The LightSpeed root canal instrumentation system - Wiley Online ...
The LightSpeed root canal instrumentation system - Wiley Online ...
The LightSpeed root canal instrumentation system - Wiley Online ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Endodontic Topics 2005, 10, 148–150<br />
All rights reserved<br />
Copyright r Blackwell Munksgaard<br />
ENDODONTIC TOPICS 2005<br />
1601-1538<br />
<strong>The</strong> <strong>LightSpeed</strong> <strong>root</strong> <strong>canal</strong><br />
<strong>instrumentation</strong> <strong>system</strong><br />
E. STEVE SENIA & WILLIAM L.WILDEY<br />
<strong>The</strong> <strong>LightSpeed</strong> s <strong>root</strong> <strong>canal</strong> instrument design is unique in that it has a non-cutting pilot, a very short blade and a<br />
flexible, non-cutting shaft. This allows negotiating 3-dimensional <strong>canal</strong> curvatures with saftey and precision. <strong>The</strong><br />
technique is simple, predictable and similar for all <strong>canal</strong>s. As its name implies, the SimpliFill s obturation technique<br />
is simple to use and unique in that it is the only carrier-based obturation <strong>system</strong> that does not leave the carrier in the<br />
<strong>canal</strong>. It consists of a 5 mm piece of gutta percha (also available in Resilon) that matches the size of the <strong>LightSpeed</strong><br />
preparation for a predictable fit. Backfilling (coronal to the Apical Plug) can be done many different ways. This<br />
article describes a backfilling technique that is fast and simple utilizing a syringe and small gauge needle.<br />
Background<br />
<strong>The</strong> apical area of the <strong>root</strong> <strong>canal</strong> <strong>system</strong> is a critical<br />
region that presents the greatest challenge for instruments<br />
to clean and irrigants to penetrate. <strong>The</strong> quality of<br />
cleaning depends on the pre-<strong>instrumentation</strong> size of<br />
the <strong>canal</strong> and the size of the largest apical instrument<br />
used (Master Apical Rotary (MAR)/MAF). Instruments<br />
smaller than the original apical <strong>canal</strong> diameter<br />
cannot remove infected dentine and it is not likely that<br />
depth of irrigation needle penetration and irrigant<br />
volume will be adequate, in particular in small <strong>canal</strong>s.<br />
Design of the <strong>LightSpeed</strong> (LS)<br />
instrument<br />
LS instruments (<strong>LightSpeed</strong> Technology Inc., San<br />
Antonio, TX, USA) are designed for apical preparation<br />
while providing the correct shape for a quality<br />
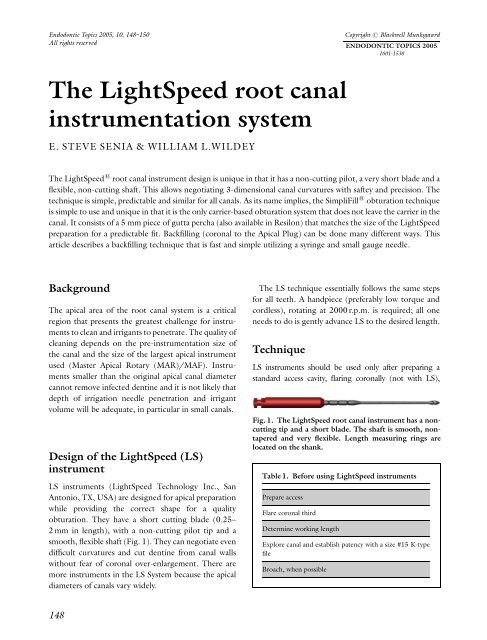
obturation. <strong>The</strong>y have a short cutting blade (0.25–<br />
2 mm in length), with a non-cutting pilot tip and a<br />
smooth, flexible shaft (Fig. 1). <strong>The</strong>y can negotiate even<br />
difficult curvatures and cut dentine from <strong>canal</strong> walls<br />
without fear of coronal over-enlargement. <strong>The</strong>re are<br />
more instruments in the LS System because the apical<br />
diameters of <strong>canal</strong>s vary widely.<br />
<strong>The</strong> LS technique essentially follows the same steps<br />
for all teeth. A handpiece (preferably low torque and<br />
cordless), rotating at 2000 r.p.m. is required; all one<br />
needs to do is gently advance LS to the desired length.<br />
Technique<br />
LS instruments should be used only after preparing a<br />
standard access cavity, flaring coronally (not with LS),<br />
Fig. 1. <strong>The</strong> <strong>LightSpeed</strong> <strong>root</strong> <strong>canal</strong> instrument has a noncutting<br />
tip and a short blade. <strong>The</strong> shaft is smooth, nontapered<br />
and very flexible. Length measuring rings are<br />
located on the shank.<br />
Table 1. Before using <strong>LightSpeed</strong> instruments<br />
Prepare access<br />
Flare coronal third<br />
Determine working length<br />
Explore <strong>canal</strong> and establish patency with a size #15 K-type<br />
file<br />
Broach, when possible<br />
148
<strong>The</strong> <strong>LightSpeed</strong> <strong>system</strong><br />
Table 2. Instrumentation – 5 steps<br />
1. Gauge <strong>canal</strong> to determine its minimum diameter (FLSB)<br />
2. Begin apical <strong>instrumentation</strong> with the FLSB size and end<br />
with the Master Apical Rotary (MAR) size (12 ‘pecks’)<br />
3. Instrument 4 mm short of WL with the next larger size<br />
4. Instrument middle third with three to four larger sizes<br />
5. Recapitulate to WL with the MAR<br />
Table 3. Handpiece movements<br />
Enter <strong>canal</strong> rotating; advance slowly to resistance<br />
From resistance go to WL with an advance/withdraw<br />
motion (pecks)<br />
At WL immediately withdraw from the <strong>canal</strong> (rotating)<br />
Always use a light touch<br />
Table 4. Apical cleaning (FLSB vs. MAR)<br />
Gauging (sizing) finds the smallest diameter (FLSB) of the<br />
<strong>canal</strong><br />
Gauging is done by hand with <strong>LightSpeed</strong> instruments<br />
Rotary <strong>instrumentation</strong> begins with the gauging size<br />
Sequentially larger sizes clean more of the <strong>canal</strong> wall<br />
<strong>The</strong> MAR size ends <strong>instrumentation</strong> (cleans all <strong>canal</strong> walls;<br />
use 12 Pecks Rule)<br />
Fig. 2. SimpliFill is a solid, 5 mm tapered gutta percha<br />
cone attached to a stainless-steel carrier. <strong>The</strong> carrier is<br />
removed from the <strong>canal</strong> after it condenses the cone to<br />
working length (with sealer). <strong>The</strong> middle and coronal<br />
parts of the <strong>canal</strong> are obturated with the technique of<br />
choice.<br />
obtaining working length (WL) and assuring <strong>canal</strong> patency<br />
with at least a loose fitting size 15 K-type file. Canals are<br />
broached when possible to remove pulp tissue (Table 1).<br />
Step 1: <strong>The</strong> original apical <strong>canal</strong> diameter is gauged<br />
(sized) with LS instruments by hand (Table 2). Gauging<br />
Fig. 3. (a) Pre-treatment radiograph of mandibular left<br />
second molar. (b) Post-obturation radiograph: <strong>The</strong> ML,<br />
MB and D <strong>canal</strong>s were obturated apically with SimpliFill<br />
GP Plugs (#60) and AH Plus sealer. <strong>The</strong> middle and<br />
coronal thirds of all <strong>canal</strong>s were obturated with GP and<br />
AH Plus sealer. (c) One-year follow-up radiograph. (Case<br />
by Dr William L. Wildey.)<br />
measures the smallest diameter of a <strong>canal</strong> with LS using<br />
moderate apical force. Begin with a small instrument and<br />
test whether it goes to WL. If it does then it is smaller<br />
149
Senia & Wildey<br />
than the <strong>canal</strong> diameter. <strong>The</strong>refore, try sequentially<br />
larger instruments until one binds before reaching WL.<br />
This instrument is used in the handpiece. However, if<br />
the small instrument selected binds short of WL it is too<br />
large and you should try sequentially smaller sizes until<br />
one goes to WL. You will find that the next larger size<br />
will bind before WL and that is the size used in the<br />
handpiece. With such gauging the instrument size<br />
closely approximates the smallest size of the <strong>canal</strong>.<br />
We call this instrument the FLSB because it is the First<br />
LS instrument size to Bind before reaching WL. Note<br />
that this size is used to begin (not end) <strong>canal</strong><br />
preparation.<br />
Step 2: Begin mechanical <strong>instrumentation</strong> with the<br />
FLSB. All LS instruments are used the same way; with a<br />
slow, continuous apical movement until the blade<br />
binds, a momentary pause, and then advancing it to WL<br />
with intermittent or ‘pecking’ motions (a ‘peck’ is a<br />
short inward and a slight withdrawal motion) (Table 3).<br />
<strong>The</strong> number of pecks required to reach WL will increase<br />
as instrument size increases because more wall dentine<br />
is cut. <strong>The</strong> instrument size that, of itself, requires 12<br />
pecks or more (‘12 pecks rule’) to advance from where<br />
it first binds (and pecking begins) until reaching WL is<br />
called the MAR. <strong>The</strong> MAR is the ‘correct’ instrument<br />
size for proper apical cleaning (Table 4). Smaller sizes<br />
do not clean as well whereas larger sizes may cause overenlargement<br />
and weakening of <strong>root</strong> structure.<br />
Step 3: <strong>The</strong> next larger size is used to instrument to a<br />
length that is 4 mm short of WL using a pecking<br />
motion but without counting pecks. This completes<br />
cleaning and shaping the apical 5 mm of the <strong>canal</strong> for<br />
obturation with a similarly shaped 5 mm SimpliFill<br />
Gutta Percha Plug (<strong>LightSpeed</strong> Technology Inc., San<br />
Antonio, TX, USA) (Fig. 2).<br />
Step 4: <strong>The</strong> middle third of the <strong>canal</strong> is instrumented<br />
with sequentially larger full-size LS instruments (there<br />
is no need to use the half-sizes). When an instrument<br />
no longer advances easily with light pecks, it is<br />
withdrawn from the <strong>canal</strong> and replaced with the next<br />
larger full size. This sequence continues until reaching a<br />
size that does not easily advance beyond the coronal<br />
third of the <strong>canal</strong>. Mid-<strong>root</strong> is usually prepared with<br />
three or four LS instruments.<br />
Step 5: Recapitulate to WL with the MAR. This<br />
ensures a clear path for filling.<br />
Conclusion<br />
Rotary <strong>instrumentation</strong> is an exciting and valuable<br />
advancement in <strong>canal</strong> preparation. Better apical cleaning,<br />
the essence of successful therapy, is now possible<br />
with the latest generation of rotary nickel–titanium<br />
instruments (Fig. 3).<br />
Acknowledgements<br />
<strong>The</strong> assistance of Mr Steven Senia, BSIE, MBA is gratefully<br />
acknowledged.<br />
150