Medical Screening Questionnaire - Tina L Baum, Physical Therapist
Medical Screening Questionnaire - Tina L Baum, Physical Therapist
Medical Screening Questionnaire - Tina L Baum, Physical Therapist

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
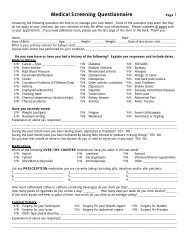
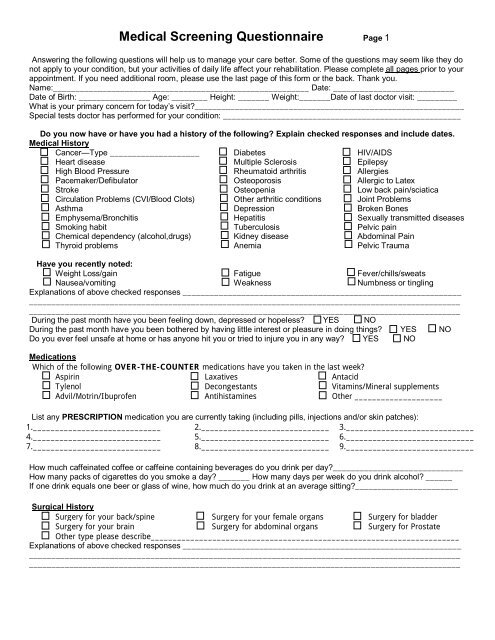
<strong>Medical</strong> <strong>Screening</strong> <strong>Questionnaire</strong> Page 1<br />
Answering the following questions will help us to manage your care better. Some of the questions may seem like they do<br />
not apply to your condition, but your activities of daily life affect your rehabilitation. Please complete all pages prior to your<br />
appointment. If you need additional room, please use the last page of this form or the back. Thank you.<br />
Name:_________________________________________________________ Date: ___________________________<br />
Date of Birth: ________________ Age: ________ Height: _______ Weight:_______Date of last doctor visit: _________<br />
What is your primary concern for today’s visit?____________________________________________________________<br />
Special tests doctor has performed for your condition: _____________________________________________________<br />
Do you now have or have you had a history of the following? Explain checked responses and include dates.<br />
<strong>Medical</strong> History<br />
Cancer—Type ____________________ Diabetes HIV/AIDS<br />
Heart disease Multiple Sclerosis Epilepsy<br />
High Blood Pressure Rheumatoid arthritis Allergies<br />
Pacemaker/Defibulator Osteoporosis Allergic to Latex<br />
Stroke Osteopenia Low back pain/sciatica<br />
Circulation Problems (CVI/Blood Clots) Other arthritic conditions Joint Problems<br />
Asthma Depression Broken Bones<br />
Emphysema/Bronchitis Hepatitis Sexually transmitted diseases<br />
Smoking habit Tuberculosis Pelvic pain<br />
Chemical dependency (alcohol,drugs) Kidney disease Abdominal Pain<br />
Thyroid problems Anemia Pelvic Trauma<br />
Have you recently noted:<br />
Weight Loss/gain Fatigue Fever/chills/sweats<br />
Nausea/vomiting Weakness Numbness or tingling<br />
Explanations of above checked responses ______________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
During the past month have you been feeling down, depressed or hopeless? YES NO<br />
During the past month have you been bothered by having little interest or pleasure in doing things? YES NO<br />
Do you ever feel unsafe at home or has anyone hit you or tried to injure you in any way? YES NO<br />
Medications<br />
Which of the following OVER-THE-COUNTER medications have you taken in the last week?<br />
Aspirin Laxatives Antacid<br />
Tylenol Decongestants Vitamins/Mineral supplements<br />
Advil/Motrin/Ibuprofen Antihistamines Other ____________________<br />
List any PRESCRIPTION medication you are currently taking (including pills, injections and/or skin patches):<br />
1._____________________________ 2._____________________________ 3._____________________________<br />
4._____________________________ 5._____________________________ 6._____________________________<br />
7._____________________________ 8._____________________________ 9._____________________________<br />
How much caffeinated coffee or caffeine containing beverages do you drink per day?_____________________________<br />
How many packs of cigarettes do you smoke a day? _______ How many days per week do you drink alcohol? ______<br />
If one drink equals one beer or glass of wine, how much do you drink at an average sitting?_______________________<br />
Surgical History<br />
Surgery for your back/spine Surgery for your female organs Surgery for bladder<br />
Surgery for your brain Surgery for abdominal organs Surgery for Prostate<br />
Other type please describe______________________________________________________________________<br />
Explanations of above checked responses ______________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________
<strong>Medical</strong> <strong>Screening</strong> <strong>Questionnaire</strong> Page 2<br />
Name: _________________________________<br />
Urologic History<br />
Trouble initiating urine stream Frequent urination Blood in urine<br />
Trouble emptying bladder Pain with urination Bladder Infections<br />
Excessive Urges to empty bladder Incontinence Vaginal dryness<br />
Trouble feeling bladder fullness Childhood bladder problem Bladder cancer<br />
Constant dribbling of urine<br />
Bed wetting<br />
Explanations of above checked responses ______________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
Sexual History<br />
Sexually active<br />
Does your sexual activity cause you pain?<br />
Explanations of above checked responses ______________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
Bowel History<br />
Irritable bowel syndrome GI problems Constipation<br />
Hemorrhoids Difficulty eliminating Trouble holding back gas<br />
Fecal incontinence/leaking<br />
Rectal Pain<br />
OB/Gyn History (Female only)<br />
Painful periods Prolapse or falling out feeling Are You Pregnant? ______ weeks<br />
Date last period _____________ Painful penetration Vaginal deliveries #_____<br />
Endometriosis Upon entry Episiotomy #______<br />
Cysts Deep C-Section #______<br />
Menopause Positional Difficult childbirth<br />
Explanations of above checked responses ______________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
Relevant History (Male Only)\<br />
Prostatitis Scrotum Pain Surgery<br />
Penile Pain Rectal Pain Pain with ejaculation<br />
Explanations of above checked responses ______________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
Please list any other concerns or comments you have:<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
Reviewed by therapist: <strong>Tina</strong> __________ ________________________________ _______________<br />
<strong>Therapist</strong> Signature<br />
Date