Cancer program annual report 2010 - Evangelical Community Hospital
Cancer program annual report 2010 - Evangelical Community Hospital
Cancer program annual report 2010 - Evangelical Community Hospital

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
EVANGELICAL COMMUNITY HOSPITAL<br />
CANCER PROGRAM ANNUAL REPORT <strong>2010</strong><br />
2
EVANGELICAL COMMUNITY HOSPITAL CANCER ANNUAL REPORT <strong>2010</strong><br />
table of contents<br />
A Letter from the Chair.............................................. 1<br />
<strong>Cancer</strong> Liaison Report................................................. 2<br />
<strong>Cancer</strong> Conferences..................................................... 3<br />
<strong>Community</strong> Outreach Program Report.................... 4<br />
Quality Initiatives........................................................ 6<br />
<strong>Cancer</strong> Registry............................................................ 7<br />
Lewisburg <strong>Cancer</strong> Center, Radiation Oncology...... 7<br />
Primary Site Tabulation for 2009 Cases.................... 8<br />
2009 Colorectal <strong>Cancer</strong> Data Analysis for<br />
<strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong>.............................10<br />
<strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong>’s <strong>Cancer</strong> Committee<br />
Commission on <strong>Cancer</strong> CP3R<br />
Quality Measure for Colorectal <strong>Cancer</strong>s................. 13<br />
Front Row, left to right: Vice President-Nursing Paul Tarves, RN, Director of the Thyra M. Humphreys Center for<br />
Breast Health Andrea Bertram, breast health specialist Beth Jordan, CRNP, breast health specialist Billie Jo Day, RN, and<br />
cancer registrar Cynthia Miller.<br />
Back Row, left to right: Vice President-Operations Kendra Aucker, Chief Compliance Officer Matthew Hoeger,<br />
Medical Director of the Thyra M. Humphreys Center for Breast Health John F. Turner, MD, FACS, radiation oncologist<br />
Peter Whitcopf, MD, social worker Mary Pahl. Not pictured are Pathology Services Medical Director John Kryston, DO,<br />
Committee Chairman Bradley Mudge, DO, FACS, ACS representative Karen Maurer, <strong>Community</strong> Health Education<br />
Director Nichole Hockenbrock, recording secretary Alicia Smith, Mayur Patel, MD, James O’Brien, MD, and survivorship<br />
coordinator Michael Hayes, PhD.
A LETTER FROM THE CHAIR<br />
Dear Friends and Colleagues:<br />
“The ‘Paint the Valley<br />
Pink’ campaign in<br />
October <strong>2010</strong> resulted in<br />
a significant increase in<br />
scheduled procedures.”<br />
Bradley Mudge, DO, FACS<br />
I<br />
The CoC’s Accreditations Program<br />
offers many notable benefits that<br />
will enhance a cancer <strong>program</strong> and<br />
its quality of patient care. One of the<br />
steps in the survey process involves<br />
participating in a consultative<br />
evaluation of the <strong>program</strong> performed<br />
by a CoC-trained independent<br />
cancer <strong>program</strong> consultant. This<br />
consultative evaluation determines<br />
the cancer <strong>program</strong>’s readiness for<br />
the Accreditations Program survey.<br />
am proud to present the <strong>2010</strong> Annual Report for the <strong>Cancer</strong> Program at <strong>Evangelical</strong><br />
<strong>Community</strong> <strong>Hospital</strong>. The <strong>Cancer</strong> Committee’s focus is not only on meeting and<br />
serving the needs of our patients and community, but also to earn accreditation<br />
through the American College of Surgeons Commission on <strong>Cancer</strong> (CoC).<br />
On October 5, <strong>2010</strong>, we were<br />
evaluated by an independent<br />
consultant; I am pleased to <strong>report</strong> we<br />
had a successful evaluation. I would like<br />
to thank the <strong>Hospital</strong>’s Administration,<br />
<strong>Cancer</strong> Committee members and all<br />
support staff for their hard work and<br />
dedication to make this possible. Our<br />
<strong>Cancer</strong> Program will be surveyed by<br />
CoC’s Accreditations Program in 2011.<br />
For our patients and the community,<br />
the quality standards established by<br />
the CoC ensure the following:<br />
• Comprehensive care including a<br />
complete range of state-of-the-art<br />
services and equipment<br />
• A multidisciplinary team approach<br />
to coordinate the best available<br />
treatment options<br />
• Information about evidence-based<br />
national treatment guidelines<br />
• Access to prevention and early<br />
detection <strong>program</strong>s, cancer<br />
education and support services<br />
• A cancer registry that offers<br />
lifelong patient follow-up<br />
• Ongoing monitoring and<br />
improvements in cancer care<br />
• Quality care in our community<br />
In addition to 2009 statistical data<br />
regarding the number of patients<br />
and the types of cancer encountered,<br />
this <strong>report</strong> offers insight into our<br />
clinical care, education and support<br />
<strong>program</strong>s. Our area of focus for this<br />
<strong>report</strong> is colorectal cancer. The <strong>annual</strong><br />
<strong>report</strong> reflects our activities for <strong>2010</strong><br />
and our commitment to providing<br />
our patients with compassionate,<br />
high-quality care.<br />
Sincerely,<br />
Bradley Mudge<br />
Bradley Mudge, DO, FACS<br />
Chair, <strong>Cancer</strong> Committee<br />
<strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong><br />
1
cancer liaison <strong>report</strong><br />
The year <strong>2010</strong> has been marked by many accomplishments for the <strong>Cancer</strong> Committee at<br />
<strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong>. For the first time on a consistent basis, Continuing Medical<br />
Education (CME) credits are available for physician participants and Continuing Education<br />
Units are available for all other participants in cancer conferences (Tumor Board).<br />
2<br />
“Many thanks are due to<br />
Cynthia Miller, CTR, for<br />
her diligence in collecting<br />
the Tumor Registry<br />
data and in readying us<br />
for the upcoming CoC<br />
accreditation survey.”<br />
John F. Turner, MD, FACS<br />
We are seeing increased primary care<br />
participation in cancer conferences<br />
and continue to work towards even<br />
greater participation. Care for our<br />
patients has been positively impacted<br />
by the involvement of their primary<br />
care providers in these conferences.<br />
Currently, all cases presented at the<br />
weekly breast Virtual Tumor Board<br />
and the majority of cases presented at<br />
the monthly General Tumor Board are<br />
presented prospectively (during the<br />
active decision-making process, prior to<br />
definitive therapy).<br />
We once again had a very successful<br />
Mammathon, making more than 4,000<br />
calls and speaking with more than<br />
1,600 women. Close to 900 committed<br />
to have their mammogram and 164<br />
scheduled their mammogram that day<br />
for a positive outcome of 53 percent.<br />
We served more than 100 women at<br />
the <strong>annual</strong> Women’s Health Screening<br />
event.<br />
As our tumor registry continues to<br />
grow, we are receiving valuable data,<br />
which influence the organization and<br />
procedures of our cancer <strong>program</strong>s<br />
and are utilized in analyzing the quality<br />
of cancer care. Gary Ayers, DO, and<br />
the director of the Gastrointestinal<br />
Malignancy Clinic, will be discussing<br />
the registry’s colon cancer statistics<br />
elsewhere in this <strong>report</strong>.<br />
Below are the data from the registry<br />
entered into the American College of<br />
Surgeons Commission on <strong>Cancer</strong> (CoC)<br />
CP3R quality measures for breast cancer<br />
study:<br />
1. Radiation therapy is administered<br />
within one year (365 days) of<br />
diagnosis for women under age 70<br />
receiving breast-conserving surgery<br />
for breast cancer.<br />
• 100 percent compliance<br />
2. Combination chemotherapy is<br />
considered or administered within<br />
four months (120 days) of diagnosis<br />
for women under age 70 with<br />
American Joint Committee on <strong>Cancer</strong><br />
(AJCC) T1CN0M0, or Stage II or III<br />
hormone receptor negative breast<br />
cancer.<br />
• 100 percent compliance<br />
3. Tamoxifen or third-generation<br />
aromatase inhibitor is considered or<br />
administered within one year (365 days)<br />
of diagnosis for women with AJCC<br />
T1CN0M0, or Stage II or III hormone<br />
receptor positive breast cancer.<br />
• 27/28 patients met this criterion<br />
(96 percent)<br />
• One patient had hormonal<br />
treatment delay due to<br />
complications during<br />
chemotherapy treatment<br />
Additionally, the surgeons at the Thyra<br />
M. Humphreys Center for Breast Health<br />
participated in the Mastery of Breast<br />
Surgery quality measure database, and<br />
our results compared quite favorably<br />
with breast surgeons across the nation<br />
in relation to three quality measures.<br />
Sincerely,<br />
John F. Turner<br />
John F. Turner, MD, FACS<br />
<strong>Cancer</strong> Liaison Physician, Breast Surgeon<br />
<strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong>
<strong>Cancer</strong> conferences<br />
<strong>Cancer</strong> conferences, also known as tumor boards, are essential forums<br />
to provide multidisciplinary consultative services for patients, and<br />
offer education to physicians and healthcare providers. <strong>Cancer</strong> conferences<br />
are a requirement for an accredited <strong>program</strong> by the CoC.<br />
The number of cases presented each year<br />
is based on a percentage of <strong>annual</strong> analytic<br />
cases added to the cancer registry database.<br />
The CoC requires that at least 10 percent of<br />
the <strong>annual</strong> analytic cases be presented, and<br />
75 percent of the cases discussed need to<br />
be presented prospectively with appropriate<br />
stage documented for the five major sites<br />
seen at our facility. Nationally recognized<br />
treatment guidelines such as those outlined<br />
by the National Comprehensive <strong>Cancer</strong><br />
Center Network need to be considered when<br />
discussing treatment options.<br />
In <strong>2010</strong>, there were 11 multidisciplinary<br />
cancer conferences held at <strong>Evangelical</strong>.<br />
Primary sites presented were colorectal, lung,<br />
prostate, small bowel, lymphoma, thyroid,<br />
endometrial, pancreas, bladder, testis,<br />
thymus, salivary gland and esophagus. A<br />
site-specific conference is held every Tuesday<br />
that includes all breast cases. Diagnosis and<br />
treatment recommendations are discussed.<br />
Primary care physician participation is<br />
encouraged for all cancer conferences and<br />
was a clinical goal the <strong>Cancer</strong> Committee<br />
achieved in <strong>2010</strong>.<br />
David Hicks, MD, from the University of<br />
Rochester, presented Her2-positive Breast<br />
<strong>Cancer</strong>/Diagnostic Tools and Challenges to<br />
the Medical Staff in March. This educational<br />
activity was in addition to the multidisciplinary<br />
cancer conference; CME credits were<br />
provided to the attendees. In April, the<br />
<strong>Cancer</strong> Committee offered educational<br />
sessions to the Medical Staff and allied health<br />
professionals on AJCC staging for breast,<br />
colon, lung and thyroid cancer.<br />
Beginning in March <strong>2010</strong>, <strong>Evangelical</strong><br />
partnered with Geisinger Medical Center,<br />
and CME credits were granted to Tumor<br />
Board/cancer conference attendees.<br />
In <strong>2010</strong>, there were<br />
11 multidisciplinary<br />
cancer conferences<br />
held at <strong>Evangelical</strong>.<br />
3
<strong>Community</strong> outreach <strong>2010</strong> Program <strong>report</strong><br />
subcommittee Members: Mayur Patel, MD (Co-Chair), Nichole Hockenbrock (Acting Co-Chair), Billie Jo Day, RN, Cynthia Miller, Karen Maurer (American<br />
<strong>Cancer</strong> Society), Chuck Stahl (<strong>Community</strong> member), Carol Yost (<strong>Community</strong> member)<br />
Key: ACS–American <strong>Cancer</strong> Society, CBH–<strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong>’s Thyra M. Humphreys Center for Breast Health, EASC–<strong>Evangelical</strong> Ambulatory<br />
Surgical Center, MCR–Middleburg <strong>Community</strong> Room, CHC–<strong>Community</strong> Health Education Center, SVM–Susquehanna Valley Mall, POB–Professional Office Building<br />
4<br />
Supportive Services<br />
Look Good …Feel Better—a partnership with an<br />
American <strong>Cancer</strong> Society Program in CHC<br />
<strong>Cancer</strong> Support Group held in conjunction with<br />
<strong>Cancer</strong> Care of Central PA<br />
<strong>Cancer</strong> Support Group—community members<br />
meet in our community conference room for<br />
group meetings in MCR<br />
*Mammogram Screening—under- and<br />
un-insured women (CBH) funded by the<br />
Northeastern Pennsylvania Affiliate of Susan G.<br />
Kommen for the Cure<br />
Health Screening for the underand<br />
un-insured<br />
Prevention & Early Detection Programs<br />
Tobacco/Smoking Education (employee <strong>program</strong>)<br />
at T-Ross Brothers Construction<br />
Date<br />
Presented<br />
Held every<br />
month<br />
Second<br />
Wednesday of<br />
most months<br />
Held every<br />
other month<br />
Throughout<br />
the <strong>2010</strong><br />
calendar year<br />
Outcomes/Findings<br />
Date of <strong>Cancer</strong><br />
Committee Review<br />
Actions Recommended<br />
Average monthly attendance = 1-2 women 9/21/<strong>2010</strong> Continue collaboration<br />
with ACS<br />
Average monthly attendance = 5-7 participants 9/21/<strong>2010</strong> Work with marketing<br />
to aid in the promotion<br />
of the group/conduct a<br />
survey of participants<br />
Average monthly attendance = 10 participants<br />
209 screenings to date. Findings: 180 normal screening results, 29<br />
required additional imaging, 7 required biopsy (6 biopsies were<br />
benign to date), 14 required 6-month follow-up.<br />
1/22/<strong>2010</strong> 54 persons in attendance, 17 self-breast exams, 3 referred for<br />
additional testing<br />
Date<br />
Outcomes/Findings<br />
Presented<br />
3/4/<strong>2010</strong> 33 participants<br />
Sun Safety Education at Turbotville Preschool 4/7/<strong>2010</strong> 12 participants<br />
Mammathon with CBH held at the SVM 4/14/<strong>2010</strong> 6,426 calls were made, spoke to 1,930 women, left 1,758<br />
messages about early detection, commitments from 1,116<br />
women to schedule their mammograms, 197 mammograms<br />
were scheduled during the event.<br />
Skin <strong>Cancer</strong> Educational Program at<br />
4/20/<strong>2010</strong> 15 participants<br />
TPA worksite<br />
Clear the Air sm — tobacco cessation <strong>program</strong> 4/26/<strong>2010</strong> 2 participants<br />
(Highmark) with CHC<br />
Men’s Health Screening—screening for prostate,<br />
skin, oral and colorectal cancer at POB<br />
6/5/<strong>2010</strong> 54 participants, 9 men required follow-up for suspicious lesions.<br />
1 positive occult blood for follow-up. 1 elevated PSA required<br />
follow-up.<br />
Date of <strong>Cancer</strong><br />
Committee Review<br />
Actions Recommended<br />
7/20/<strong>2010</strong> Continue <strong>annual</strong> event
Prevention & Early Detection Programs<br />
Sun Safety Education Program held for<br />
CONCERN employees<br />
Clear the Air sm —Tobacco Cessation Program<br />
(Highmark) with CHC<br />
<strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong><br />
Employee Health Fair<br />
Women’s Health Screening and *Mammogram<br />
Screening (CBH) skin, breast, colorectal and<br />
cervical cancer<br />
Life After Loss Bereavement Support Group, held<br />
in conjunction with <strong>Evangelical</strong> Hospice<br />
“Paint the Valley Pink” Marketing Initiative for<br />
Breast <strong>Cancer</strong> Awareness<br />
Breast <strong>Cancer</strong> Education in partnership with the<br />
ACS at Northumberland National Bank Health Fair<br />
I Can Cope Program for the Breast <strong>Cancer</strong><br />
Survivor (CBH)—support <strong>program</strong> for patients<br />
and family members<br />
Clear the Air sm —Tobacco Cessation Program<br />
(Highmark) with CHC<br />
AIRS (Area Invitation and Recall System)—phone<br />
calls are made to non-compliant women<br />
encouraging them to schedule a mammogram<br />
Date<br />
Presented<br />
7/8/<strong>2010</strong> 18 participants<br />
7/26/<strong>2010</strong> 3 participants<br />
Outcomes/Findings<br />
9/8/<strong>2010</strong> Education on Breast, American <strong>Cancer</strong> Society Resources,<br />
prevention and early detection information and Smoking<br />
Cessation was provided for more than 250 employees and<br />
family members.<br />
9/11/<strong>2010</strong> 73 women screened for colon cancer, 2 positive results; 73<br />
women screened for cervical cancer, 0 follow-ups; 45 women<br />
screened for breast cancer, 2 women required follow-up; 84<br />
women screened for skin cancer, 4 required follow-up.<br />
September- 8 participants<br />
October <strong>2010</strong><br />
October <strong>2010</strong> This was part of the comprehensive breast cancer awareness<br />
<strong>program</strong>—radio, newspaper advertising and outdoor<br />
billboards. The “Paint the Valley Pink” Web site had<br />
18,000 visitors. Approximately 75,000 listeners per day,<br />
which included four radio stations. Newspapers reached<br />
approximately 25,000 persons. Results included a significant<br />
increase in scheduled procedures.<br />
October <strong>2010</strong> 90 participants<br />
October <strong>2010</strong><br />
10/25/<strong>2010</strong><br />
June 2009-<br />
April <strong>2010</strong><br />
30 participants<br />
1,378 phone calls were made, 195 women committed to<br />
scheduling a mammogram, 259 had their mammograms,<br />
256 messages were left, 179 mammograms were scheduled<br />
during the phone call, 208 did not schedule.<br />
Date of <strong>Cancer</strong><br />
Committee Review<br />
Actions Recommended<br />
9/21/<strong>2010</strong> Continue <strong>annual</strong>ly<br />
OTHER: The ACS tracks referrals made to them from the <strong>Evangelical</strong> network. <strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong> network made 42 referrals to the American <strong>Cancer</strong> Society, 62 from<br />
<strong>Cancer</strong> Care of Central PA and 3 referrals from Central Penn Gastroenterology Associates. <strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong> employees participated in the American <strong>Cancer</strong> Society Relay<br />
events, and the <strong>Hospital</strong>, along with Central Susquehanna Surgical Specialists, PC, sponsored area Relays. <strong>Evangelical</strong> was a site for the American <strong>Cancer</strong> Society Daffodil Days.<br />
*<strong>2010</strong> Mammogram Screening Results<br />
5
quality initiatives<br />
The Tumor Board model<br />
ensures that quality is<br />
built into the care process.<br />
Tumor Boards<br />
General Tumor Boards are at the center of the <strong>Cancer</strong> Committee’s quality initiatives at <strong>Evangelical</strong> <strong>Community</strong><br />
<strong>Hospital</strong> and integral to its efforts to offer a comprehensive approach to patient care that involves a wide<br />
range of disciplines. Monthly meetings to discuss prospective cases routinely include surgeons, pathologists,<br />
oncologists, primary care physicians, patient navigators and various other support personnel.<br />
6<br />
By prospectively discussing the case details among personnel with varying<br />
perspectives, the group can come to a consensus on a treatment plan that<br />
offers the patient the greatest opportunity for success, which is based on<br />
National Comprehensive <strong>Cancer</strong> Network (NCCN) evidence-based guidelines.<br />
The <strong>Cancer</strong> Committee believes that this model ensures that quality is built<br />
into the care process.<br />
Quality Initiatives<br />
Because this is a relatively new <strong>program</strong> for the <strong>Hospital</strong>, the quality<br />
initiatives were undertaken on an ad hoc basis as the <strong>program</strong> developed<br />
but were consistently focused on maintaining the quality of the database as<br />
it is the foundation for not only the <strong>Cancer</strong> Committee’s work here at the<br />
<strong>Hospital</strong> but across the entire Registry. The <strong>Cancer</strong> Committee began with<br />
a focus on educating physicians on the proper staging of primary sites and<br />
the associated documentation. Members also realized the need to be able<br />
to survey patients undergoing surgical interventions as part of their cancer<br />
treatment separately from patients utilizing other surgical services. The<br />
<strong>Cancer</strong> Committee is now able to more specifically survey those patients,<br />
which will help gain a better understanding of how they perceived their care<br />
experience. This information will help to identify future quality improvement<br />
efforts. Finally, the <strong>Cancer</strong> Committee will continually benchmark key care<br />
indicators against national standards and follow generally accepted and<br />
scientifically proven methods related to care processes.
lewisburg cancer care, radiation oncology<br />
<strong>Cancer</strong> Registry<br />
The cancer registry is a source of statistics<br />
and data for research, presentations, quality<br />
improvement opportunities, productivity<br />
measures and protocol applications. The cancer<br />
registry at <strong>Evangelical</strong> utilizes Electronic Registry<br />
Systems to collect, manage and analyze data<br />
on oncology patients. The American College<br />
of Surgeons Commission on <strong>Cancer</strong> (CoC)<br />
requires registries in approved <strong>program</strong>s to<br />
access, abstract and conduct follow-up activities<br />
for required tumors diagnosed and/or initially<br />
treated at the abstracting facility. The tumors<br />
must meet the criteria for analytic cases<br />
(classes of case 00-22), and pathologically and<br />
clinically diagnosed inpatients and outpatients<br />
must be included. All abstracting is performed<br />
using the CoC Facility Oncology Registry Data<br />
Standards and the Pennsylvania <strong>Cancer</strong> Registry<br />
requirements.<br />
The registry at <strong>Evangelical</strong> is managed by a<br />
Certified Tumor Registrar, who is an active<br />
member of the National <strong>Cancer</strong> Registrar<br />
Association and Pennsylvania Association of<br />
<strong>Cancer</strong> Registrars.<br />
Sincerely,<br />
Cynthia Miller<br />
Cynthia Miller, CTR<br />
<strong>Cancer</strong> Registry Coordinator<br />
<strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong><br />
In October 2009, Peter Whitcopf, MD, joined the staff of <strong>Cancer</strong> Care of Central Pennsylvania<br />
as the radiation oncologist at Lewisburg <strong>Cancer</strong> Care. Dr. Whitcopf trained at the<br />
University of Virginia and worked at the Ephrata <strong>Cancer</strong> Center and Reading <strong>Hospital</strong><br />
prior to moving to Selinsgrove. This year, the radiation oncology department has treated<br />
patients mostly for breast, prostate and lung cancer.<br />
The treatment unit at Lewisburg <strong>Cancer</strong> Care is capable<br />
of Intensity-Modulated Radiation Therapy (IMRT), which is<br />
used for nearly all prostate cancer patients and for many<br />
other types of cancer as well. In many situations, IMRT is<br />
better than conventional radiation therapy techniques at<br />
protecting normal tissues from the damaging effects of<br />
radiation while effectively treating the cancer.<br />
Most breast cancer patients receive six to seven weeks of<br />
external-beam radiation therapy, but some patients were<br />
treated with Accelerated Partial Breast Irradiation (APBI),<br />
which is given over just one week, with High Dose-Rate<br />
(HDR) brachytherapy using the Contura balloon catheter.<br />
APBI is an option available for some, but not all, women<br />
with early-stage breast cancer, available through the<br />
Thyra M. Humphreys Center for Breast Health. In selected<br />
patients, the balloon catheter is placed in the tumor cavity<br />
by either John Turner, MD, or Bradley Mudge, DO, and the<br />
patient goes to Lewisburg <strong>Cancer</strong> Care to receive radiation<br />
therapy twice a day for five days.<br />
Additionally, prostate brachytherapy (also known as “seed<br />
implant”) is being offered by urologist Anuj Chopra, MD.<br />
Dr. Chopra performed brachytherapy in Hazleton previously<br />
and now brings his expertise to <strong>Evangelical</strong> <strong>Community</strong><br />
<strong>Hospital</strong>. The procedure is performed as One-Day Surgery<br />
in selected patients with early prostate cancer. Drs.<br />
Chopra and Whitcopf use an ultrasound-guided, real-time<br />
planning technique to precisely place radioactive “seeds”<br />
containing Iodine-125 to irradiate prostate cancers from<br />
within. Many of these patients also receive a course of<br />
hormone-blocking therapy (i.e., Lupron) from Dr. Chopra,<br />
depending on the size of the prostate gland and grade<br />
of the cancer. Thus far, 11 patients have undergone this<br />
procedure since April 6, <strong>2010</strong>.<br />
7
Primary Site Tabulation for 2009 Cases<br />
PRIMARY SITE TOTAL CLASS SEX CS STAGE GROUP<br />
A N/A M F 0 I II III IV UNK N/A<br />
ALL SITES 585 270 315 271 314 58 96 76 48 96 156 55<br />
ORAL CAVITY 4 1 3 2 2 0 1 0 1 1 1 0<br />
LIP 1 1 0 0 1 0 0 0 1 0 0 0<br />
TONGUE 1 0 1 1 0 0 1 0 0 0 0 0<br />
OROPHARYNX 0 0 0 0 0 0 0 0 0 0 0 0<br />
HYPOPHARYNX 0 0 0 0 0 0 0 0 0 0 0 0<br />
OTHER 2 0 2 1 1 0 0 0 0 1 1 0<br />
DIGESTIVE SYSTEM 115 64 51 69 46 14 11 10 14 29 33 4<br />
ESOPHAGUS 10 6 4 7 3 0 0 0 1 4 5 0<br />
STOMACH 10 5 5 8 2 0 0 0 1 3 5 1<br />
COLON 51 30 21 30 21 11 4 8 9 14 5 0<br />
RECTUM 21 12 9 14 7 3 7 2 2 1 6 0<br />
ANUS/ANAL CANAL 0 0 0 0 0 0 0 0 0 0 0 0<br />
LIVER 3 2 1 2 1 0 0 0 0 0 3 0<br />
PANCREAS 15 6 9 5 10 0 0 0 0 7 7 1<br />
OTHER 5 3 2 3 2 0 0 0 1 0 2 2<br />
RESPIRATORY SYSTEM 62 37 25 33 29 0 6 1 12 31 11 1<br />
NASAL/SINUS 0 0 0 0 0 0 0 0 0 0 0 0<br />
LARYNX 0 0 0 0 0 0 0 0 0 0 0 0<br />
LUNG/BRONCHUS 61 36 25 33 28 0 6 1 12 30 11 1<br />
OTHER 1 1 0 0 1 0 0 0 0 1 0 0<br />
BLOOD & BONE MARROW 33 12 21 17 16 0 0 0 0 0 0 33<br />
LEUKEMIA 13 3 10 9 4 0 0 0 0 0 0 13<br />
MULTIPLE MYELOMA 4 0 4 2 2 0 0 0 0 0 0 4<br />
OTHER 16 9 7 6 10 0 0 0 0 0 0 16<br />
BONE 0 0 0 0 0 0 0 0 0 0 0 0<br />
CONNECT/SOFT TISSUE 3 1 2 3 0 0 1 0 0 0 2 0<br />
SKIN 25 6 19 11 14 1 2 2 1 1 18 0<br />
MELANOMA 23 5 18 11 12 1 1 2 1 1 17 0<br />
OTHER 2 1 1 0 2 0 1 0 0 0 1 0<br />
BREAST 123 67 56 1 122 20 37 32 13 9 11 1<br />
8
Primary Site Tabulation for 2009 Cases (cont.)<br />
PRIMARY SITE TOTAL CLASS SEX CS STAGE GROUP<br />
A N/A M F 0 I II III IV UNK N/A<br />
FEMALE GENITAL 45 16 29 0 45 1 12 0 2 6 24 0<br />
CERVIX UTERI 3 2 1 0 3 0 2 0 0 0 1 0<br />
CORPUS UTERI 22 9 13 0 22 0 10 0 0 1 11 0<br />
OVARY 15 5 10 0 15 0 0 0 2 5 8 0<br />
VULVA 4 0 4 0 4 1 0 0 0 0 3 0<br />
OTHER 1 0 1 0 1 0 0 0 0 0 1 0<br />
MALE GENITAL 82 17 65 82 0 0 4 22 1 7 47 1<br />
PROSTATE 78 13 65 78 0 0 0 22 1 7 47 1<br />
TESTIS 3 3 0 3 0 0 3 0 0 0 0 0<br />
OTHER 1 1 0 1 0 0 1 0 0 0 0 0<br />
URINARY SYSTEM 46 18 28 36 10 22 8 7 0 5 2 2<br />
BLADDER 37 12 25 29 8 22 3 7 0 4 1 0<br />
KIDNEY/RENAL 6 5 1 5 1 0 4 0 0 1 1 0<br />
OTHER 3 1 2 2 1 0 1 0 0 0 0 2<br />
BRAIN & CNS 3 1 2 2 1 0 0 0 0 0 0 3<br />
BRAIN (BENIGN) 0 0 0 0 0 0 0 0 0 0 0 0<br />
BRAIN (MALIGNANT) 0 0 0 0 0 0 0 0 0 0 0 0<br />
OTHER 3 1 2 2 1 0 0 0 0 0 0 3<br />
ENDOCRINE 16 14 2 2 14 0 12 0 1 2 1 0<br />
THYROID 16 14 2 2 14 0 12 0 1 2 1 0<br />
OTHER 0 0 0 0 0 0 0 0 0 0 0 0<br />
LYMPHATIC SYSTEM 18 7 11 7 11 0 2 2 3 5 6 0<br />
HODGKIN’S DISEASE 2 1 1 1 1 0 0 0 0 1 1 0<br />
NON-HODGKIN’S 16 6 10 6 10 0 2 2 3 4 5 0<br />
UNKNOWN PRIMARY 9 9 0 5 4 0 0 0 0 0 0 9<br />
OTHER/ILL-DEFINED 1 0 1 1 0 0 0 0 0 0 0 1<br />
Number of cases excluded: 3<br />
This <strong>report</strong> EXCLUDES CA in-situ cervix cases, squamous and basal cell skin cases, and intraepithelial neoplasia cases.<br />
9
2009 Colorectal <strong>Cancer</strong> Data Analysis for <strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong><br />
The <strong>Cancer</strong> Committee at <strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong>,<br />
as part of the <strong>Hospital</strong>’s ongoing effort to improve<br />
cancer care, performs <strong>annual</strong> analyses of cancer-specific<br />
data to assess the effectiveness of treatments provided.<br />
Such analyses are strongly advocated by the American College<br />
of Surgeons Commission on <strong>Cancer</strong> (CoC) so that the institution<br />
can objectively compare its outcomes with nationally recognized<br />
benchmarks. The goal of this undertaking is to demonstrate both<br />
strengths and weaknesses in the institution’s treatment processes<br />
in an effort to improve patient care and survival outcomes.<br />
With respect to colorectal cancer,<br />
the CoC has developed three quality<br />
measures that have been documented in<br />
the medical literature to improve survival<br />
outcomes for colon and rectal cancer:<br />
1. At least 12 regional lymph nodes are<br />
removed and pathologically examined<br />
for resected colon cancer.<br />
2. Adjuvant chemotherapy is considered<br />
or administered within four months<br />
(120 days) of diagnosis for patients<br />
under the age of 80 with American<br />
Joint Committee on <strong>Cancer</strong> (AJCC)<br />
Stage III (lymph node positive) colon<br />
cancer.<br />
3. Radiation therapy is considered or<br />
administered within six months (180<br />
days) of diagnosis to patients under the<br />
age of 80 who have been diagnosed<br />
with AJCC T4N0M0 or Stage III rectal<br />
cancer and who are receiving surgical<br />
therapy for said cancer.<br />
The following data analysis targets the<br />
above numbered quality measures and<br />
also presents a broad overview of the<br />
spectrum of colon and rectal cancer<br />
treated at <strong>Evangelical</strong> during 2009.<br />
10
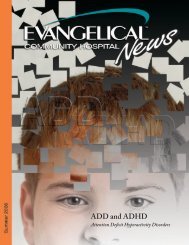
Number of Patients<br />
10<br />
8<br />
6<br />
4<br />
2<br />
0<br />
Figure 1<br />
20-29<br />
30-39<br />
40-49<br />
50-59<br />
60-69<br />
Age Range<br />
70-79<br />
80-89<br />
Female<br />
Male<br />
90-99<br />
Overview<br />
At <strong>Evangelical</strong>, 41 cases of colorectal cancer were treated during<br />
2009. Of those, 59 percent were male and 41 percent were female.<br />
Average age distributions at the time of diagnosis were higher for<br />
males (70-79 years of age) when compared with the female cohort<br />
(60-69 years of age), (see Figure 1).<br />
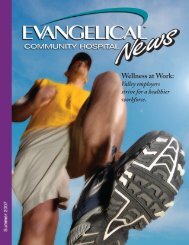
Stage at Diagnosis<br />
With respect to the stage of disease present at the time of diagnosis,<br />
no real trend is apparent insofar as comparative analysis to statewide<br />
data is concerned. It does appear, however, that a significantly higher<br />
number of Stage 0 cancers were surgically treated at <strong>Evangelical</strong><br />
when compared with the rest of the state (see Figure 2).<br />
The bulk of cancers treated at <strong>Evangelical</strong> comprised early stage<br />
cancer, i.e., Stage 0 and I colon cancers. Further illustration of the<br />
stage at the time of diagnosis can be found in Figure 3.<br />
30<br />
25<br />
<strong>Evangelical</strong><br />
PA<br />
19.51%<br />
20<br />
21.95%<br />
Percent<br />
15<br />
10<br />
17.07%<br />
5<br />
5.00%<br />
0<br />
0 I II III IV Unknown<br />
9.76%<br />
14.63%<br />
Figure 2<br />
Stage<br />
Figure 3<br />
12.20%<br />
0 I IV IIA IIIB IIIC IIIA<br />
11
Quality Measure Analysis<br />
Lymph node harvest:<br />
Regarding the first of the aforementioned quality<br />
measures—harvest and analysis of at least 12 lymph<br />
nodes in the resected specimen—<strong>Evangelical</strong> shows<br />
room for improvement: Of all cancers resected at<br />
<strong>Evangelical</strong>, 32 percent were found to have at least 12<br />
lymph nodes in the specimen. The above data include<br />
Stage 0 cancers, which, in essence, represent incidental<br />
findings of carcinoma in polyps<br />
resected endoscopically, which<br />
then go on to oncologic<br />
resection secondary to an<br />
inability to assess for complete<br />
excision on the colonoscopically<br />
resected specimen. One can<br />
argue that such scenarios<br />
should be excluded as there is<br />
no residual carcinoma identified<br />
on the final pathology;<br />
disregarding the Stage 0<br />
resections, however, results in only nominal elevation<br />
of percentage of specimens removed with the requisite<br />
number of lymph nodes: 43 percent.<br />
Lymph node harvests in<br />
excess of 12 nodes have<br />
been shown to increase<br />
survival as a result of<br />
their staging properties.<br />
The author of this <strong>report</strong> undertook analysis of the<br />
data available insofar as the impact of the surgeon,<br />
pathologist and site of the primary tumor was concerned<br />
regarding lymph node harvest. The data demonstrated<br />
no clear trend with respect to the impact of the surgeon<br />
or the pathologist in question. Regarding the site of<br />
the primary tumor, sigmoid resections demonstrated<br />
the largest lymph node harvest with an average of 23<br />
lymph nodes per specimen; this was followed closely by<br />
right colectomies, which demonstrated an average of<br />
14 lymph nodes per specimen.<br />
Discussions have ensued regarding the handling of<br />
pathologic specimens by the pathologists, and it has<br />
been determined that measures are in place to ensure<br />
maximal nodal harvest from the surgical specimen,<br />
namely that of de-fatting protocols to assist in the<br />
identification of mesenteric lymph nodes.<br />
Per the guidelines of the National Comprehensive<br />
<strong>Cancer</strong> Network (NCCN), lymph node harvests in excess<br />
of 12 nodes have been shown to increase survival<br />
as a result of their staging<br />
properties; counter-arguments<br />
would state that adequate<br />
lymph node harvest acts as a<br />
surrogate marker for adequate<br />
resection and, accordingly,<br />
inadequate nodal harvest<br />
reflects inadequate oncologic<br />
resection, thereby leading to<br />
inferior outcomes insofar as<br />
survival is concerned. While it<br />
is a fine point to argue, current<br />
guidelines do recommend for adjuvant chemotherapy in<br />
patients resected with inadequate nodal harvests; this,<br />
in essence, is an argument as to whether or not to treat<br />
Stage II cancers with fewer than 12 lymph nodes in the<br />
resected specimen.<br />
With the advent of novel assays such as the Oncotype<br />
dx colon cancer genomic assay, one could argue the<br />
value of lymph node harvest for Stage II colon cancers.<br />
In essence, the Oncotype dx colon cancer assay is<br />
a genomic assay that assesses the propensity of<br />
recurrence of the primary tumor following resection. A<br />
score is generated based on the assay results, and this<br />
score predicts the probability of local recurrence within<br />
a 36-month period. A lower score portends a lower<br />
likelihood of recurrence. This assay has been utilized by<br />
the author of this <strong>report</strong> to help determine the utility of<br />
adjuvant chemotherapy in Stage II colon cancers with<br />
a great degree of success (admittedly, though, with<br />
a very small cohort of patients). The advocacy of the<br />
NCCN insofar as KRAS mutation and mismatch repair<br />
gene testing is concerned pays homage to the potential<br />
significance of genetic markers and their impact on<br />
colon cancer treatment.<br />
Adjuvant chemotherapy for Stage III cancer:<br />
Eight patients under the age of 80 were surgically resected<br />
for Stage III disease and 100 percent of these patients<br />
were referred for evaluation by Medical Oncology for<br />
the consideration of adjuvant chemotherapy. Complete<br />
compliance in this regard is enthusiastically endorsed<br />
by the author, accompanied by an insatiable desire to<br />
<strong>report</strong> identical results in the ensuing years.<br />
Radiation therapy for rectal cancer:<br />
Zero out of one cases that fulfill the requirements of<br />
this benchmark were referred for radiation therapy. The<br />
precise details of the situation in question are unknown<br />
to the author, so insight into this clinical scenario is<br />
obscure. The benefit of neoadjuvant therapy in rectal<br />
cancer as it pertains to reductions in local recurrence has<br />
been unabashedly endorsed in the medical literature,<br />
and one would be hard pressed to argue against it; that<br />
12
eing said, mitigating circumstances could be present<br />
insofar as reasons against radiation oncology referral are<br />
concerned in this particular case.<br />
Summary and Conclusion<br />
In essence, 41 cases of colorectal carcinoma were<br />
treated at <strong>Evangelical</strong> in 2009. The patient distributions<br />
of age and sex were, essentially, in accordance with<br />
national guidelines. It appears as though there was an<br />
exceptionally high number of early-grade carcinomas of<br />
the colon treated at <strong>Evangelical</strong>. This is likely indicative<br />
of enhanced screening protocols put in place by the<br />
primary care physicians.<br />
The utilization of adjuvant chemotherapy in patients<br />
with Stage III adenocarcinoma was found to be in<br />
100 percent compliance. The utility of radiation in the<br />
context of rectal cancer was sorely understated in the<br />
given study; one could argue the validity of such results<br />
given a patient population of one.<br />
The primary point of contention in the current study is<br />
that of lymph node harvest. Disregarding the Stage 0<br />
carcinomas, the percentage of cases in which 12 or more<br />
lymph nodes were harvested is woefully inadequate.<br />
Analysis of the surgeon and pathologist data failed<br />
to reveal any clear-cut correlation to the analysis in<br />
question. Ultimately, the data presented indicate<br />
that an increase in aggressive surgical intervention is<br />
indicated as it pertains to colorectal surgery. One could<br />
argue that an anticipated increase in vascular injury<br />
might be anticipated as one pursues more aggressive<br />
resections in the context of colorectal cancer, but this<br />
remains to be seen. A counter-argument would be<br />
that of incorporating genomic assays into the staging<br />
of colorectal cancers, which could serve to enhance<br />
staging criteria and potentially lead to a situation in<br />
which aggressive surgical resection is unnecessary.<br />
Commission on <strong>Cancer</strong> CP3R<br />
Quality Measure for Colorectal <strong>Cancer</strong>s<br />
• At least 12 regional lymph nodes are removed and<br />
pathologically examined for resected colon cancer.<br />
• Adjuvant chemotherapy is considered or administered<br />
within four months (120 days) of diagnosis for<br />
patients under the age of 80 with American Joint<br />
Committee on <strong>Cancer</strong> (AJCC) Stage III (lymph node<br />
positive) colon cancer.<br />
• Radiation therapy is considered or administered<br />
within six months (180 days) of diagnosis for patients<br />
under the age of 80 with clinical or pathologic AJCC<br />
T4N0M0 or Stage III and who are receiving surgical<br />
resection for rectal cancer.<br />
<strong>Evangelical</strong> resected colon cases 2009<br />
• Total number of surgical colon cases: 37 (9 cases Stage 0)<br />
• Twelve cases: >12 lymph nodes removed<br />
<strong>Evangelical</strong> Stage III colon cases 2009— patients under the age of 80—<br />
considered or administered chemotherapy within four months (120 days)<br />
• Total number of Stage III colon cases-patient under the age<br />
of 80: 8 of 8 (100 percent)<br />
• All eight cases met this criterion<br />
Radiation therapy is considered or administered to patients under the age of 80 with clinical or<br />
pathologic AJCC T4N0M0 or Stage III rectal cancer.<br />
<strong>Evangelical</strong> had one rectal case in 2009 where the patient was under 80, pathologic Stage IIIB, surgically<br />
resected and received chemotherapy per <strong>Cancer</strong> Care; there is no documentation that the patient was<br />
seen or considered for radiation.<br />
Prepared by Cynthia Miller, CTR<br />
Source: <strong>Evangelical</strong> <strong>Community</strong> <strong>Hospital</strong> Tumor Registry<br />
2009 colorectal cancer cases<br />
13
1<br />
(570) 522-2000<br />
One <strong>Hospital</strong> Drive<br />
Lewisburg, PA 17837<br />
www.evanhospital.com