View Video Transcript - Joint Commission
View Video Transcript - Joint Commission
View Video Transcript - Joint Commission

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
2012 5th International High Reliability Organizing Conference:<br />
Seeking Reliability through Operations, Attitudes,<br />
and Measuring Success<br />
Dr. Mark R. Chassin<br />
Keynote Address<br />
May 21, 2012<br />
Part III<br />
Robust process improvement and the Center for Transforming Healthcare<br />
So what we mean by RPI (Robust Process Improvement) are the three different tool chests that we<br />
believe need to come together to support the creation of nearly perfect processes — Lean, Six Sigma and<br />
change management, three tool chests inside the RPI tool shed, if you will. I know it's a cumbersome<br />
metaphor, but it's the only one I can come up with so far. Each of these tool chests has specific tools and<br />
methods and strategies for making health care processes, and any process, more effective.<br />
We are in the middle of a very aggressive program inside The <strong>Joint</strong> <strong>Commission</strong> to adopt all of these<br />
tools and train all thousand of our workforce in them at levels that are appropriate for their jobs. It helps<br />
us with our own business processes. It helps us focus on our customers, as those of you that are expert<br />
in these tools know. And we are also adopting all of the components of a safety culture. We measure<br />
both of these, and we report them to our board as part of our strategic plan and our strategic metric so<br />
that our board can see how well we're doing in achieving the goals of adopting safety culture and RPI.<br />
Now, we are doing this to improve our business, and it's already had a dramatic impact, including with a<br />
positive ROI, although that wasn't our primary purpose. But we also did this because we wanted to apply<br />
these tools with healthcare organizations that had also mastered them in order to tackle some of the most<br />
resistant quality and safety problems that we have. And we created a new part of The <strong>Joint</strong> <strong>Commission</strong><br />
called the Center for Transforming Healthcare in order to do that. And you probably can't read that little<br />
tagline under the Center's name which says "Creating solutions for high reliability health care."<br />
So this is the RPI component of getting to high reliability. How do we create these processes with<br />
defenses that have minuscule holes in them? How do we create safety protocols that work not 40 or 50<br />
percent of the time but 90, 95 percent of the time, at least? And we are not very good at doing that today<br />
in health care.<br />
The Center was created not only because we thought these tools would work but because our customers<br />
were asking us for solutions to the same safety and quality problems that The <strong>Joint</strong> <strong>Commission</strong> has<br />
been talking about for years. The <strong>Joint</strong> <strong>Commission</strong> discovered wrong-site surgery in 1995 — not solved.<br />
We are committed to delivering the products of the Center. Now, three years later, we're still committed,<br />
at no added cost to our accredited customers. As part of accreditation, we've raised now about $33<br />
million from — both from The <strong>Joint</strong> <strong>Commission</strong> but from other major donors. Each of these farsighted<br />
organizations — from the American Hospital Association to Medline, Cardinal Health, the Blue Cross Blue<br />
2012 5th International HRO Conference, Chicago, Illinois The <strong>Joint</strong> <strong>Commission</strong><br />
Dr. Mark R. Chassin: Keynote Address, May 21, 2012 Page 1
Shield Association — has contributed $1 million or more to the Center. And we are continuing down this<br />
road.<br />
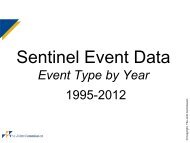
We've tackled a large number of problems using these tools. This year we will launch a project on sepsis<br />
and a medication safety project and a third one before the end of the year. And this is the list of hospitals<br />
and systems that has joined with us to tackle these problems. Some have been involved in three or four<br />
projects. And we are recruiting more all the time. We'll probably add another three or four this year.<br />
These organizations have been recruited because they know how to use Lean, Six Sigma and change<br />
management. And we can do these projects essentially on business time frames — well, close to<br />
business time frames. Most of us are not-for-profits, so we're not used to for-profit business time frames.<br />
But these are not training exercises, is my point. We apply the tools and we generate generalizable<br />
knowledge.<br />
Now, I said these problems have been with us for a long time. And they've been with us despite at least a<br />
decade in which health care has focused a lot of effort and energy to solving. Why haven't they been<br />
solved? Well, I think one of the questions we have to ask is, what improvement model have we been<br />
throwing at these problems over this decade? And pretty much it's been a single note or slight variations<br />
on a single note. We find somebody that says they've solved a problem, and we say, "Oh, that's a best<br />
practice. Let's make a toolkit, a checklist, a protocol out of that. We'll call it a bundle. Everybody should do<br />
it the same way, and the problem will be solved everywhere." Right? How is that working out?<br />
Well, I know it wasn't working out very well when I was on the hospital side trying this five, six years ago.<br />
And we thought there's probably a better way. And, in fact, when you look carefully at this approach, it<br />
does work in certain very narrowly circumscribed situations. It's worked to get rid of — almost get rid of<br />
ICU infections from central lines. It's worked to drastically reduce ventilator-associated pneumonia. But<br />
they produce these results only when the process you're trying to fix doesn't vary very much from one<br />
place to another and when the causes of failure are few and easily identified.<br />
Now, none of the problems on the previous slide have any of those characteristics. They are much more<br />
complicated, and they require more sophisticated problem-solving approaches, ones that use RPI.<br />
Complicated processes are not solved with simple solutions. It turns out there are many causes of failure<br />
for these processes, not just four or five, but 15, 18, 20, 25, when you look carefully. Each cause typically<br />
requires a very different strategy to get rid of. And another critical finding of this work is that when you<br />
look at one place and find the four or five critical causes that explain half of the failures and you look at<br />
place number two, you don't find the same critical few causes, you find different ones, which is a big<br />
reason why the same best practice, even if it really did a good job over here, is not going to work in the<br />
second place.<br />
So we believe that the next generation of best practices, using these very effective process improvement<br />
tools, will produce solutions that are customized to an organization's specific and important causes of the<br />
problem, which will vary from one place to another.<br />
2012 5th International HRO Conference, Chicago, Illinois The <strong>Joint</strong> <strong>Commission</strong><br />
Dr. Mark R. Chassin: Keynote Address, May 21, 2012 Page 2