Audit Tool
Audit Tool
Audit Tool

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Review Date:<br />
Provider:<br />
Location :<br />
Reviewer:<br />
Patient Name:<br />
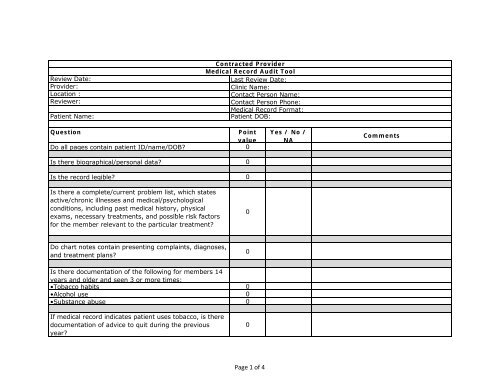
Contracted Provider<br />
Medical Record <strong>Audit</strong> <strong>Tool</strong><br />
Last Review Date:<br />
Clinic Name:<br />
Contact Person Name:<br />
Contact Person Phone:<br />
Medical Record Format:<br />
Patient DOB:<br />
Question<br />
Point<br />
value<br />
Do all pages contain patient ID/name/DOB? 0<br />
Is there biographical/personal data? 0<br />
Is the record legible? 0<br />
Yes / No /<br />
NA<br />
Comments<br />
Is there a complete/current problem list, which states<br />
active/chronic illnesses and medical/psychological<br />
conditions, including past medical history, physical<br />
exams, necessary treatments, t t and possible risk factors<br />
for the member relevant to the particular treatment?<br />
0<br />
Do chart notes contain presenting complaints, diagnoses,<br />
and treatment plans?<br />
0<br />
Is there documentation of the following for members 14<br />
years and older and seen 3 or more times:<br />
•Tobacco habits 0<br />
•Alcohol use 0<br />
•Substance abuse 0<br />
If medical record indicates patient uses tobacco, is there<br />
documentation of advice to quit during the previous<br />
year?<br />
0<br />
Page 1 of 4
Review Date:<br />
Provider:<br />
Location :<br />
Reviewer:<br />
Patient Name:<br />
Contracted Provider<br />
Medical Record <strong>Audit</strong> <strong>Tool</strong><br />
Last Review Date:<br />
Clinic Name:<br />
Contact Person Name:<br />
Contact Person Phone:<br />
Medical Record Format:<br />
Patient DOB:<br />
Question<br />
Point<br />
value<br />
Yes / No /<br />
NA<br />
Comments<br />
Does chart contain past medical history, physical<br />
examinations, necessary treatments, and possible risk<br />
factors for the member relevant to the particular<br />
treatment?<br />
0<br />
Is there evidence that HIPAA privacy requirements are<br />
met and that privacy information is provided to patients<br />
and documented in the chart?<br />
0<br />
If the clinic has electronic medical records, do they have<br />
screen savers with password protection to prevent<br />
confidential information from being viewed by<br />
unauthorized people?<br />
0<br />
Are documents in the medical record securely attached<br />
in the chart?<br />
0<br />
Is there identification of all providers participating in the<br />
member's care and information on services furnished by<br />
these providers?<br />
0<br />
Do all chart notes generated by the provider under<br />
medical record review include the date of service, a<br />
legible signature, the provider's credentials, and<br />
authentication by the provider (for any documents<br />
generated by but not transcribed by the provider under<br />
review)?<br />
0<br />
Is there documentation of preventive care? 0<br />
Page 2 of 4
Review Date:<br />
Provider:<br />
Location :<br />
Reviewer:<br />
Patient Name:<br />
Contracted Provider<br />
Medical Record <strong>Audit</strong> <strong>Tool</strong><br />
Last Review Date:<br />
Clinic Name:<br />
Contact Person Name:<br />
Contact Person Phone:<br />
Medical Record Format:<br />
Patient DOB:<br />
Question<br />
Point<br />
value<br />
Is there documentation of education of self-care? 0<br />
Yes / No /<br />
NA<br />
Comments<br />
Page 3 of 4
Review Date:<br />
Provider:<br />
Location :<br />
Reviewer:<br />
Patient Name:<br />
Contracted Provider<br />
Medical Record <strong>Audit</strong> <strong>Tool</strong><br />
Last Review Date:<br />
Clinic Name:<br />
Contact Person Name:<br />
Contact Person Phone:<br />
Medical Record Format:<br />
Patient DOB:<br />
Question<br />
Point<br />
value<br />
Is there a current medication profile? 0<br />
Yes / No /<br />
NA<br />
Comments<br />
Is there a current allergy and adverse reaction profile?<br />
0<br />
Is it clear and prominently indicated that an inquiry has<br />
been made regarding a patient's advanced directive? 0<br />
Are age-appropriate immunization records<br />
present/current?<br />
0<br />
Is there documentation of follow up care? 0<br />
General Comments:<br />
0 0<br />
Scoring:<br />
To achieve a passing score, the following threshold must be met: ≥80%<br />
Elements 0 #DIV/0! #DIV/0!<br />
Page 4 of 4