Section 12 Vascular Access for Hemodialysis - American ...
Section 12 Vascular Access for Hemodialysis - American ...
Section 12 Vascular Access for Hemodialysis - American ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Section</strong> <strong>12</strong>. <strong>Vascular</strong> <strong>Access</strong> <strong>for</strong> <strong>Hemodialysis</strong><br />
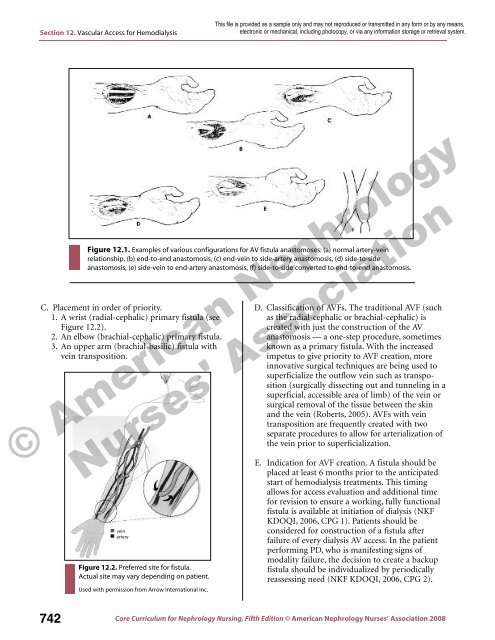
Figure <strong>12</strong>.1. Examples of various configurations <strong>for</strong> AV fistula anastomoses: (a) normal artery-vein<br />
relationship, (b) end-to-end anastomosis, (c) end-vein to side-artery anastomosis, (d) side-to-side<br />
anastomosis, (e) side-vein to end-artery anastomosis, (f) side-to-side converted to end-to-end anastomosis.<br />
C. Placement in order of priority.<br />
1. A wrist (radial-cephalic) primary fistula (see<br />
Figure <strong>12</strong>.2).<br />
2. An elbow (brachial-cephalic) primary fistula.<br />
3. An upper arm (brachial-basilic) fistula with<br />
vein transposition.<br />
vein<br />
artery<br />
Figure <strong>12</strong>.2. Preferred site <strong>for</strong> fistula.<br />
Actual site may vary depending on patient.<br />
Used with permission from Arrow International Inc.<br />
D. Classification of AVFs. The traditional AVF (such<br />
as the radial-cephalic or brachial-cephalic) is<br />
created with just the construction of the AV<br />
anastomosis — a one-step procedure, sometimes<br />
known as a primary fistula. With the increased<br />
impetus to give priority to AVF creation, more<br />
innovative surgical techniques are being used to<br />
superficialize the outflow vein such as transposition<br />
(surgically dissecting out and tunneling in a<br />
superficial, accessible area of limb) of the vein or<br />
surgical removal of the tissue between the skin<br />
and the vein (Roberts, 2005). AVFs with vein<br />
transposition are frequently created with two<br />
separate procedures to allow <strong>for</strong> arterialization of<br />
the vein prior to superficialization.<br />
E. Indication <strong>for</strong> AVF creation. A fistula should be<br />
placed at least 6 months prior to the anticipated<br />
start of hemodialysis treatments. This timing<br />
allows <strong>for</strong> access evaluation and additional time<br />
<strong>for</strong> revision to ensure a working, fully functional<br />
fistula is available at initiation of dialysis (NKF<br />
KDOQI, 2006, CPG 1). Patients should be<br />
considered <strong>for</strong> construction of a fistula after<br />
failure of every dialysis AV access. In the patient<br />
per<strong>for</strong>ming PD, who is manifesting signs of<br />
modality failure, the decision to create a backup<br />
fistula should be individualized by periodically<br />
reassessing need (NKF KDOQI, 2006, CPG 2).<br />
742<br />
Core Curriculum <strong>for</strong> Nephrology Nursing, Fifth Edition © <strong>American</strong> Nephrology Nurses’ Association 2008