facility network request form - Ubhonline.com
facility network request form - Ubhonline.com
facility network request form - Ubhonline.com

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
PLEASE COMPLETE AND FAX THIS DOCUMENT TO YOUR UBH/OPTUMHEALTH<br />
NETWORK MANAGEMENT STAFF<br />
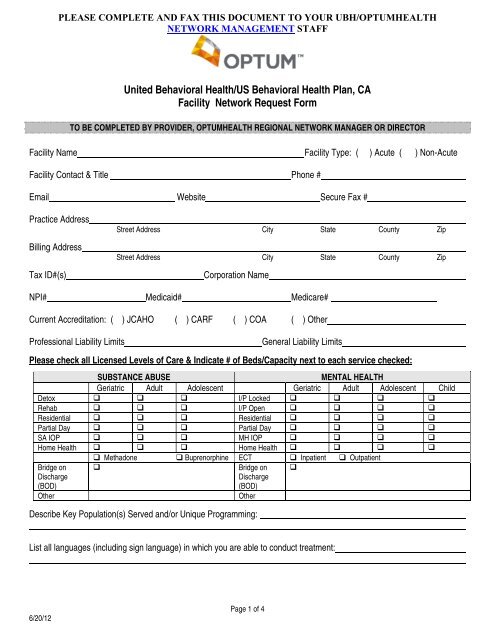
United Behavioral Health/US Behavioral Health Plan, CA<br />
Facility Network Request Form<br />
TO BE COMPLETED BY PROVIDER, OPTUMHEALTH REGIONAL NETWORK MANAGER OR DIRECTOR<br />
Facility Name Facility Type: ( ) Acute ( ) Non-Acute<br />
Facility Contact & Title Phone #<br />
Email Website Secure Fax #<br />
Practice Address<br />
Billing Address<br />
Tax ID#(s)<br />
Street Address City State County Zip<br />
Street Address City State County Zip<br />
Corporation Name<br />
NPI# Medicaid# Medicare#<br />
Current Accreditation: ( ) JCAHO ( ) CARF ( ) COA ( ) Other<br />
Professional Liability Limits<br />
General Liability Limits<br />
Please check all Licensed Levels of Care & Indicate # of Beds/Capacity next to each service checked:<br />
SUBSTANCE ABUSE<br />
MENTAL HEALTH<br />
Geriatric Adult Adolescent Geriatric Adult Adolescent Child<br />
Detox I/P Locked <br />
Rehab I/P Open <br />
Residential Residential <br />
Partial Day Partial Day <br />
SA IOP MH IOP <br />
Home Health Home Health <br />
Methadone Buprenorphine ECT Inpatient Outpatient<br />
Bridge on <br />
Bridge on <br />
Discharge<br />
(BOD)<br />
Discharge<br />
(BOD)<br />
Other<br />
Other<br />
Describe Key Population(s) Served and/or Unique Programming:<br />
List all languages (including sign language) in which you are able to conduct treatment:<br />
6/20/12<br />
Page 1 of 4
PLEASE COMPLETE AND FAX THIS DOCUMENT TO YOUR UBH/OPTUMHEALTH<br />
NETWORK MANAGEMENT STAFF<br />
List Attending Physicians and/or Attach Staff Roster:<br />
Are the attending physicians employed by the <strong>facility</strong>? ( ) Yes ( ) No<br />
Provide the names of the primary attending MD’s at your <strong>facility</strong>:<br />
How many single case agreements have you made with UBH in the last 6 months?<br />
List and/or Attach Current Managed Care Participation<br />
Provide the most recent 4 quarters of average length of stay (ALOS) experience for the levels of care (LOC) your <strong>facility</strong><br />
offers (for managed care members only): Inpatient Residential Partial IOP<br />
NOTE: If you are a NEW <strong>facility</strong>, please <strong>com</strong>plete the in<strong>form</strong>ation below<br />
Facility Practices<br />
1. Pre-Certification:<br />
A) Please provide a brief description of the <strong>facility</strong>’s Intake/Pre-Certification process.<br />
B) Can a call be made to UBH from Admission upon Assessment? Yes No<br />
C) How do they assign attending physicians?<br />
D) Will they assign members to UBH contracted physicians? Yes No<br />
E) Do they have personnel and a process to assure pre-cert on nights and<br />
Yes No<br />
weekends?<br />
2. UR Process/Treatment Planning<br />
A) Provide copy of UBH Initial Review In<strong>form</strong>ation to <strong>facility</strong>.<br />
Would staff be willing to use the UBH Initial Review template? Yes No<br />
B) Does staff conduct individualized treatment planning? Please describe.<br />
C) Does staff include family involvement or therapy in treatment? How soon, how often?<br />
D) Please describe the UR process. Do the UR staff round with the MDs?<br />
E) What is the <strong>facility</strong>’s process regarding peer to peers?<br />
F) How soon do they begin discharge planning?<br />
6/20/12<br />
Page 2 of 4
PLEASE COMPLETE AND FAX THIS DOCUMENT TO YOUR UBH/OPTUMHEALTH<br />
NETWORK MANAGEMENT STAFF<br />
3. Continuity and Coordination of Care:<br />
A) How does the <strong>facility</strong> <strong>com</strong>municate with outpatient mental health providers?<br />
B) How does the <strong>facility</strong> <strong>com</strong>municate with PCPs or other medical providers?<br />
C) What is the <strong>facility</strong>’s process to research and resolve member generated <strong>com</strong>plaints?<br />
D) Any other questions from the <strong>facility</strong>?<br />
4. Program/Services:<br />
A) Does the <strong>facility</strong> have appropriate step-down options? Please describe.<br />
B) Does the <strong>facility</strong> have age/specialty specific LOCs? Yes No<br />
If yes, please describe treatment and staffing for programs.<br />
5. Discharge Plan/Ambulatory follow-up:<br />
A) Please describe the <strong>facility</strong>’s discharge plan/program.<br />
B) Is the <strong>facility</strong> able to schedule follow-up appointments within 7 days? Yes No<br />
If no, what are the barriers?<br />
6. Readmission:<br />
A) What is the <strong>facility</strong> readmission rate? (Target: less than 12%)<br />
B) Do they have a plan to address relapse prevention? Yes No<br />
If yes, please describe.<br />
7. Collaboration:<br />
A) What has been their experience in working with managed care?<br />
B) Do they have any current workflows that would be helpful to UBH or the delivery of care?<br />
C) What is the <strong>facility</strong>’s process to research and resolve member generated <strong>com</strong>plaints?<br />
D) Any other questions from the <strong>facility</strong>?<br />
8. UBH Guidelines<br />
A) Have you reviewed the UBH Best Practice/Level of Care Guidelines? Yes No<br />
Any Questions or Concerns?<br />
6/20/12<br />
Page 3 of 4
PLEASE COMPLETE AND FAX THIS DOCUMENT TO YOUR UBH/OPTUMHEALTH<br />
NETWORK MANAGEMENT STAFF<br />
B) Have you reviewed the Facility Manual? Yes No<br />
Any Questions or Concerns?<br />
Facility Name:<br />
Facility Authorized Signature<br />
Print Name:<br />
Title:<br />
Date:<br />
For Internal Use Only:<br />
Network Manager Signature: ____________________________Date Received:___________ # of Covered Lives:_______________<br />
Date Routed to Care Advocacy Center: ______________________________________________________________( ) Fax ( )Mail<br />
Signature of CAC Representative (approval to panel <strong>facility</strong>): ________________________________________Date:_____________<br />
Date Routed to Facility Contracting: _________________________________________________________________( ) Fax ( ) Mail<br />
6/20/12<br />
Page 4 of 4