<br />
I certify that all information provided is true and correct.<br />
The student will receive written notification of the decision.<br />
****************************************<strong>University</strong> and College Use Only****************************************<br />
Request result: ____Approved ____Denied<br />
Issued by Office for Academic Affairs July 2012<br />
Signature _______________________________________________<br />
Title ________________________________Date _______________<br />
(Please forward to Office for Academic Affairs)
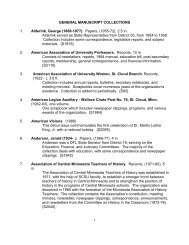
<strong>St</strong>. <strong>Cloud</strong> <strong>St</strong>ate <strong>University</strong><br />
<strong>Late</strong> <strong>Withdrawal</strong> Policy<br />
A late withdrawal is a request to withdraw from a class after the published withdrawal deadline and is<br />
considered only for extenuating circumstances. Typically, requests must be submitted no later than<br />
one calendar year from the last day of the semester of occurrence.<br />
Procedures for Requesting<br />
Consideration of <strong>Late</strong> <strong>Withdrawal</strong>s<br />
<br />
<br />
<br />
<br />
Typically, requests for late withdrawals should be submitted in the semester of occurrence but<br />
no later than one calendar year from the last day of the semester of occurrence. A request for<br />
late withdrawal from an individual course should be submitted to the office of the college or<br />
school offering the course. A request for late withdrawal from all courses should be submitted<br />
to the Office of Academic Affairs. A late withdrawal will be considered only if there are<br />
significant circumstances beyond the student’s control which affected the ability to complete<br />
the course. The circumstances must be documented. Requests without appropriate<br />
documentation or without extenuating circumstances will not be considered. Please refer to the<br />
<strong>Late</strong> <strong>Withdrawal</strong> <strong>Form</strong> for examples. <strong>Form</strong>s are available at various locations, including college<br />
offices and the Office of Academic Affairs.<br />
If permission for a <strong>Late</strong> <strong>Withdrawal</strong> is not granted, the earned grade will appear on the<br />
transcript. If permission is granted, a “W” will appear on the transcript.<br />
All Federal and <strong>St</strong>ate policies and procedures regarding financial aid eligibility will be enforced.<br />
<strong>St</strong>udents with financial aid in the form of scholarships, grants or loans may be required to<br />
repay the award if they withdraw or change course load. <strong>St</strong>udents are advised to contact the<br />
Business Services Office (AS 123) and Financial Aid Office (AS 106) before withdrawing from<br />
any class.<br />
Requests for refund/credit will be submitted to the Business Services Office (AS 123) no later<br />
than 45 days after the end of the term or September 25 th for summer terms.<br />
Issued by Office for Academic Affairs<br />
July 2012
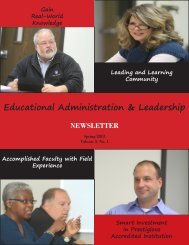
MEDICAL VERIFICATION FORM<br />
FOR ACADEMIC APPEALS AND REQUESTS FOR ACADEMIC CHANGE<br />
ST. CLOUD STATE UNIVERSITY<br />
720 Fourth Avenue South<br />
<strong>St</strong>. <strong>Cloud</strong>, MN 56301-4498<br />
<strong>St</strong>udent: If you have medical or psychological issues as reasons for an academic appeal or<br />
other academic change, it is necessary to have your medical/psychological provider verify the<br />
extenuating circumstances that are explained in your request. It is not necessary to supply full<br />
medical records. The provider information on this form must be returned with your appeal or<br />
academic change request.<br />
Please sign and date this form which acknowledges that you give permission to your<br />
medical/psychological provider to furnish the required information below.<br />
<strong>St</strong>udent Information:<br />
<strong>St</strong>udent Name: ______________________________________ ID: _____________________<br />
<strong>St</strong>udent Signature: ___________________________________ Date: __________________<br />
Office/Dept./College receiving your request: ________________________________________<br />
If the health care provider prefers to mail or fax the information, complete the following:<br />
Office/Department Name: _______________________________________________________<br />
Building & Room No: __________________________________________________________<br />
Phone (optional): (______) _______________ Fax (optional): (_______) _________________<br />
Mailing Address: (Office/Dept.), (Bldg./Rm. No.),<br />
<strong>St</strong>. <strong>Cloud</strong> <strong>St</strong>ate <strong>University</strong>, 720 Fourth Avenue South, <strong>St</strong>. <strong>Cloud</strong>, MN 56301-4498<br />
Semester(s) and class(es) impacted by medical/psychological condition being<br />
documented (to be completed by student):<br />
Entire semester (indicate semester and year (Ex. Fall 2012)<br />
Fall______ Spring ______ Summer I ______ Summer II _______<br />
OR List individual classes under request:<br />
Course ID Dept. Number Section Credits Course Name<br />
(Ex: 000243) (ENGL) (191) (01) (4)<br />
____________ ______ _____ _____ ____ _____________________________________<br />
____________ ______ _____ _____ ____ _____________________________________<br />
____________ ______ _____ _____ ____ _____________________________________<br />
____________ ______ _____ _____ ____ _____________________________________<br />
11/02/2012 Page 1 of 2
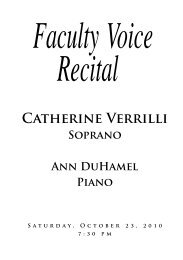
MEDICAL VERIFICATION FORM (continued)<br />
Provider Instructions:<br />
The student named above is requesting documentation for extenuating circumstances that have<br />
impacted their academic performance. The nature of the request and the permission to release<br />
information are at the top of this form.<br />
Please reply to the questions in the box below. You may supply this on your office letterhead,<br />
print this form on your letterhead or supply the necessary contact information below. If not on<br />
letterhead, please include your office stamp or seal or business card.<br />
Thank you for your assistance.<br />
Provider Name: ______________________________________________________________<br />
Contact information: ___________________________________________________________<br />
Provider Signature: _________________________________________ Date: _____________<br />
Provider: This <strong>St</strong>. <strong>Cloud</strong> <strong>St</strong>ate <strong>University</strong> student is asking to withdraw from one or more<br />
classes or appeal an academic issue because of a medical/psychological condition for which<br />
you have treated them.<br />
Please fill out the following portion of this form in its entirety to assist the student in the<br />
withdrawal process.<br />
Medical/psychological condition (brief description): ___________________________________<br />
____________________________________________________________________________<br />
____________________________________________________________________________<br />
Date of onset of condition: ______________________ Duration of condition:_______________<br />
Dates of visits for this condition: __________________________________________________<br />
In your professional opinion would the above condition for which you have treated the student<br />
prevent a student from attending class sessions in a <strong>University</strong> setting? Yes No<br />
Please identify the dates or duration for which attendance may be impacted: _________________<br />
In your professional opinion would the above condition for which you have treated the student<br />
prevent completion of coursework in a <strong>University</strong> setting for the above time periods? Yes No<br />
Please identify the dates or duration for which coursework may be impacted: _________________<br />
____________________________________________________________________________<br />
11/02/2012 Page 2 of 2