Section 12 Vascular Access for Hemodialysis - American ...
Section 12 Vascular Access for Hemodialysis - American ...
Section 12 Vascular Access for Hemodialysis - American ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Section</strong> <strong>12</strong><br />
<strong>Vascular</strong> <strong>Access</strong><br />
<strong>for</strong> <strong>Hemodialysis</strong><br />
Lesley C. Dinwiddie, MSN, RN, FNP, CNN
<strong>Section</strong> <strong>12</strong>. <strong>Vascular</strong> <strong>Access</strong> <strong>for</strong> <strong>Hemodialysis</strong><br />
About the Author<br />
Lesley C. Dinwiddie, MSN, RN, FNP, CNN, <strong>Section</strong> Editor and Author, is<br />
a Nephrology Nurse Consultant at <strong>Vascular</strong> <strong>Access</strong> Education and<br />
Research in Cary, North Carolina, and the Executive Director <strong>for</strong> the<br />
Institute of Excellence, Education and Research (ICEER).<br />
736<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008
<strong>Section</strong> <strong>12</strong><br />
<strong>Vascular</strong> <strong>Access</strong> <strong>for</strong><br />
<strong>Hemodialysis</strong><br />
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 738<br />
Historical Perspectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 739<br />
Chapter<br />
58 Patient Evaluation <strong>for</strong> Long-term <strong>Access</strong> Selection . . . . . . . . . . . . . . . . . 740<br />
59 <strong>Vascular</strong> <strong>Access</strong> Type and Site of Placement . . . . . . . . . . . . . . . . . . . . . . . 741<br />
60 Nursing Process in the Routine Care of <strong>Vascular</strong> <strong>Access</strong> . . . . . . . . . . . . 752<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008 737
<strong>Section</strong> <strong>12</strong>. <strong>Vascular</strong> <strong>Access</strong> <strong>for</strong> <strong>Hemodialysis</strong><br />
<strong>Section</strong><br />
<strong>12</strong><br />
<strong>Vascular</strong> <strong>Access</strong> <strong>for</strong> <strong>Hemodialysis</strong><br />
Purpose<br />
The purpose of this section is to provide an overview of the commonly used<br />
types of vascular access <strong>for</strong> hemodialysis as well as the nursing process necessary<br />
to assure the following patient outcomes (Burrows-Hudson & Prowant, 2005):<br />
1. The patient’s vascular access will provide a blood flow rate adequate to<br />
achieve the dialysis prescription.<br />
2. The patient’s vascular access will have a long use-life and be free of<br />
complications.<br />
3. The patient will demonstrate knowledge regarding his/her vascular access.<br />
Objectives<br />
Upon completion of this section, the learner will be able to:<br />
1. List the preferential order <strong>for</strong> vascular access according to the 2006 KDOQI<br />
guidelines and compare the indications, locations, advantages, and<br />
disadvantages of the arteriovenous fistula (AVF); the arteriovenous graft<br />
(AVG); and the central venous catheter (CVC) and catheter/port devices.<br />
2. State the steps <strong>for</strong> assessment <strong>for</strong> each type of access.<br />
3. List the possible causes and diagnoses of complications.<br />
4. Describe routine planning <strong>for</strong> management of the vascular access, implementation<br />
(including cannulation), and interventions <strong>for</strong> complications.<br />
5. Define the ongoing evaluation by the vascular access team through<br />
continuous quality improvement (CQI) and:<br />
a. Patient education.<br />
b. Staff education.<br />
c. Data collection and analyses.<br />
Introduction<br />
<strong>Vascular</strong> access is essential to hemodialysis (HD) therapy. Positive patient<br />
outcomes <strong>for</strong> hemodialysis are highly dependent on complication-free<br />
vascular access. The type of vascular access needed to achieve such outcomes<br />
depends upon the diagnosis and prognosis as well as the anatomic and<br />
physiologic potential and limitations of the patient. The ideal blood flow<br />
through a patient’s fistula or graft is a flow sufficient to achieve prescribed blood<br />
flow rates through the dialyzer without compromising cardiac output or flow to<br />
the extremity distal to the access. While creation/placement of vascular access is<br />
primarily the purview of physicians, the routine maintenance, preservation, and<br />
patient education is the responsibility of the nephrology nurse.<br />
738<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008
Historical Perspectives<br />
Historical Perspectives<br />
1960 Scribner and Quinton developed the first<br />
permanent access <strong>for</strong> chronic hemodialytic<br />
therapy. It consisted of Teflon tubes, one placed<br />
in an artery and one in a vein, which exited<br />
through the skin and were joined by a Teflon<br />
loop by means of swedge locks. (The detailed<br />
in<strong>for</strong>mation on external AV shunts that has<br />
appeared in previous editions of the Core<br />
Curriculum has been archived to Historical<br />
Documents on the ANNA Web site,<br />
www.annanurse.org.)<br />
1961 Shaldon described a technique <strong>for</strong> cannulation<br />
of femoral veins.<br />
1962 Siliconized rubber used <strong>for</strong> external shunt loop<br />
and Teflon used <strong>for</strong> vessel tips. A curved loop<br />
connected the two cannulas <strong>for</strong>ming the shunt,<br />
which was specifically made <strong>for</strong> each patient.<br />
Siliconized rubber segments had steps and bends<br />
<strong>for</strong>med in them to make them more com<strong>for</strong>table<br />
<strong>for</strong> patients, and to extend the life of the shunt<br />
by bringing it back up to the limb and away<br />
from the joint (reverse-winged shunt).<br />
1966 Brescia and Cimino developed the internal<br />
arteriovenous (AV) fistula <strong>for</strong> repeated<br />
venipunctures <strong>for</strong> maintenance hemodialysis.<br />
1966 Ramirez developed the straight-winged shunt<br />
<strong>for</strong> better stabilization and easier declotting.<br />
1966 Buselmeier shunt developed.<br />
1972 Allen-Brown shunt developed.<br />
1974 Bovine carotid artery graft used <strong>for</strong> circulatory<br />
access.<br />
1975 Gore-tex® graft became commercially available<br />
<strong>for</strong> use as AV access <strong>for</strong> hemodialysis.<br />
1977 Umbilical cord vein used <strong>for</strong> AV graft.<br />
1977 Expanded polytetrafluoroethylene (ePTFE) used<br />
as AV conduit <strong>for</strong> hemodialysis.<br />
1979 Uldall developed a catheter that allowed repeated<br />
cannulation of subclavian vein <strong>for</strong> temporary<br />
access <strong>for</strong> hemodialysis; introduced the concept<br />
of subclavian vein as temporary access to avoid<br />
destruction of peripheral vessels that later may<br />
be needed <strong>for</strong> creation of permanent vascular<br />
access. This led to the development of subclavian<br />
and jugular vein catheters that could be used as<br />
permanent circulatory access <strong>for</strong> hemodialysis<br />
when peripheral vasculature was inadequate to<br />
support creation and patency of either an AV<br />
fistula or an AV graft.<br />
1980 Button needle-free vascular access <strong>for</strong> hemodialysis<br />
developed.<br />
1980 Interventional radiology procedures <strong>for</strong> the<br />
(circa) treatment of underlying anatomic stenotic<br />
lesions emerged.<br />
1980 Urokinase used <strong>for</strong> thrombolysis of AV access,<br />
(circa) especially catheters.<br />
1983 The tunneled, cuffed catheter <strong>for</strong> long-term<br />
hemodialysis access introduced.<br />
1997 National Kidney Foundation/Dialysis Outcome<br />
Quality Initiative (NKF-DOQI) Clinical Practice<br />
Guidelines published.<br />
1998 Trials began <strong>for</strong> subcutaneous port/catheter<br />
devices <strong>for</strong> hemodialysis.<br />
1999 Clinical Per<strong>for</strong>mance Measures (CPMs) based<br />
on the NKF-DOQI guidelines were introduced.<br />
1999 Centers dedicated to vascular access were<br />
established with many using interventional<br />
nephrologists.<br />
1999 Urokinase was removed from the market. Other<br />
lytics came to the <strong>for</strong>efront, most notably tissue<br />
plasminogen activator (tPA), to fill the need to<br />
lyse clot in thrombosed accesses.<br />
2001 The DOQI guidelines were revised and renamed<br />
the Kidney Disease Outcomes Quality Initiative<br />
(KDOQI). The most significant change in these<br />
<strong>Vascular</strong> <strong>Access</strong> guidelines was in the section on<br />
Monitoring and Surveillance.<br />
2003 The National <strong>Vascular</strong> <strong>Access</strong> Improvement<br />
Initiative (NVAII) began because the AVF<br />
growth and the catheter reduction goals in the<br />
KDOQI guidelines were not being realized. It<br />
soon came to be known as the Fistula First<br />
Program and in March 2005, this program was<br />
elevated by CMS to breakthrough initiative<br />
status and is now known as the Fistula First<br />
Breakthrough Initiative (FFBI).<br />
2006 The KDOQI guidelines <strong>for</strong> <strong>Vascular</strong> <strong>Access</strong> were<br />
revised with major <strong>for</strong>mat changes. There are<br />
now eight clinical practice guidelines (CPG) and<br />
a section <strong>for</strong> clinical practice recommendations<br />
(CPR) with specific recommendations <strong>for</strong><br />
pediatrics. The CPGs are evidence-based. The<br />
CPRs are supported by a combination of weaker<br />
evidence and expert opinion. Four topics were<br />
intensively reviewed and revised <strong>for</strong> this iteration<br />
and all others updated. While the goal <strong>for</strong> longterm<br />
catheter reduction (< 10%) is unchanged,<br />
the goal <strong>for</strong> AVFs, incident and prevalent, is now<br />
65% (NKF KDOQI, 2006, CPG 8). It is to be<br />
noted that the KDOQI guidelines are not<br />
standards of care.<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008 739
<strong>Section</strong> <strong>12</strong>. <strong>Vascular</strong> <strong>Access</strong> <strong>for</strong> <strong>Hemodialysis</strong><br />
Chapter 58<br />
Patient Evaluation <strong>for</strong><br />
Long-term <strong>Access</strong> Selection<br />
This chapter is based on NKF KDOQI, 2006, CPG 1.<br />
I. Patient history. To optimize the choice of access<br />
type and placement, the following factors must be<br />
assessed.<br />
A. Dominant arm.<br />
B. Exercise capacity and current arm strength<br />
training (Leaf et al., 2003; Oder et al., 2003).<br />
C. History of:<br />
1. Previous vascular catheters, peripheral or central.<br />
2. Previous vascular surgery <strong>for</strong> access.<br />
3. Needle phobia.<br />
4. Pacemaker or internal defibrillator.<br />
5. Other arm, neck, breast, chest surgery, or trauma.<br />
6. Any cardiovascular disease including stroke.<br />
7. Diabetes mellitus.<br />
8. Coagulopathies.<br />
9. Other life-threatening comorbidities (e.g.,<br />
malignancies).<br />
D. Current anticoagulation therapy.<br />
E. Kidney replacement therapy (KRT) modality plan.<br />
1. Scheduled transplant from a living donor.<br />
2. Potential candidate <strong>for</strong> peritoneal dialysis.<br />
3. Undergoing a trial of hemodialysis to help<br />
decide between KRT or palliative care option.<br />
II. Physical examination.<br />
A. Examine skin <strong>for</strong> scarring.<br />
B. Check arterial blood supply in all extremities,<br />
noting:<br />
1. Character of peripheral pulses.<br />
2. Color of digits.<br />
3. Temperature of hands and feet.<br />
4. Presence of lesions.<br />
5. Deficits in function.<br />
C. Per<strong>for</strong>m Allen test (see Table <strong>12</strong>.1).<br />
D. Listen to apical pulse <strong>for</strong> rate and rhythm.<br />
E. Measure bilateral upper arm blood pressures to<br />
detect differences in arterial flow.<br />
F. Examine venous drainage in all extremities.<br />
1. Compare both arms <strong>for</strong>:<br />
a. Presence and degree of edema.<br />
b. Differences in size (evidence of venous<br />
and/or lymphatic obstruction).<br />
c. Patency of veins noting compressibility and<br />
mobility of superficial veins in arms.<br />
d. Note degree of change in superficial vessels<br />
with application of tourniquet.<br />
2. Compare both legs <strong>for</strong>:<br />
a. Presence and degree of edema.<br />
Standards of Nursing Care <strong>for</strong> <strong>Vascular</strong> <strong>Access</strong><br />
The nephrology nurse:<br />
A. Assesses the patient and collects comprehensive data pertinent to the<br />
maturation or routine management of the access <strong>for</strong> HD therapy.<br />
B. Analyzes the assessment findings and/or data to determine normalcy of the<br />
access or the presence of pathology.<br />
C. Identifies expected individual patient outcomes.<br />
D. Develops a plan of care to attain the patient outcomes.<br />
E. Implements the plan by:<br />
1. Coordinating the delivery of care and assuring appropriate documentation.<br />
2. Providing patient education including self-management.<br />
F. Evaluates the status of the patient’s progress in attaining the stated outcomes<br />
individually and as part of the vascular access team using the CQI process.<br />
740<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008
Chapter 58. Patient Evaluation <strong>for</strong> Long-term <strong>Access</strong> Selection • Chapter 59. <strong>Vascular</strong> <strong>Access</strong> Type and Site of Placement<br />
Table <strong>12</strong>.1<br />
Allen Test<br />
III. Diagnostic evaluation.<br />
1. Patient clenches the fist of one hand to produce<br />
pallor in the hand.<br />
2. Clinician occludes arterial flow by compressing both<br />
radial and ulnar arteries.<br />
3. Patient opens clenched fist.<br />
4. Clinician releases pressure on the ulnar artery and<br />
counts the seconds required <strong>for</strong> color to return to the<br />
hand. More than 3 seconds indicates decreased ulnar<br />
arterial supply to the hand if the radial artery is used<br />
<strong>for</strong> the vascular access.<br />
5. Repeat the procedure, but release pressure on radial<br />
artery this time to assess radial arterial flow to hand.<br />
6. Repeat procedure with opposite hand.<br />
b. Difference in size (evidence of lymphatic<br />
and/or venous obstruction).<br />
c. Presence of varicosities.<br />
3. Look <strong>for</strong> swelling and presence of collateral<br />
veins in chest wall and neck indicating central<br />
venous obstruction.<br />
A. Duplex ultrasound mapping of the upper<br />
extremity arteries and veins <strong>for</strong> all patients.<br />
B. Central vein evaluation in the patient known<br />
to have:<br />
1. Previous catheter, pacemaker, and/or internal<br />
defibrillator.<br />
2. Edema or unilateral enlargement in the<br />
extremity of choice.<br />
3. Collateral veins above the planned access site.<br />
4. Evidence of any surgery or trauma to the neck,<br />
chest, breast, or arm involving the planned<br />
access vessels.<br />
C. Central venography can be accomplished with<br />
dilute contrast, CO 2 , magnetic resonance imaging<br />
(MRI), duplex ultrasound to avoid nephrotoxicity<br />
and preserve residual kidney function. However,<br />
gadolinium-based contrast agents <strong>for</strong> MRI should<br />
not be used in patients with CKD stage 4 or 5 due<br />
to risk of nephrogenic systemic fibrosis (NSF)<br />
(FDA, 2007).<br />
Chapter 59<br />
<strong>Vascular</strong> <strong>Access</strong> Type and Site of Placement<br />
This chapter is based on NKF KDOQI, 2006, CPG 2.<br />
<strong>Vascular</strong> access should be placed distally and in the<br />
upper extremities whenever possible. Because AVF<br />
provides the access with the longest patency rates and<br />
need <strong>for</strong> fewest interventions (Huber et al., 2003;<br />
NKF, 2006; Pisoni et al, 2002) options <strong>for</strong> AVF<br />
creation should be considered first, followed by<br />
prosthetic grafts, if AVF creation is not possible.<br />
Catheters should be avoided <strong>for</strong> HD and used only<br />
when the previous options are not possible, are<br />
contraindicated by the patient’s condition, or the<br />
access <strong>for</strong> hemodialysis is short-term.<br />
I. Arteriovenous fistulae (AVF).<br />
A. Definition. A surgically created opening between<br />
an artery anastomosed to a juxtapositional<br />
(nearby) vein allowing the high pressure arterial<br />
blood to flow into the vein causing engorgement,<br />
enlargement, and wall thickening. This process is<br />
known as arterialization or maturation of the vein<br />
and is necessary to provide a vessel with adequate<br />
flow <strong>for</strong> hemodialysis and sufficiently strong to<br />
effectively cannulate. The outflow vessel should be<br />
naturally superficial or surgically superficialized.<br />
The artery and the anastomosis site should never<br />
be cannulated. A variety of surgical anasomotic<br />
techniques are used to create the fistula and are<br />
illustrated in Figure <strong>12</strong>.1.<br />
B. Anatomic locations. The sites <strong>for</strong> creation of an<br />
AVF are limited only by the patient’s suitable<br />
vasculature and the skill and creativity of the<br />
clinicians creating and caring <strong>for</strong> it.<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008 741
<strong>Section</strong> <strong>12</strong>. <strong>Vascular</strong> <strong>Access</strong> <strong>for</strong> <strong>Hemodialysis</strong><br />
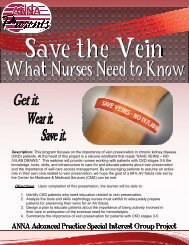
Figure <strong>12</strong>.1. Examples of various configurations <strong>for</strong> AV fistula anastomoses: (a) normal artery-vein<br />
relationship, (b) end-to-end anastomosis, (c) end-vein to side-artery anastomosis, (d) side-to-side<br />
anastomosis, (e) side-vein to end-artery anastomosis, (f) side-to-side converted to end-to-end anastomosis.<br />
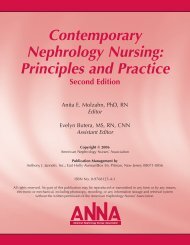
C. Placement in order of priority.<br />
1. A wrist (radial-cephalic) primary fistula (see<br />
Figure <strong>12</strong>.2).<br />
2. An elbow (brachial-cephalic) primary fistula.<br />
3. An upper arm (brachial-basilic) fistula with<br />
vein transposition.<br />
vein<br />
artery<br />
Figure <strong>12</strong>.2. Preferred site <strong>for</strong> fistula.<br />
Actual site may vary depending on patient.<br />
Used with permission from Arrow International Inc.<br />
D. Classification of AVFs. The traditional AVF (such<br />
as the radial-cephalic or brachial-cephalic) is<br />
created with just the construction of the AV<br />
anastomosis — a one-step procedure, sometimes<br />
known as a primary fistula. With the increased<br />
impetus to give priority to AVF creation, more<br />
innovative surgical techniques are being used to<br />
superficialize the outflow vein such as transposition<br />
(surgically dissecting out and tunneling in a<br />
superficial, accessible area of limb) of the vein or<br />
surgical removal of the tissue between the skin<br />
and the vein (Roberts, 2005). AVFs with vein<br />
transposition are frequently created with two<br />
separate procedures to allow <strong>for</strong> arterialization of<br />
the vein prior to superficialization.<br />
E. Indication <strong>for</strong> AVF creation. A fistula should be<br />
placed at least 6 months prior to the anticipated<br />
start of hemodialysis treatments. This timing<br />
allows <strong>for</strong> access evaluation and additional time<br />
<strong>for</strong> revision to ensure a working, fully functional<br />
fistula is available at initiation of dialysis (NKF<br />
KDOQI, 2006, CPG 1). Patients should be<br />
considered <strong>for</strong> construction of a fistula after<br />
failure of every dialysis AV access. In the patient<br />
per<strong>for</strong>ming PD, who is manifesting signs of<br />
modality failure, the decision to create a backup<br />
fistula should be individualized by periodically<br />
reassessing need (NKF KDOQI, 2006, CPG 2).<br />
742<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008
Chapter 59. <strong>Vascular</strong> <strong>Access</strong> Type and Site of Placement<br />
F. Advantages of AVF accesses.<br />
1. Have the lowest rate of thrombosis and require<br />
the fewest interventions, providing longer<br />
survival of the access (Huber et al., 2003; Pisoni<br />
et al., 2002).<br />
2. Have lower rates of infection than grafts<br />
(which, in turn, are less prone to infection than<br />
percutaneous catheters and subcutaneous port<br />
catheter systems).<br />
3. Cost of implantation and access maintenance<br />
are the lowest long-term.<br />
4. Are associated with increased survival (Dhingra<br />
et al., 2001) and lower hospitalization rates.<br />
5. Avoid the complications associated with the<br />
venous anastomosis in AVGs.<br />
6. Avoid potential <strong>for</strong> allergic response to<br />
synthetic materials.<br />
7. Outflow veins are autogenous tissue which seals<br />
and heals after cannulation. Synthetic grafts<br />
only seal by means of a fibrin plug.<br />
8. Can utilize the buttonhole cannulation technique.<br />
G. Disadvantages of AVF accesses.<br />
1. The vein may fail to enlarge or increase wall<br />
thickness (i.e., fail to mature). This may be caused<br />
by inadequate inflow or the presence of collateral<br />
or accessory veins that divert both volume and<br />
pressure from the intended outflow vein.<br />
2. AVFs have comparatively long maturation<br />
times. Weeks to months must elapse following<br />
creation of these fistulae be<strong>for</strong>e they can be<br />
used. If the access has not been created several<br />
weeks in advance of the anticipated need <strong>for</strong><br />
dialysis, an alternative method of vascular<br />
access must be used while the fistula matures.<br />
3. In some individuals, the vein may be more<br />
difficult to cannulate than an AVG.<br />
4. AVF creation and cannulation require different<br />
skill sets than <strong>for</strong> AVGs. Proficiency in one type<br />
of access does not assure proficiency in the other.<br />
5. Thrombosed AVF may be more difficult in<br />
which to restore flow.<br />
6. The enlarged vein may be visible, especially in<br />
the <strong>for</strong>earm and perceived as cosmetically<br />
unattractive by some individuals.<br />
7. A hypertrophied outflow vein may significantly<br />
increase cardiac output (in turn increasing<br />
cardiopulmonary recirculation), and myocardial<br />
load and may cause steal syndrome in patients<br />
with compromised peripheral vasculature.<br />
H. Complications of AVFs (KDOQI, 2006, CPG 5).<br />
1. Nonmaturing outflow vein and early failure.<br />
Primary nondevelopment of the outflow vein<br />
may be secondary to:<br />
a. Insufficient vasculature caused by poor<br />
arterial flow and/or small vein size.<br />
Signs and symptoms.<br />
(1) Minimal increase in vein size and bruit<br />
limited to anastomosis area.<br />
(2) Absence of palpable thrill and bruit by<br />
auscultation along the outflow vein.<br />
b. Treatment is surgical revision if possible.<br />
2. Disturbances in flow dynamics that are usually<br />
caused by venous stenosis (abnormal narrowing<br />
of the lumen of the vessel as a result of injury to<br />
the wall causing intimal hyperplasia). Related<br />
problems include:<br />
a. Venous hypertension: engorgement of vessels<br />
distal to anastomosis when resistance to flow<br />
is greater in proximal veins due to venous<br />
stenosis (Schanzer, 2002).<br />
b. Sore thumb syndrome: engorgement of<br />
thumb veins with sometimes painful<br />
throbbing or pulsating of distal veins and<br />
edema of thumb that may extend to entire<br />
hand; cyanotic nail bed with potential <strong>for</strong><br />
serous oozing if obstruction of venous<br />
capillary drainage continues (White, 2006).<br />
c. Increased venous return can cause arm,<br />
breast, neck, chest, and face swelling if<br />
stenosis develops in the central vessels.<br />
3. <strong>Access</strong>ory veins: arterial flow through multiple<br />
outflow veins prevents the arterialization of a<br />
single outflow vein and there<strong>for</strong>e the development<br />
of a functional fistula; thrill and bruit are<br />
present but appropriate vein development is<br />
absent. To detect the presence of an accessory<br />
vein, occlude the main outflow vein with finger<br />
pressure sequentially along the vein. Note the<br />
character of the flow with the occlusion. If there<br />
is no accessory, the flow will become an<br />
augmented pulse. If an accessory vein is present<br />
between the anastomosis and the occlusion<br />
point, the thrill will continue.<br />
4. Medical diagnostics and treatment.<br />
a. Doppler ultrasound or fistulogram/venogram<br />
to measure flow and detect stenosis.<br />
Treatment <strong>for</strong> hemodynamically significant<br />
stenosis is balloon angioplasty.<br />
b. Treatment <strong>for</strong> venous hypertension is arm<br />
elevation above the level of the heart.<br />
c. Treatment <strong>for</strong> accessory veins is surgical<br />
ligation or percutaneous coil ablation (coils<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008 743
<strong>Section</strong> <strong>12</strong>. <strong>Vascular</strong> <strong>Access</strong> <strong>for</strong> <strong>Hemodialysis</strong><br />
are injected into the veins and expand to<br />
block and clot the veins) if no stenosis is<br />
detected in main outflow vein.<br />
d. Infection occurring within 3 weeks of surgery<br />
is generally considered perioperative infection<br />
and is usually prevented by prophylactic<br />
antibiotics at the time of surgery.<br />
5. Late failure.<br />
a. Thrombosis.<br />
(1) Causes. Items (a) through (d) are<br />
applicable <strong>for</strong> AVG also.<br />
(a) Stenosis of main outflow vein<br />
without collateral circulation and/or<br />
(b) Significant hypotension due to<br />
volume depletion.<br />
(c) Hypercoagulable states.<br />
(d) Prolonged occlusive compression of<br />
access vessel vein from a pressure<br />
dressing, tight clothing or jewelry<br />
(anything that leaves an impression is<br />
too tight), supporting heavy objects<br />
such as a basket handle or a sleeping<br />
head. (Lifting heavy objects with the<br />
hands once the suture line is well<br />
healed [> 10 days postoperatively]<br />
will not damage the AVF.)<br />
(2) Signs and symptoms of impending<br />
thrombosis. Items (b) through (h) are<br />
applicable <strong>for</strong> AVG as well.<br />
(a) The vein is distended and does not<br />
soften when the arm is elevated<br />
overhead.<br />
(b) Significantly decreased intra-access<br />
blood flow (400–500 mL/min <strong>for</strong><br />
AVF and < 600 mL/min <strong>for</strong> AVG )<br />
(NKF KDOQI, 2006, CPG 4).<br />
(c) Increased static venous pressures and<br />
standardized dynamic venous<br />
pressures with a ratio:<br />
[1] >0.5 <strong>for</strong> AVG venous segment<br />
and <strong>for</strong> AVG arterial segment<br />
ratio > 0.75.<br />
[2] >0.35 <strong>for</strong> AVF venous segment<br />
and > 0.43 <strong>for</strong> AVF arterial segment<br />
(NKF KDOQI, 2006, CPG 4).<br />
(d) Changes in the quality of the bruit.<br />
(e) Pulsation rather than thrill.<br />
(f) Difficulty cannulating or pain with<br />
cannulation.<br />
(g) Evacuation of clots even with needle<br />
properly inserted into the center of<br />
the vessel.<br />
(h) Increased viscosity of intra-access<br />
flow as evidenced by:<br />
[1] Difficulty maintaining<br />
extracorporeal blood flow at<br />
prescribed rate without increase<br />
in venous pressure and decrease<br />
in arterial pressure.<br />
[2] <strong>Access</strong> recirculation causing<br />
unexplained decrease in Kt/V and<br />
URR – this is a late sign.<br />
[3] Black blood syndrome that occurs<br />
when the same blood is being<br />
recirculated through the dialyzer<br />
and becomes deoxygenated as<br />
well as hemoconcentrated.<br />
Lightening of blood color in the<br />
arterial line when saline is<br />
introduced into the venous line<br />
confirms recirculation. This is a<br />
very late sign and constitutes an<br />
emergency requiring same day<br />
intervention.<br />
(3) Predominant signs of thrombosis in AVF<br />
and AVG are the absence of thrill and<br />
bruit along the access vessel. There may<br />
be a strong pulse in the artery at the<br />
inflow anastomosis. Do not cannulate<br />
vessel to confirm. Needle holes in a<br />
thrombosed access complicate or prevent<br />
lytic administration.<br />
(4) Treatment <strong>for</strong> AVF and AVG.<br />
(a) Urgent referral to an interventionalist<br />
or surgeon to:<br />
[1] Prevent thrombosis by detecting<br />
and treating stenosis or<br />
[2] Per<strong>for</strong>m thrombectomy by lysing<br />
with a thrombolytic such as tPA<br />
(tissue plasminogen activator)<br />
to soften or resolve clot. This is<br />
frequently used be<strong>for</strong>e mechanical<br />
thrombectomy and can be<br />
followed by correction of causative<br />
stenoses if indicated with<br />
angioplasty or surgical revision.<br />
(b) <strong>Access</strong> monitoring and surveillance<br />
postprocedure to assure normal flow<br />
and pressure parameters.<br />
(c) Anticoagulation <strong>for</strong> proven<br />
hypercoagulable states.<br />
(d) Targeted ultrafiltration to patient<br />
tolerance.<br />
(e) Patient and staff education about<br />
prevention of:<br />
[1] Prolonged occlusive pressure.<br />
[2] Hypovolemic hypotension.<br />
744<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008
Chapter 59. <strong>Vascular</strong> <strong>Access</strong> Type and Site of Placement<br />
b. Infection (<strong>for</strong> both AVF and AVG).<br />
(1) Causes.<br />
(a) Poor patient hygiene (Kaplowitz et<br />
al., 1988).<br />
(b) Inadequate skin cleansing <strong>for</strong><br />
cannulation.<br />
(c) Not using aseptic technique <strong>for</strong><br />
cannulation (Schanzer, 2002).<br />
(d) Seeding from another infected site in<br />
the body.<br />
(2) Signs and symptoms.<br />
(a) Inflammation.<br />
(b) Pain.<br />
(c) Skin break with drainage along the<br />
course of the vessel.<br />
(d) Fever.<br />
(3) Intervention and treatment.<br />
(a) Culture of any exudates.<br />
(b) IV broad spectrum or organism<br />
sensitive antibiotics.<br />
(c) Surgical takedown of AVF if evidence<br />
of septic emboli. Surgical resection<br />
and removal of affected portion or all<br />
of graft.<br />
(4) Nursing management note: Cannulation<br />
of an access with an infected segment<br />
should be done only with a physician<br />
order if dialysis is extremely urgent. The<br />
infected area must be avoided.<br />
c. High output cardiac failure (seen in AVF and<br />
progresses with AVF maturation).<br />
(1) Cause. Creation or development of an<br />
AVF that shunts more blood through the<br />
fistula to the detriment of the peripheral<br />
circulation causing tissue hypoxemia and<br />
a compensatory increase in cardiac<br />
output (Guyton & Hall, 2006). This<br />
condition can include the development<br />
of left ventricular hypertrophy, highoutput<br />
cardiac failure, exacerbation of<br />
coronary ischemia, and the possible<br />
contribution to the development of<br />
central vein stenosis (MacRae et al.,<br />
2006) and is aggravated by a preexisting<br />
anemia and/or cardiovascular disease.<br />
(2) Signs and symptoms that occur at or<br />
near dry weight:<br />
(a) Tachycardia.<br />
(b) Shortness of breath.<br />
(c) Pulmonary crackles.<br />
(d) Cyanosis of lips and nail beds.<br />
(e) Pulmonary edema.<br />
(f) Peripheral edema.<br />
(g) Jugular vein distension (if patent).<br />
(h) Confusion.<br />
(3) Potential complications.<br />
(a) Pulmonary edema.<br />
(b) Angina.<br />
(c) Cardiac dysrhythmias.<br />
(4) Diagnosis is by:<br />
(a) Branham’s sign: a decreasing pulse<br />
rate when the vein is compressed.<br />
(b) Echocardiography with and without<br />
AVF compression.<br />
(5) Treatment.<br />
(a) Surgical reduction of flow with a<br />
banding procedure or surgical ligation.<br />
(b) Correct anemia.<br />
(c) Review cardiac pharmacotherapy.<br />
(d) To reduce interdialytic symptoms, the<br />
AVF and outflow vein can be wrapped<br />
with an elastic bandage to reduce<br />
cardiac output. This requires a physician’s<br />
or APN’s order. The nurse or<br />
patient must be able to com<strong>for</strong>tably<br />
slide an index finger under the bandage<br />
to be sure the AVF is not occluded.<br />
II. Arteriovenous grafts (AVG).<br />
A. Definition. A synthetic or, less frequently, biologic<br />
conduit implanted subcutaneously and interposed<br />
between an artery and a vein. Needles are inserted<br />
into the graft (never into the anastomoses) to<br />
remove and return blood during hemodialysis.<br />
The average graft diameter is 6 mm.<br />
B. Types. Synthetic grafts are usually made of<br />
expanded polytetrafluoroethylene (ePTFE/Teflon)<br />
and may be tapered <strong>for</strong> the arterial anastomosis or<br />
contain ringed segments to prevent kinking at the<br />
apex of the loop. Tapering and external rein<strong>for</strong>cement<br />
have not been shown to significantly<br />
improve AVG outcomes (NKF KDOQI, 2006,<br />
CPG 2). The composite/polyurethane graft has a<br />
temporary advantage over ePTFE. Because of its<br />
self-sealing property, it can be cannulated within<br />
hours of placement. Biologic grafts are sometimes<br />
autogenous vein or cryopreserved human vein but<br />
most frequently are from treated bovine vessels.<br />
The latter have been shown to provide functional<br />
access <strong>for</strong> patients who have failed PTFE.<br />
C. Indications. Patients who do not have vasculature<br />
suitable <strong>for</strong> AVF or who have a failed AVF in the<br />
location of the planned AVG.<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008 745
<strong>Section</strong> <strong>12</strong>. <strong>Vascular</strong> <strong>Access</strong> <strong>for</strong> <strong>Hemodialysis</strong><br />
4. Can be placed in many areas of the body<br />
including the upper surface of the thighs and<br />
the anterior chest wall.<br />
5. Can be placed in a variety of shapes to facilitate<br />
cannulation.<br />
6. Are easier <strong>for</strong> the surgeon to handle, implant,<br />
and construct the vascular anastomoses.<br />
7. Are comparatively easier to repair either<br />
surgically or endovascularly (gaining entry<br />
through the vascular system rather than<br />
through an incision).<br />
vein<br />
artery<br />
Figure <strong>12</strong>.3. Forearm loop graft. Actual site<br />
may vary depending on patient.<br />
Used with permission from Arrow International Inc.<br />
D. Anatomic locations, configurations, and<br />
placement priority (NKF KDOQI, 2006 CPG 2)<br />
(see Figure <strong>12</strong>.3).<br />
1. A <strong>for</strong>earm loop graft is preferable to a straight<br />
configuration.<br />
2. Upper arm graft – either an arc (preferred) or a<br />
loop.<br />
3. Chest wall or “necklace” prosthetic graft or<br />
lower-extremity fistula (rare) or graft; (all arm<br />
sites should be exhausted). “Femoral placement<br />
of access has been associated with proximal<br />
venous stenosis, which may be problematic later<br />
in patients receiving kidney transplantation”<br />
(NKF, 2006).<br />
E. Advantages of AVGs.<br />
1. Have a large surface area available <strong>for</strong><br />
cannulation.<br />
2. Are technically easier to cannulate than new AVFs.<br />
3. Lag time from insertion to maturation is short.<br />
For ePTFE grafts, it is recommended that not<br />
less than 14 days should elapse prior to<br />
cannulation to allow healing and incorporation<br />
of the surrounding tissue into the graft. Ideally<br />
3–6 weeks are recommended to allow healing of<br />
incision and resolution of pain and swelling.<br />
F. Disadvantages of AVGs.<br />
1. Are associated with an increased incidence of<br />
thrombosis and infection over an AVF.<br />
2. Patients have a higher mortality risk than<br />
patients dialyzed with fistulae. Those without<br />
diabetes have a relative risk (RR) = 1.47, and<br />
those with diabetes have a RR = 2.47 (Dhingra<br />
et al., 2001).<br />
3. Have shorter patency rates than AVF (a primary<br />
patency in grafts at 18 months of 33%<br />
compared with fistulae at 51% and a secondary<br />
patency rate of 55% as compared with 77% in<br />
fistulae) (Huber et al., 2003).<br />
4. Cannulation sites seal but do not heal.<br />
5. Have the potential <strong>for</strong> an allergic response to<br />
nonautogenous material, especially PTFE.<br />
6. May cause steal syndrome in patients with<br />
compromised peripheral vasculature.<br />
G. Complications of AVGs (NKF KDOQI, 2006,<br />
CPG 6).<br />
1. Extremity edema.<br />
a. Causes. Venous hypertension secondary to<br />
increased cardiac output and exacerbated by<br />
presence of one or more stenotic lesions in<br />
the proximal and central vessels.<br />
b. Treatment. If newly postoperative, arm<br />
should be elevated above the level of the<br />
heart whenever the patient is sitting or lying<br />
down. If swelling persists beyond 2–3 weeks,<br />
imaging to detect pathologic stenosis is<br />
indicated and corrected with angioplasty and<br />
maybe even stenting <strong>for</strong> a long, recoiling<br />
(returns after angioplasty) stenosis.<br />
2. Steal syndrome, usually early post-AVG<br />
placement, is ischemia of the extremity distal to<br />
the arterial anastomosis (may be seen late in<br />
AVF with hypertrophied upper arm with flows<br />
> 1.5 L/min).<br />
a. Caused by diverting significant volume of<br />
blood away from the peripheral circulation.<br />
746<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008
Chapter 59. <strong>Vascular</strong> <strong>Access</strong> Type and Site of Placement<br />
b. Complicated by patients, usually elderly,<br />
with:<br />
(1) Peripheral vascular disease.<br />
(2) Diabetes.<br />
(3) History of multiple access surgeries in<br />
same extremity.<br />
c. Signs and symptoms (that may increase<br />
intradialytically).<br />
(1) Pain distal to anastomosis.<br />
(2) Cold, pale hand.<br />
(3) Impaired hand movement and strength.<br />
(4) Paresthesias: numbness, tingling (pins<br />
and needles) which increases<br />
intradialytically.<br />
(5) Poor capillary refill of affected nail beds<br />
(> 2 secs).<br />
(6) May progress to ulcerated, necrotic<br />
fingertips.<br />
d. Diagnosis, based on physical examination,<br />
can be confirmed with ultrasound to<br />
measure arterial flow to fingertips<br />
(plethysmyography/PPGs).<br />
e. Treatment.<br />
(1) Surgical reperfusion of the hand using<br />
the DRIL (distal revascularizationinterval<br />
ligation) procedure (Diehl et al.,<br />
2003; Knox et al., 2002) while<br />
maintaining flow through AVG.<br />
(2) Banding of inflow to AVF to reduce flow.<br />
(3) Severe ischemia not amenable to surgical<br />
revision may require urgent ligation of<br />
the access.<br />
(4) Symptoms of mild ischemia may be<br />
improved with the wearing of a glove,<br />
keeping the hand dependent as much as<br />
possible, exercise, and massage.<br />
3. Graft degeneration and pseudoaneurysms in<br />
AVG and aneurysms in AVF outflow vein.<br />
a. Causes.<br />
(1) AVG. Repeated cannulation in same area<br />
of graft leading to extravasation (bleeding)<br />
into the incorporating tissue and creating<br />
a pseudoaneurysm. The expansion of the<br />
pseudoaneurysm can cause stretching of<br />
the overlying subcutaneous tissue and<br />
combined with the scar tissue of multiple<br />
cannulations can lead to compromise of<br />
the microcirculation. This causes tissue<br />
breakdown and puts the patient at risk <strong>for</strong><br />
graft rupture.<br />
(2) AVF. Repeated cannulation in same area<br />
of vein leading to weakening and<br />
subsequent ballooning of the vein wall.<br />
What is the difference between an aneurysm and a<br />
pseudoaneurysm?<br />
■ An aneurysm is an abnormal blood-filled dilation of a<br />
blood vessel wall (most commonly in arteries) resulting<br />
from disease or repeated injury of the vessel wall.<br />
■ A pseudoaneurysm is a vascular abnormality that<br />
resembles an aneurysm, but the outpouching is not<br />
limited by a true vessel wall, but rather by external<br />
fibrous tissue.<br />
Adapted from the glossary (NKF, 2006).<br />
b. Signs (2–4 apply to both AVF and AVG).<br />
(1) Sudden appearance of an irregular,<br />
pulsatile mass on the surface of the AVG.<br />
(2) Increase in size of the pseudoaneurysm<br />
or aneurysm from increased pressure<br />
in vessel.<br />
(3) Thinning of the overlying skin over the<br />
vessel giving a shiny appearance.<br />
(4) Poor healing of needle sites.<br />
c. Treatment.<br />
(1) Never cannulate into a pseudoaneurysm<br />
or a large aneurysm. It causes further<br />
vessel degeneration and can be difficult<br />
to locate the center of the underlying<br />
vessel flow.<br />
(2) A rapidly, progressing pseudoaneurysm<br />
or aneurysm is one that is more than<br />
twice the diameter of the vessel and must<br />
be surgically repaired or a covered stent<br />
placed. Those with skin degeneration<br />
should be surgically repaired as they put<br />
the patient at risk <strong>for</strong> infection and access<br />
rupture that is a life-threatening emergency.<br />
Cannulation through a stent is an<br />
off-label use of the device and should<br />
never be done without a physician’s order.<br />
4. Traumatic AVF.<br />
a. Caused by needle passing through the vessel<br />
during cannulation and creating an abnormal<br />
fistula track between the vessel and an underlying<br />
artery. Blood from the artery shunts<br />
into the vessel, thereby disturbing the existing<br />
flow pattern (White, 2006).<br />
b. Signs.<br />
(1) Abnormal presence of a strong pulsation<br />
in area of vessel not previously observed.<br />
May be more pronounced than at the<br />
arterial anastomosis.<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008 747
<strong>Section</strong> <strong>12</strong>. <strong>Vascular</strong> <strong>Access</strong> <strong>for</strong> <strong>Hemodialysis</strong><br />
<strong>Vascular</strong> <strong>Access</strong> Terminology <strong>for</strong> Physical Examination<br />
■ Proximal: that portion of the access used <strong>for</strong> “arterial<br />
needle.” In both a graft and AVF, this is the part of the<br />
access vessel that is closest to the arterial anastomosis.<br />
■ Distal: that portion of the access that is used <strong>for</strong> the<br />
“venous needle” and leads to the draining veins of the<br />
central venous system.<br />
Adapted from the glossary (NKF, 2006).<br />
(2) Sudden increase in venous pressure not<br />
present during previous dialysis session is<br />
possible.<br />
c. Treatment is referral to an interventionalist<br />
<strong>for</strong> evaluation and/or to a surgeon <strong>for</strong><br />
possible repair.<br />
5. Thrombosis, impending and actual.<br />
a. Causes.<br />
(1) Stenosis at the anastomoses, intragraft,<br />
the outflow vein or the central veins.<br />
Though the venous anastomosis is the<br />
most common site of stenosis, inflow<br />
stenosis at the arterial anastomosis can be<br />
as high as 20 to 25%. Stenosis is the cause<br />
of 90% of thrombosed grafts (NKF<br />
KDOQI, 2006, CPG 6).<br />
(2) In the absence of stenosis, causes as <strong>for</strong> AVF.<br />
b. Signs of impending thrombosis (same as <strong>for</strong><br />
AVF), plus:<br />
(1) Increasing static pressures proximal to<br />
the stenosis; can lead to extended time to<br />
hemostasis postdialysis and appearance<br />
of new pseudoaneurysms.<br />
(2) Decreasing flow through the graft to<br />
< than 600 mL/min.<br />
(3) Abnormal coagulation studies indicating<br />
a hypercoagulable state (LeSar et al.,<br />
1999; O’Shea et al., 2003).<br />
c. Treatment <strong>for</strong> preventing impending<br />
thrombosis.<br />
(1) Angiography with selective angioplasty of<br />
those stenoses that cause > 50% decrease<br />
in vessel lumen diameter and reduction<br />
in access flow with increased intra-access<br />
pressure.<br />
(2) Anticoagulation or antiplatelet therapy<br />
<strong>for</strong> hypercoagulable state.<br />
(3) Signs and treatment of thrombosis is as<br />
<strong>for</strong> AVF.<br />
6. Infection (see complications of AVF).<br />
III. Central venous catheters (CVC)/port<br />
catheter systems.<br />
Catheters and ports are essential tools <strong>for</strong> providing<br />
urgent and, in some cases, long-term vascular access.<br />
Prevention and early treatment of complications<br />
should greatly reduce associated morbidity and<br />
mortality (NKF KDOQI, 2006, CPG 7).<br />
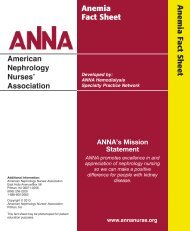
A. Definition. A synthetic, relatively large (10–22 Fr.<br />
outer diameter in adults) tube placed into a highflowing<br />
central vein. Because hemodialysis<br />
removes and returns blood at the same time, the<br />
catheter either has two side-by-side chambers or<br />
lumens (called a dual lumen catheter) or two<br />
single lumen catheters (called twin catheters). The<br />
end of the catheter that enters the patient’s<br />
bloodstream is the “tip” and has holes <strong>for</strong> blood<br />
entry or exit. The other end, the “tail,” is outside<br />
the body with the two lumens separated (see<br />
Figure <strong>12</strong>.4). Each lumen has a threaded hub on<br />
the tail <strong>for</strong> attaching to the bloodlines. The exit<br />
site is where the catheter comes out through the<br />
skin. The port catheter system has one or two<br />
metal ports under the skin that are attached to<br />
single lumen catheters. These are accessed each<br />
treatment by cannulas.<br />
Tunnel tract<br />
Portion of the catheter that<br />
is tunneled<br />
under the skin<br />
Cuff<br />
Small fibrous band<br />
that holds the<br />
catheter in place<br />
under the skin<br />
Exit site<br />
Where the catheter exits<br />
the body<br />
Tips<br />
Placed in right<br />
atrium of the heart<br />
Figure <strong>12</strong>.4. Central venous catheter.<br />
Used with permission from Arrow International Inc.<br />
748<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008
Chapter 59. <strong>Vascular</strong> <strong>Access</strong> Type and Site of Placement<br />
B. Types. Catheters need to be made of rigid, semirigid<br />
material, or be structurally rein<strong>for</strong>ced to<br />
prevent collapse of the lumen. Catheter lengths<br />
vary with the size of the patient and the site of<br />
placement.<br />
1. Nontunneled, noncuffed acute catheters <strong>for</strong><br />
short-term use (see Figure <strong>12</strong>.5). These should<br />
stay in no longer than a week, and the patient<br />
should not be discharged from hospital with<br />
this type of catheter. The tips should be in the<br />
superior vena cava (NKF KDOQI, 2006, CPG 2.)<br />
2. Tunneled, cuffed catheters (see Figure <strong>12</strong>.6) and<br />
port catheter systems are <strong>for</strong> long-term use only<br />
in the patient who:<br />
a. Is not suitable <strong>for</strong> an AVF or AVG access.<br />
b. Has an AVF or AVG planned.<br />
c. Has an AVF or AVG waiting to mature.<br />
d. Is waiting <strong>for</strong> a scheduled live donor<br />
transplant.<br />
3. The tips of the catheter should be in the right<br />
mid-atrium with the arterial port medial (<strong>for</strong><br />
neck and chest placements) (NKF KDOQI,<br />
2006, CPG 2) (see Figure <strong>12</strong>.4). The fibrous<br />
cuff, positioned about 1 cm from exit site inside<br />
the tunnel, is designed to incorporate the<br />
tunnel tissue thereby creating a barrier to<br />
organism entry as well preventing catheter<br />
dislodgment. In chest and neck placements, the<br />
exit site is usually a few centimeters below the<br />
clavicle. To determine whether the catheter is<br />
inserted into the internal jugular (IJ) or the<br />
subclavian vein, see Table <strong>12</strong>.2.<br />
C. Anatomic locations. Catheters or port/catheter<br />
devices should not be placed on the same side as a<br />
slowly maturing long-term access (NKF KDOQI,<br />
2006, CPG 2). Catheters are always inserted into<br />
veins.<br />
1. Right internal (or external) jugular vein is the<br />
preferred site because this site offers a more<br />
direct route to the right atrium than the leftsided<br />
great veins (see Figure <strong>12</strong>.4). Catheter<br />
insertion and maintenance in the right internal<br />
jugular vein are associated with a lower risk of<br />
complications compared to other potential<br />
catheter insertion sites.<br />
Figure <strong>12</strong>.5. Nontunneled, noncuffed acute catheters <strong>for</strong><br />
short-term use.<br />
Used with permission from Arrow International Inc.<br />
Table <strong>12</strong>.2<br />
How to Differentiate Between an IJ<br />
and a Subclavian Catheter Placement<br />
Inspection<br />
pediatric<br />
adult<br />
split<br />
lumens<br />
twin,<br />
single<br />
lumen<br />
■ Where is the exit site — above or below the clavicle?<br />
■ Can you see the outline of the catheter in a tunnel?<br />
■ Can you see the tunneled catheter crossing the<br />
clavicle?<br />
Figure <strong>12</strong>.6. Cuffed catheters. The pencil is shown as a<br />
size comparison.<br />
Palpation<br />
■ With a gloved hand, feel the skin above the exit site.<br />
Can you feel the catheter in a tunnel?<br />
■ Trace the tunnel till you can no longer feel the<br />
catheter. If it crosses the clavicle, it’s jugular. If not, it’s<br />
probably subclavian.<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008 749
<strong>Section</strong> <strong>12</strong>. <strong>Vascular</strong> <strong>Access</strong> <strong>for</strong> <strong>Hemodialysis</strong><br />
2. Left internal jugular vein catheter placement<br />
potentially puts the left arm’s vasculature in<br />
jeopardy <strong>for</strong> a long-term access on the same<br />
side. It may also be associated with poorer<br />
blood flow rates and higher rates of stenosis<br />
and thrombosis than the RIJ due to the<br />
increased length.<br />
3. Femoral placement is associated with the<br />
highest infection rates and the catheter tip must<br />
be in the inferior vena cava to avoid regional<br />
recirculation (see Figure <strong>12</strong>.7). Placement of a<br />
femoral catheter in a transplant candidate<br />
should be avoided because of potential damage<br />
to blood vessels needed <strong>for</strong> the transplant.<br />
4. Subclavian veins on either side must be strictly<br />
avoided due to risk of stenosis, which can<br />
permanently exclude the possibility of upper<br />
extremity long-term AVF or AVG (NKF<br />
KDOQI, 2006, CPG 2). They should be used<br />
only when all access sites are exhausted in the<br />
ipsilateral (same side) arm. Subclavian<br />
placement puts patient at greater risk <strong>for</strong><br />
pneumothorax and/or hemothorax during<br />
insertion.<br />
5. When all the above sites are exhausted, catheters<br />
may be inserted into the inferior vena cava using<br />
the translumbar or transhepatic approach.<br />
D. Advantages of catheters/ports.<br />
1. Are universally applicable – anyone can have one.<br />
2. Can be inserted into multiple sites relatively<br />
easily.<br />
3. Require no maturation time. They can be used<br />
immediately (after tip position is confirmed by<br />
fluoroscopy or chest x-ray).<br />
4. Cause no changes in cardiac output or<br />
myocardial load.<br />
5. Can provide access over a period of months,<br />
permitting AVF maturation in patients who<br />
require immediate hemodialysis.<br />
6. Percutaneous catheters only.<br />
a. Skin puncture not required <strong>for</strong> repeated<br />
vascular access <strong>for</strong> hemodialysis.<br />
b. Lower initial cost and replacement costs.<br />
Exit site<br />
Venous<br />
Arterial<br />
E. Disadvantages.<br />
1. High morbidity due to thrombosis and infection<br />
(Oliver et al., 2004; Pastan et al., 2003). Patients<br />
receiving catheters have a relative risk (RR) of<br />
death (RR = 2.3 <strong>for</strong> patients with diabetes and<br />
1.83 <strong>for</strong> those without) greater than those with<br />
an AVF (Dhingra et al., 2001).<br />
2. Risk of permanent central venous stenosis or<br />
occlusion.<br />
3. Percutaneous catheters only.<br />
a. Discom<strong>for</strong>t and cosmetic disadvantage of an<br />
external appliance.<br />
b. Safety concern with inadvertent dislodgment<br />
of external appliance as well as need <strong>for</strong><br />
protection of exit site.<br />
c. Shorter expected use-life than other access<br />
types.<br />
d. Overall lower blood flow rates, requiring<br />
longer dialysis times.<br />
4. Frequent episodes of occluded catheters due to<br />
thrombosis or fibrin sheaths may require use of<br />
a lytic agent or an interventional procedure to<br />
replace the catheter and possibly disrupt a<br />
sheath. These episodes may lead to reduced<br />
dialysis adequacy (lower BFRs and shortened or<br />
missed treatments) that is associated with<br />
increased morbidity and mortality.<br />
Figure <strong>12</strong>.7. Femoral vein central venous catheter.<br />
750<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008
Chapter 59. <strong>Vascular</strong> <strong>Access</strong> Type and Site of Placement<br />
F. Complications.<br />
1. Immediate/early.<br />
a. All catheters should be placed using imaging<br />
such fluoroscopy or ultrasound (NKF<br />
KDOQI, 2006, CPG 2) to assure correct<br />
tip placement and minimize complications<br />
such as:<br />
(1) Carotid or femoral artery puncture.<br />
(2) Pneumothorax.<br />
(3) Hemothorax.<br />
(4) Cardiac dysrhythmias.<br />
(5) Tissue per<strong>for</strong>ation (e.g., brachial plexus,<br />
trachea, superior vena cava, myocardium).<br />
(6) Poor flow from malpositioned tip.<br />
b. Operating room conditions and practice<br />
must be used <strong>for</strong> placement to prevent<br />
infection.<br />
2. Late complications.<br />
a. Infection. Local and systemic.<br />
(1) Causes.<br />
(a) Not using aseptic technique and<br />
appropriate cleansing <strong>for</strong> accessing<br />
catheter.<br />
(b) Poor patient hygiene.<br />
(c) Inadequate skin cleansing at dressing<br />
change.<br />
(2) Signs and symptoms.<br />
(a) Inflammation and pain around exit<br />
site and in tunnel.<br />
(b) Drainage at exit site or from tunnel.<br />
(c) Erosion of skin over catheter.<br />
(d) Fever and/or chills.<br />
(3) Treatment (NKF KDOQI, 2006, CPG 7).<br />
(a) IV broad spectrum or organism<br />
sensitive antibiotics <strong>for</strong> all infections<br />
except localized exit site where topical<br />
and/or oral antibiotics may be used.<br />
(b) Catheter exchange within 72 hours of<br />
initiating antibiotic therapy with<br />
follow-up cultures 1 week after<br />
antibiotic therapy.<br />
(c) Antibiotic lock therapy may be used<br />
instead of catheter exchange in cases<br />
where the patient is clinically stable<br />
and/or the catheter is reinfected with<br />
the same organism and catheter sites<br />
are limited (NKF KDOQI, 2006,<br />
CPR 7) (see <strong>Section</strong> 5, Table 5.6, <strong>for</strong><br />
sample protocol).<br />
(d) Port pocket infections are treated<br />
with systemic antibiotics and pocket<br />
irrigation.<br />
b. Catheter dysfunction (BFR < 300 mL/min).<br />
Exceptions are <strong>for</strong> pediatric patients and<br />
small adults. Dysfunction <strong>for</strong> these categories<br />
is defined by a significant reduction in<br />
baseline flows.<br />
(1) Causes.<br />
(a) Mechanical. Line and catheter<br />
kinking, holes or cracks in catheter,<br />
drug precipitation.<br />
(b) Patient position.<br />
(c) Partial or complete occlusion due to<br />
intraluminal or mural thrombus or<br />
fibrin sheath.<br />
(2) Signs.<br />
(a) Inability to withdraw anticoagulant<br />
lock or blood.<br />
(b) Inability to maintain consistent<br />
BFR > 300 mL/min at an arterial<br />
< -250 mm/Hg. Arterial prepump<br />
pressure monitoring is mandatory.<br />
(c) Presence of leak from catheter.<br />
(3) Treatment. See algorithm in Nursing<br />
Process interventions (see Figure <strong>12</strong>.8).<br />
c. Superior vena cava syndrome. Catheter<br />
insertion and long-term placement can cause<br />
endothelial injury, inflammation, stenosis,<br />
and occlusion of any vein. When this occurs<br />
in the superior vena cava, it has lifethreatening<br />
implications and constitutes an<br />
emergency to be reported to the physician. It<br />
can have slow or rapid onset.<br />
(1) Signs and symptoms.<br />
(a) Swelling of the chest/breast, arms,<br />
neck, and face with periorbital edema.<br />
(b) Visible collateral veins on chest wall<br />
and jugular vein distension (if patent).<br />
(c) CNS disturbances such as vision<br />
changes, dizziness, confusion, pain.<br />
(d) Dyspnea (difficulty breathing) and/or<br />
dysphagia (difficulty swallowing).<br />
(2) Treatment.<br />
(a) Removal of any obstruction<br />
including an indwelling catheter.<br />
(b) Lysing of thrombus with a<br />
thrombolytic infusion.<br />
(c) Angioplasty of identified stenoses.<br />
Stents could be placed <strong>for</strong> recoiling<br />
stenoses.<br />
(Figure <strong>12</strong>.8 on next page)<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008 751
<strong>Section</strong> <strong>12</strong>. <strong>Vascular</strong> <strong>Access</strong> <strong>for</strong> <strong>Hemodialysis</strong><br />
Nursing Assessment: Decision to Use a Thrombolytic<br />
Sluggish flow or inability to withdraw blood or<br />
infuse fluid through the catheter<br />
Check <strong>for</strong> mechanical<br />
obstruction<br />
Occlusion<br />
remains<br />
Suspect<br />
thrombus<br />
Thrombolytic therapy?<br />
Obstruction<br />
corrected<br />
Flow restored<br />
• BFR < 300 mL/min<br />
• URR < 65%<br />
• Kt/V < 1.2<br />
• AP > -250 mm Hg<br />
• VP > 200 mm Hg<br />
• Kink in line<br />
• Catheter migration<br />
• Patient position<br />
• Catheter integrity<br />
• BFR < 300 mL/min<br />
• URR < 65%<br />
• Kt/V < 1.2<br />
• AP > -250 mm Hg<br />
• VP > 200 mm Hg<br />
YES!<br />
Figure <strong>12</strong>.8. Algorithm <strong>for</strong> catheter dysfunction.<br />
Source: Dinwiddie, L.C. (2004). Managing catheter dysfunction <strong>for</strong> better patient outcomes:<br />
A team approach. Nephrology Nursing Journal, 31(6), 653-660.<br />
Needle phobia<br />
Needle phobia has been defined<br />
as a <strong>for</strong>mal medical condition and<br />
is included in the <strong>American</strong> Psychiatric<br />
Association’s Diagnostic<br />
and Statistical Manual of Mental<br />
Disorders, 4th edition (DSM-IV)<br />
within the diagnostic category of<br />
Blood-Injection-Injury. Needle<br />
phobia is evidenced by a vasovagal<br />
reflex (frequently inherited) that<br />
causes shock with needle puncture.<br />
With repeated needle exposure,<br />
those with vasovagal shock<br />
reflex tend to develop a fear of<br />
needles. According to the DSM-IV,<br />
a phobia is defined by the<br />
presence of fear and by avoidance<br />
behavior. While a dislike or mild<br />
fear of needles is very common,<br />
needle phobia can be more<br />
rigorously defined by objective<br />
clinical findings in addition to<br />
subjective symptoms.<br />
Source: Hamilton, J.G. (1995). Needle<br />
phobia: A neglected diagnosis. Journal<br />
of Family Practice, 41(5), 437, 5<strong>12</strong>.<br />
Chapter 60<br />
Nursing Process in the Routine Care<br />
of <strong>Vascular</strong> <strong>Access</strong><br />
I. Assessment of all accesses, mature or maturing.<br />
A. Assess patient’s subjective response to the vascular<br />
access, e.g. function, body image, self-concept,<br />
fears, need <strong>for</strong> local anesthesia. Many patients who<br />
suffer from needlephobia will require some <strong>for</strong>m<br />
of local anesthetic. A cream containing lidocaine<br />
2.5%/prilocaine 2.5% is the best choice. The<br />
patient self-administers the cream prior to coming<br />
to dialysis. He/she will need to be instructed on<br />
needle sites at the previous treatment time. This<br />
cream is expensive and can have systemic effects if<br />
too much is absorbed (AstraZeneca, 2005).<br />
There<strong>for</strong>e it should not be applied all over the<br />
vessel. If the patient does not have cream, lidocaine<br />
injection or ethyl chloride spray can be used.<br />
Lidocaine injections put the cannulator at twice<br />
the risk of needle accident and are thought to<br />
facilitate scarring as is ethyl chloride. Patients<br />
should be assessed frequently to determine if the<br />
local anesthetic can be discontinued.<br />
B. Solicit access complaints from patient and<br />
evaluate prior to initiation of treatment.<br />
752<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008