

Assessment of Adverse Events in the Demise of Pediatric Burn ...
Assessment of Adverse Events in the Demise of Pediatric Burn ...
Assessment of Adverse Events in the Demise of Pediatric Burn ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Adverse</strong> <strong>Events</strong> <strong>in</strong> <strong>Burn</strong> Care<br />
rema<strong>in</strong><strong>in</strong>g autopsy was performed by <strong>the</strong> county coroner. In<br />
addition to <strong>the</strong> autopsy f<strong>in</strong>d<strong>in</strong>gs, <strong>the</strong> pathologist also reviewed<br />
each patient’s hospital records and reported a summary<br />
<strong>of</strong> <strong>the</strong> cl<strong>in</strong>ical course for each patient. These cl<strong>in</strong>ical<br />
case summaries were available for all 72 deaths. For all<br />
admissions to <strong>the</strong> Shr<strong>in</strong>ers hospital dur<strong>in</strong>g this 10-year <strong>in</strong>terval,<br />
patient characteristics and demographics were available<br />
on computerized hospital records.<br />
Review Process<br />
After approval from <strong>the</strong> Institutional Review Board, autopsies<br />
and cl<strong>in</strong>ical course records were reviewed by four<br />
surgeons, all <strong>of</strong> whom have experience <strong>in</strong> burn care; three<br />
hav<strong>in</strong>g completed postresidency fellowships <strong>in</strong> burn care at a<br />
Shr<strong>in</strong>ers Hospitals for Children, <strong>the</strong> o<strong>the</strong>r with fellowship<br />
tra<strong>in</strong><strong>in</strong>g <strong>in</strong> pediatric surgery and with more than 10 years<br />
experience as a physician consultant at <strong>the</strong> Shr<strong>in</strong>ers Hospitals<br />
for Children. Us<strong>in</strong>g a standardized form, each reviewer was<br />
asked to note <strong>the</strong> probable cause <strong>of</strong> death and any associated<br />
factors contribut<strong>in</strong>g to death. Reviewers were also asked to<br />
scale <strong>the</strong> contribution <strong>of</strong> any deficiencies <strong>in</strong> care to <strong>the</strong> cause<br />
<strong>of</strong> death, from 1 (denot<strong>in</strong>g no error) to 4 (denot<strong>in</strong>g a significant<br />
impact <strong>of</strong> negligence on <strong>the</strong> child’s death). Also scaled<br />
from 1 to 4 by each reviewer were (1) <strong>the</strong> percent chance that<br />
a misadventure caused death and (2) <strong>the</strong> possibility <strong>of</strong> surviv<strong>in</strong>g<br />
to discharge had <strong>the</strong> error not occurred. For grad<strong>in</strong>g<br />
items 1 and 2, reviewers agreed on <strong>the</strong> follow<strong>in</strong>g scale: 1 <br />
0% to 15%, 2 16% to 50%, 3 51% to 84%, and 4 85%<br />
to 100%. Each reviewer was screened from <strong>the</strong> decisions <strong>of</strong><br />
<strong>the</strong> o<strong>the</strong>r reviewers.<br />
Statistics<br />
Patient characteristics between survivors and deaths<br />
were compared us<strong>in</strong>g a Student’s <strong>in</strong>dependent t test. Differences<br />
<strong>in</strong> <strong>the</strong> <strong>in</strong>cidence <strong>of</strong> <strong>in</strong>halation <strong>in</strong>jury between survivors<br />
and deaths were assessed us<strong>in</strong>g 2 . Median values between<br />
raters were used to report <strong>the</strong> <strong>in</strong>cidence <strong>of</strong> an event. Median<br />
and mean values corresponded closely for all variables, so mean<br />
values are not reported. Inter-rater agreement was assessed us<strong>in</strong>g<br />
simultaneous -statistics for variables that had an <strong>in</strong>cidence <strong>of</strong> at<br />
least 10%. values <strong>of</strong> greater than 0.7 were considered significant<br />
and <strong>in</strong>dicative <strong>of</strong> strong <strong>in</strong>ter-rater agreement.<br />
RESULTS<br />
The overall mortality for all hospital admissions dur<strong>in</strong>g<br />
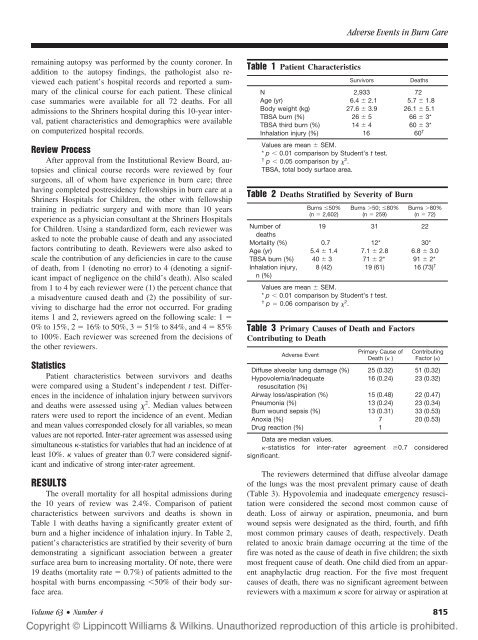
<strong>the</strong> 10 years <strong>of</strong> review was 2.4%. Comparison <strong>of</strong> patient<br />
characteristics between survivors and deaths is shown <strong>in</strong><br />
Table 1 with deaths hav<strong>in</strong>g a significantly greater extent <strong>of</strong><br />
burn and a higher <strong>in</strong>cidence <strong>of</strong> <strong>in</strong>halation <strong>in</strong>jury. In Table 2,<br />
patient’s characteristics are stratified by <strong>the</strong>ir severity <strong>of</strong> burn<br />
demonstrat<strong>in</strong>g a significant association between a greater<br />
surface area burn to <strong>in</strong>creas<strong>in</strong>g mortality. Of note, <strong>the</strong>re were<br />
19 deaths (mortality rate 0.7%) <strong>of</strong> patients admitted to <strong>the</strong><br />
hospital with burns encompass<strong>in</strong>g 50% <strong>of</strong> <strong>the</strong>ir body surface<br />
area.<br />
Table 1 Patient Characteristics<br />
Survivors<br />
Deaths<br />
N 2,933 72<br />
Age (yr) 6.4 2.1 5.7 1.8<br />
Body weight (kg) 27.6 3.9 26.1 5.1<br />
TBSA burn (%) 26 5 66 3*<br />
TBSA third burn (%) 14 4 60 3*<br />
Inhalation <strong>in</strong>jury (%) 16 60 †<br />
Values are mean SEM.<br />
* p 0.01 comparison by Student’s t test.<br />
† p 0.05 comparison by 2 .<br />
TBSA, total body surface area.<br />
Table 2 Deaths Stratified by Severity <strong>of</strong> <strong>Burn</strong><br />
<strong>Burn</strong>s 50%<br />
(n 2,602)<br />
<strong>Burn</strong>s 50; 80%<br />
(n 259)<br />
<strong>Burn</strong>s 80%<br />
(n 72)<br />
Number <strong>of</strong><br />
19 31 22<br />
deaths<br />
Mortality (%) 0.7 12* 30*<br />
Age (yr) 5.4 1.4 7.1 2.8 6.8 3.0<br />
TBSA burn (%) 40 3 71 2* 91 2*<br />
Inhalation <strong>in</strong>jury,<br />
n (%)<br />
8 (42) 19 (61) 16 (73) †<br />
Values are mean SEM.<br />
* p 0.01 comparison by Student’s t test.<br />
† p 0.06 comparison by 2 .<br />
Table 3 Primary Causes <strong>of</strong> Death and Factors<br />
Contribut<strong>in</strong>g to Death<br />
<strong>Adverse</strong> Event<br />
Primary Cause <strong>of</strong><br />
Death ( )<br />
Contribut<strong>in</strong>g<br />
Factor ()<br />
Diffuse alveolar lung damage (%) 25 (0.32) 51 (0.32)<br />
Hypovolemia/<strong>in</strong>adequate<br />
16 (0.24) 23 (0.32)<br />
resuscitation (%)<br />
Airway loss/aspiration (%) 15 (0.48) 22 (0.47)<br />
Pneumonia (%) 13 (0.24) 23 (0.34)<br />
<strong>Burn</strong> wound sepsis (%) 13 (0.31) 33 (0.53)<br />
Anoxia (%) 7 20 (0.53)<br />
Drug reaction (%) 1<br />
Data are median values.<br />
-statistics for <strong>in</strong>ter-rater agreement 0.7 considered<br />
significant.<br />
The reviewers determ<strong>in</strong>ed that diffuse alveolar damage<br />
<strong>of</strong> <strong>the</strong> lungs was <strong>the</strong> most prevalent primary cause <strong>of</strong> death<br />
(Table 3). Hypovolemia and <strong>in</strong>adequate emergency resuscitation<br />
were considered <strong>the</strong> second most common cause <strong>of</strong><br />
death. Loss <strong>of</strong> airway or aspiration, pneumonia, and burn<br />
wound sepsis were designated as <strong>the</strong> third, fourth, and fifth<br />
most common primary causes <strong>of</strong> death, respectively. Death<br />
related to anoxic bra<strong>in</strong> damage occurr<strong>in</strong>g at <strong>the</strong> time <strong>of</strong> <strong>the</strong><br />
fire was noted as <strong>the</strong> cause <strong>of</strong> death <strong>in</strong> five children; <strong>the</strong> sixth<br />
most frequent cause <strong>of</strong> death. One child died from an apparent<br />
anaphylactic drug reaction. For <strong>the</strong> five most frequent<br />
causes <strong>of</strong> death, <strong>the</strong>re was no significant agreement between<br />
reviewers with a maximum score for airway or aspiration at<br />
Volume 63 • Number 4 815
