Occupational Health Medical History Form
Occupational Health Medical History Form
Occupational Health Medical History Form

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
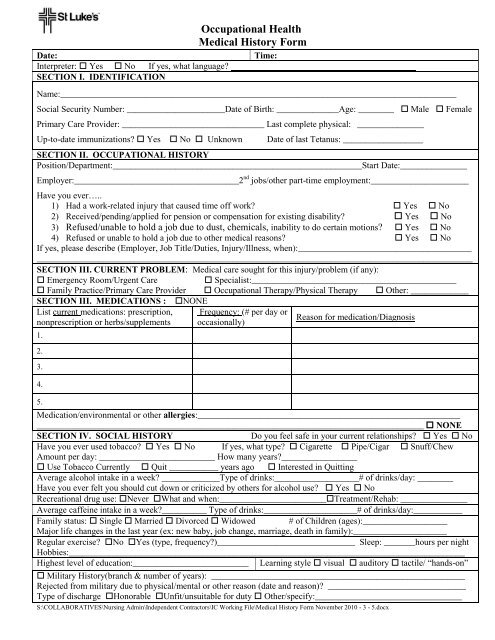
Date:<br />
Interpreter: Yes No If yes, what language?<br />
SECTION I. IDENTIFICATION<br />
<strong>Occupational</strong> <strong>Health</strong><br />
<strong>Medical</strong> <strong>History</strong> <strong>Form</strong><br />
Time:<br />
Name:_________________________________________________________________________________________<br />
Social Security Number: ______________________Date of Birth: ______________Age: ________ Male Female<br />
Primary Care Provider: ________________________________ Last complete physical: _______________<br />
Up-to-date immunizations? Yes No Unknown<br />
Date of last Tetanus: __________________<br />
SECTION II. OCCUPATIONAL HISTORY<br />
Position/Department:________________________________________________________Start Date:_______________<br />
Employer:_____________________________________2 nd jobs/other part-time employment:______________________<br />
Have you ever…..<br />
1) Had a work-related injury that caused time off work? Yes No<br />
2) Received/pending/applied for pension or compensation for existing disability? Yes No<br />
3) Refused/unable to hold a job due to dust, chemicals, inability to do certain motions? Yes No<br />
4) Refused or unable to hold a job due to other medical reasons? Yes No<br />
If yes, please describe (Employer, Job Title/Duties, Injury/Illness, when):_______________________________________<br />
__________________________________________________________________________________________________<br />
SECTION III. CURRENT PROBLEM: <strong>Medical</strong> care sought for this injury/problem (if any):<br />
Emergency Room/Urgent Care<br />
Specialist:______________________________________________<br />
Family Practice/Primary Care Provider <strong>Occupational</strong> Therapy/Physical Therapy Other: _____________<br />
SECTION III. MEDICATIONS : NONE<br />
List current medications: prescription,<br />
nonprescription or herbs/supplements<br />
1.<br />
2.<br />
3.<br />
4.<br />
5.<br />
Frequency: (# per day or<br />
occasionally)<br />
Reason for medication/Diagnosis<br />
Medication/environmental or other allergies:___________________________________________________________<br />
_______________________________________________________________________________________ NONE<br />
SECTION IV. SOCIAL HISTORY<br />
Do you feel safe in your current relationships? Yes No<br />
Have you ever used tobacco? Yes No If yes, what type? Cigarette Pipe/Cigar Snuff/Chew<br />
Amount per day: __________________________ How many years?_________________<br />
Use Tobacco Currently Quit ___________ years ago Interested in Quitting<br />
Average alcohol intake in a week? _____________Type of drinks:___________________# of drinks/day: ________<br />
Have you ever felt you should cut down or criticized by others for alcohol use? Yes No<br />
Recreational drug use: Never What and when:________________________Treatment/Rehab: _______________<br />
Average caffeine intake in a week?__________ Type of drinks:_____________________# of drinks/day:___________<br />
Family status: Single Married Divorced Widowed # of Children (ages):___________________<br />
Major life changes in the last year (ex: new baby, job change, marriage, death in family):_____________________<br />
Regular exercise? No Yes (type, frequency?)_______________________________ Sleep: _______hours per night<br />
Hobbies:_________________________________________________________________________________________<br />
Highest level of education:__________________________ Learning style visual auditory tactile/ “hands-on”<br />
Military <strong>History</strong>(branch & number of years): _________________________________________________________<br />
Rejected from military due to physical/mental or other reason (date and reason)? _______________________________<br />
Type of discharge Honorable Unfit/unsuitable for duty Other/specify:_________________________________<br />
S:\COLLABORATIVES\Nursing Admin\Independent Contractors\IC Working File\<strong>Medical</strong> <strong>History</strong> <strong>Form</strong> November 2010 - 3 - 5.docx
SECTION V. FAMILY HISTORY:<br />
Please indicate current status of immediate family (parent, sibling, child)<br />
Alcohol/Drug abuse:___________ Depression/Suicide:____________ Asthma/COPD:_______________<br />
Cancer(type):_________________ Genetic disorders:_____________ Diabetes:____________________<br />
Heart disease:_________________ High blood pressure:___________ Stroke:_____________________<br />
Bleeding disorder/clots:_________ <strong>Health</strong>y:_____________________ Other:______________________<br />
SECTION VI. MEDICAL HISTORY<br />
Handedness: Right Left<br />
Have you been diagnosed with any of the following conditions?<br />
Alcohol/substance abuse Seizures Arthritis, Rheumatism or Bursitis Thyroid Problem<br />
Cancer Liver disease Bone or Joint problems Back pain/injury<br />
Diabetes Lung Disease Heart problems/High blood pressure Prostate Problems<br />
Major Accident Kidney Disease Stomach/Intestine problems Migraines<br />
Claustrophobia Asbestos/toxic chemical exposure Depression/Anxiety/Mental <strong>Health</strong> Conditions<br />
Type and when: ____________________________________________________________________________________<br />
Please list all other medical conditions: _________________________________________________________________<br />
---------------------------------------------------------------------------------------------------------------------------------------------------<br />
(Provider comments:________________________________________________________________________________)<br />
SECTION VII. HOSPITALIZATION/SURGERIES (Advised to have/had a procedure or surgery? Yes No )<br />
Year Reason Year Reason<br />
SECTION VIII. REVIEW OF SYSTEMS (Which of the following are problems at this time?)<br />
General/Constitutional<br />
Heart/Lungs<br />
Ears/Nose/Throat<br />
Fever >100<br />
Chest Pain or Pressure<br />
Difficulty Hearing<br />
Shivering/Chills<br />
Irregular Heart Beat<br />
Ringing, Buzzing<br />
Generalized Weakness<br />
Palpitations/Skipped Beats<br />
Wear a Hearing Aid<br />
Unexplained Weight Loss/Gain<br />
New or Changed Cough<br />
Sneezing/Runny Nose<br />
Excessive Fatigue<br />
Coughing Up Blood<br />
Nosebleeds<br />
Swollen Glands<br />
Wheezing<br />
Difficulty Swallowing<br />
Loss of Consciousness/Head injury Shortness of Breath<br />
Dry Mouth<br />
Loss of Appetite<br />
Night Sweats<br />
Dizziness<br />
Neurological/Psychiatric<br />
Headaches<br />
Numbness or Tingling<br />
Depression/Excessive Anxiety<br />
Insomnia/Difficulty Sleeping<br />
Loss of Memory<br />
Suicide Attempt or Plans<br />
Musculoskeletal<br />
Muscle Pain<br />
Back Pain<br />
Neck Pain<br />
Weakness in Arms/Legs<br />
Swollen or Painful Joints<br />
S:\COLLABORATIVES\Nursing Admin\Independent Contractors\IC Working File\<strong>Medical</strong> <strong>History</strong> <strong>Form</strong> November 2010 - 3 - 5.docx<br />
Eyes<br />
Wear Corrective Lenses<br />
Change in Vision<br />
Lack of Vision in Either Eye<br />
Itching<br />
Tearing<br />
Digestive System<br />
Skin<br />
Genitourinary and Reproductive<br />
Nausea/Vomiting<br />
Rash<br />
Difficult or Painful Urination<br />
Diarrhea<br />
Moles-Changed in Size/Color Blood in Urine<br />
Constipation<br />
Itching<br />
Fertility Problems<br />
Rectal Bleeding or Black Stools Non-healing Wound or Ulcer<br />
Teeth/Gum Disease<br />
Women Only<br />
Men Only<br />
Specify: ______________________ Breast Lump/Discharge<br />
Lump in Testicle<br />
Currently or Possibly Pregnant Impotence<br />
I certify I have answered these questions to the best of my knowledge and the answers are complete and true.<br />
Patient Signature: __________________________________________________________ Date: ___________________<br />
Provider Signature: _________________________________________________________Date: ___________________<br />
Patient 2 nd Injury Review: ____________________________________________________Date: ___________________<br />
Provider Signature 2 nd Injury: _________________________________________________Date: ___________________
S:\COLLABORATIVES\Nursing Admin\Independent Contractors\IC Working File\<strong>Medical</strong> <strong>History</strong> <strong>Form</strong> November 2010 - 3 - 5.docx