![Absence Management [234kb] - Sunderland City Council](https://img.yumpu.com/28481957/1/500x640/absence-management-234kb-sunderland-city-council.jpg)
Absence Management [234kb] - Sunderland City Council
Absence Management [234kb] - Sunderland City Council
Absence Management [234kb] - Sunderland City Council

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong>
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
Contents:<br />
Chapter<br />
Page<br />
1. Foreword from the Chairman of the Committee 3<br />
2. Scope of Review 4<br />
3. Summary of Recommendations 5<br />
4. Reasons for Review 6<br />
5. Process of Review<br />
Establishing a Focus 8<br />
Evidence Gathering:<br />
Sizing the issue 8<br />
Healthy Workforce 9<br />
A new focus 9<br />
Feedback and Reporting 11<br />
6. Our Findings<br />
Manager Ownership 12<br />
Healthy Workforce 16<br />
Policy 19<br />
Process 20<br />
7. Bibliography 22<br />
1
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
Membership <strong>Council</strong>lors: John Donnelly (Chairman)<br />
Kath Rolph (Vice-Chairman)<br />
Joan Carthy<br />
David Forbes<br />
Bob Heron<br />
George Howe<br />
Bob Kirby<br />
Stuart Porthouse<br />
James Walker<br />
Dennis Whalen<br />
Linda Williams<br />
Peter Wood<br />
Subject<br />
A study into absence management at the <strong>Council</strong><br />
Date of Report June, 2006<br />
Contact<br />
Paul Staines<br />
Review Co-ordinator<br />
0191 553 1006<br />
paul.staines@sunderland.gov.uk<br />
2
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
Foreword from the Chairman of the Committee<br />
“As Chairman of the Policy & Co-ordination Review Committee, I have pleasure in commending this report to you.<br />
I would like to thank anyone who has, in any way, been involved in its preparation.<br />
<strong>Council</strong> services are delivered by staff. Employees are therefore our principal resource in delivering quality services<br />
to residents.<br />
As a Committee, we have looked at how staff attendance is managed - with a vision of providing the best support<br />
available to employees.<br />
We have also looked at whether improved attendance - through the right interventions - can help the authority<br />
meet calls for ‘greater public sector efficiencies’ in Sir Peter Gershon’s report Releasing Resources for the Frontline:<br />
Independent Review of Public Sector Efficiency.<br />
I believe our review has ‘added value’ to work already undertaken and to ongoing debate.<br />
The review is not about weaknesses, but engaging around good practice - both from within the <strong>Council</strong> and elsewhere.<br />
<strong>Council</strong>lor John Donnelly<br />
Chairman, Policy & Co-ordination Review Committee<br />
3
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
2. Scope of the Review<br />
2.1 The key question for us was “what can be done to reduce the <strong>Council</strong>’s overall rate of sickness absence”. Our<br />
review sought to capture:<br />
Within the <strong>Council</strong> -<br />
• What policies there were<br />
• What information was collected - and how was it used<br />
• What management there was of attendance - including developing a healthy workforce; and<br />
• What views there were from staff and the Trade Unions<br />
Outside the <strong>Council</strong> -<br />
• Best practice:<br />
• from similar authorities<br />
• from experience elsewhere in the private and public sector<br />
2.2 In gathering information, we envisaged our study might indicate:<br />
• Underlying reasons for absence (if any)<br />
• Barriers to reducing levels of absence<br />
• Directorate activity to deliver policy<br />
• Directorate activity in promoting and supporting healthy lifestyles<br />
• Individual manager activity in maximising attendance at work<br />
• The role staff had themselves<br />
2.3 By ‘sickness absence’, we mean:<br />
• Short-term illhealth (uncertified but sanctioned by the manager, self certified illhealth<br />
or illness covered by a Doctor’s Note)<br />
• Long-term illhealth<br />
• Unauthorised absence or persistent lateness, for a medical health related reasons<br />
4
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
3. Summary of Recommendations<br />
3.1 Recommendations following our review are:<br />
R1: MANAGER OWNERSHIP: The <strong>Council</strong> should support managers to take more ownership of<br />
absence in their teams<br />
R2: HEALTHY WORKFORCE: The <strong>Council</strong> should seek to mainstream, across all Directorates, equal<br />
access to work-based wellness initiatives<br />
R3: POLICY: The <strong>Council</strong> should consider including in its formal policy a written statement about<br />
the role of the Occupational Health Service and the role of the employee’s ‘friend’<br />
R4: PROCESS: The <strong>Council</strong> should consider reviewing correspondence with employee’s Medical<br />
Practitioners to establish if an alternative to absence is appropriate considering the nature of the<br />
employee’s absence<br />
5
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
4. Reasons for Review<br />
4.1 We chose to study this area for two reasons:<br />
1. Performance & Productivity: Everyone, at all levels in the workforce, feels the impact of illhealth and sickness<br />
absence. It can significantly affect how the <strong>Council</strong> performs and crucially the quality of service to clients<br />
2. Healthy Workforce: The <strong>Council</strong> will always lose some days to absence, but what does it do to<br />
promote good health?<br />
In short, the issue was not stopping/restricting sickness absence, but how best the <strong>Council</strong> could support<br />
and encourage attendance.<br />
4.2 When looking at key national and local drivers we noted:<br />
Healthy<br />
Workforce<br />
The National Picture<br />
<strong>Absence</strong> as a<br />
costed issue<br />
Gershon Efficiencies<br />
Review<br />
<strong>Council</strong> Performance<br />
Previous Committe<br />
Monitoring<br />
Improvement Elsewhere<br />
• The National Picture: Workplace absence rose for the first time in five years (2004 Confederation of British Industry)<br />
costing the UK economy £12.2 billion. The CBI survey (of over 500 organisations) showed an average of 6.8<br />
working days lost per employee in 2004. The Labour Force Survey (collecting information in a reference week)<br />
showed some 1.7 million working days lost (March-May 2004). 2.9% of employees (3.1 in the public sector, 2.8<br />
elsewhere) took at least one day off in the reference week prior to interview. Particular groups most likely to be<br />
absent included women [73.3% of the <strong>Council</strong>’s workforce in 2004/05 were female]<br />
• <strong>Absence</strong> as a Costed Issue. The Chartered Institute for Personnel Development (CIPD) estimates an average<br />
‘cost’ of £601 per employee per year (2005 Survey of policy and practice). Days lost in the public service have an<br />
additional cost on lost personal services to clients. The Chancellor of the Exchequer spoke of seeing a 9%<br />
reduction in the number of days lost to injury and illhealth as part of the 2004 Spending Review<br />
• <strong>Council</strong> Performance: The <strong>Council</strong> had failed to meet its own target of 10.8 days lost per employee in<br />
2003/04. Out-turn data showed 12.9 days. This was a 20% increase on the 10.73 days lost in 2002/03.<br />
12.9 was also the highest figure since data began to be collected in 2000/01:<br />
Best Value Performance Indicator (BVPI) 12 = number of days/shifts lost due to sickness absence<br />
Gateshead Newcastle North Tyneside South Tyneside <strong>Sunderland</strong> National Average<br />
BVPI 12<br />
2001/02<br />
BVPI 12<br />
2002/03<br />
BVPI 12<br />
2003/04<br />
BVPI 12<br />
2004/05<br />
13.3 14.6 8.6 13.1 10.8 10.2<br />
11.3 12.9 10.6 13.7 10.7 10.0<br />
11.7 12.2 11.8 12.6 12.9 10.3<br />
13.21 11.4 12.9 11.46 12.56* 9.71<br />
[* Provided during later stages of the review. Expectations for 2005/06 out-turn are there will be a significant reduction on 2003/04 although figures were not been<br />
concluded by the time of our last Committee meeting on 28th April, 2006]<br />
6
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
The <strong>Council</strong> was also one of only 74 out of 386 authorities where performance was ‘qualified’ by the Audit<br />
Commission - indicating uncertainty of data. Whilst we were happy to note, in the later stages of the<br />
review, <strong>Council</strong> progress since 2003/04, we were aware work remains - as evidenced by the Annual Audit<br />
and Inspection Letter 2004/05. Performance also continued to slip compared to the national average<br />
and some (but not all) Tyne & Wear authorities. Other <strong>Council</strong>s, with similar demographics, had<br />
significantly fewer days lost. Rates exceeded those in other parts of the local economy. Our study into<br />
Contact Centres last year, for example, heard from EDF Energy of circa 6 days lost in their <strong>Sunderland</strong><br />
offices per employee. Although we realise we might not be comparing like with like, there will be<br />
similarities in terms of the catchment area of staff<br />
Significant variations between Directorates were also mapped during the review, (eg in 2003/04 9.31<br />
days were lost in Education and 18.63 days in Social Services).<br />
• Improvement Elsewhere: Analysis of absence in the Civil Service in 2004 showed a headline figure of 9.1<br />
days lost per employee - a fall of .9 days from 2003. At the same time, <strong>Council</strong> rates were rising. We<br />
realise Civil Service jobs are essentially office-based (and a likely comparison for the <strong>Council</strong> would be<br />
Corporate Services with a figure of 9.85 days for the same period)<br />
• Previous Committee Monitoring: We had already expressed concern at the number of employees absent<br />
in excess of 12 months during consideration of the Best Value review of Managing our Employees. An<br />
Action Plan gave 12 key objectives including: aligning policy, ensuring effective ownership, having clear<br />
roles & responsibilities, positioning the <strong>Council</strong> as the employer of choice and delivering cost<br />
effectiveness & improved performance<br />
• Gershon Efficiencies: The Government’s target of a 2.5% efficiency gain over the next three years is<br />
challenging. We envisage reducing sickness absence might be a useful contribution. We see any<br />
contribution as ‘non-cashable’, ie getting greater outputs/improved quality from the same inputs.<br />
<strong>Absence</strong> is also a useful area of focus given there are so few other areas for improvement in the ‘Use of<br />
Resources’ block of the Comprehensive Performance Assessment<br />
• Healthy Workforce: The <strong>Council</strong> will always lose days to absence, but what does it do to promote good<br />
health - and make a broader contribution to ‘a Healthy <strong>City</strong>’ ?<br />
7
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
5. Process of Review<br />
a) Establishing a Focus …<br />
5.1 At our meeting on 23rd June, 2005, we agreed absence management as the focus of ‘policy development<br />
and review’ in 2005/06. Possible topics had been prepared from a canvass of all members of the Committee.<br />
This was supported by an assessment tool to highlight corporate priorities. ‘Policy development and review’ is<br />
one aspect of our work programme and involves detailed analysis of an issue. It provides an opportunity to<br />
assist the <strong>Council</strong> in the development of future policy and practice.<br />
5.2 At our 21st July, 2005 meeting, we discussed how we would approach the study and agreed we would like to<br />
hear from a range of employees, Occupational Health and the Trade Unions (who were contacted about how<br />
they would like to be involved). As a pre-cursor we asked for information from officers on the corporate<br />
approach to absence management.<br />
5.3 Given scrutiny is Member-led, we agreed <strong>Council</strong>lor Kath Rolph, Vice-Chairman, would take an active role in<br />
preparing evidence and reporting to the full Committee.<br />
b) Evidence Gathering …<br />
Sizing the Issue -<br />
5.4 A presentation to our 22nd September meeting addressed baseline information and gave an understanding<br />
of <strong>Sunderland</strong>’s relative position. A copy of the <strong>Council</strong>’s Attendance <strong>Management</strong> Policy & Guidance was<br />
fully set out together with a headcount of the workforce by service area, gender and salary scale. Individual<br />
Directorate sickness rates were also detailed together with generic actions to reduce sickness absence/assist<br />
staff. Headlines from the workforce profile were updated by a report on 23rd March, 2006.<br />
5.5 In 2004/05 causes of sickness absence at the <strong>Council</strong> by full time equivalent days lost were:<br />
Sickness Grouping<br />
FTE days sickness<br />
Vague Condition 39,839.83<br />
Musculo-Skeletal 22,308.98<br />
Psychiatric 21,187.11<br />
Respiratory 14,164.06<br />
Alimentary 8,829.40<br />
Central Nervous System/Eyes & Ears 3,576.94<br />
Endocrine System 3,389.17<br />
Fractures 3,065.69<br />
Pregnancy/Gynaecology related 2,884.57<br />
Cardiac Condition 2,656.64<br />
Dermatology 1,288.28<br />
Renal 925.18<br />
Circulatory 787.35<br />
Haematological 316.10<br />
Poisons 146.88<br />
National Local Government Groupings<br />
8
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
5.6 In terms of % of time lost to the <strong>Council</strong>, this is shown below:<br />
Poisons<br />
Haematological<br />
Circulatory<br />
Renal<br />
Dermatology<br />
Cardiac<br />
5.7 Due to limitations in existing management information systems, it was not possible to deliver a detailed<br />
analysis of statistics without a manual pick of many paper records. Reassuringly, actions were being taken to<br />
address this acknowledged organisational need in a new payroll/HR system system. Cabinet had agreed<br />
funding and this would facilitate real-time monitoring and holistic information to managers and Corporate<br />
Personnel. We also received updated information to our meeting on 23rd March, 2006 providing mid-year<br />
absence statistics and projected outcomes for 2005/06.<br />
Healthy Workforce -<br />
5.8 A report to our 11th November, 2005 meeting focussed on the aspiration of a healthy workforce and how<br />
corporate strategies sought to achieve this goal. The <strong>Council</strong>’s Occupational Health Service Manager set out<br />
key issues from her 2004/05 Annual Report.<br />
c) A New focus -<br />
0.12<br />
0.25<br />
0.62<br />
0.73<br />
1.02<br />
2.11<br />
Gynaecological 2.29<br />
Fractures 2.43<br />
Endocrine 2.69<br />
Central Nerv/Eyes & Ears 2.84<br />
Alimentary 7.01<br />
Respiratory 11.24<br />
Psychiatric 17.34<br />
Muscolo-Skelatal 17.7<br />
% absence<br />
Vague Conditions 31.61<br />
0 5 10 15 20 25 30 35<br />
5.9 Given difficulties in providing data to interrogate, we looked at new ways in which the principal aim of our<br />
review - to help reduce the <strong>Council</strong>’s overall rate of sickness absence - could be delivered. On 11th<br />
November, 2005 we agreed a new focus. This involved both qualitative and quantitative research and<br />
provided for:<br />
• A focus on operational practice rather than the <strong>Council</strong>’s written policy. When compared to the best<br />
performing authorities, there appeared to be few significant differences in written policy - with the<br />
exception of identified roles for Occupational Health and the employee’s ‘friend’ that the <strong>Council</strong> had not<br />
set out<br />
• Analysis of a particular Directorate (Development & Regeneration (D&R)). The Directorate includes a<br />
broad range of job types and is ‘middling’ in terms of sickness levels - ie with no special areas for<br />
attention. D&R also has policies in place to share best practice internally. Staff within the Directorate<br />
were asked for their knowledge and perceptions of the <strong>Council</strong>’s approach to enable - hopefully - a candid<br />
‘SWOT’ analysis to be considered (strengths, weaknesses, opportunities and threats). A total of 684 forms<br />
were distributed. 18% were returned. Whilst this is disappointing, the profile of forms returned indicated<br />
a likely cross section of staff upon which some conclusions might be drawn. A further 15 forms were<br />
received too late to be processed. This brings the total Directorate response to nearly 20%.<br />
9
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
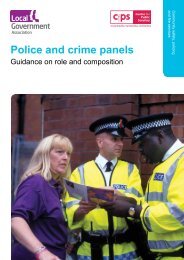
• Best practice advice from Solihull Borough, Manchester <strong>City</strong> and St Helens <strong>Council</strong>s who were best<br />
performing metropolitan authorities in national BVPI 12. Key questions to these authorities were:<br />
Cultural Issues: Growing an attendance culture, quick & long-term wins, the changing pattern of absence<br />
given interventions, remaining ‘hot spots’, the impact of family-friendly and other policies as alternatives<br />
to time off sick and rewards for good attendance<br />
<strong>Management</strong> Ownership & Accountability: Training/enabling managers, sanction against absentees - both<br />
casual and perpetual - and managing contact consistently across the organisation when people are off<br />
The role of Corporate Personnel through the Process: Who leads, Corporate Personnel or managers ?,<br />
making full use of policies and management flexibility, available statistics and the ability to provide detail<br />
(eg on trends)<br />
Sustaining and Improving attendance levels: Plans for the future<br />
<strong>Council</strong>lor Kath Rolph (centre) and council colleagus from Manchester (above) and St Helens (below)<br />
10
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
5.10 We also took the opportunity to gather information on tools that reduced sickness absence, aided<br />
rehabilitation and promoted a healthy lifestyle from a Fit for Life, Fit for Work, Fit for the Future conference<br />
attended by the Vice-Chairman on 6th April. Speakers included:<br />
• Lord Hunt of Kingsheath OBE, Parliamentary Secretary of State at the Department for Work and Pensions<br />
(‘Government Progress & Investment’)<br />
• Dr Sayeed Khan, a Commissioner for the Health and Safety Executive (‘A Guide to Rehabilitation of Sick<br />
Employese’)<br />
• Judith Rasmussen, Regional Director of Sports England (‘Well at Work’)<br />
• David Walker, Acting Regional Director of Public Health for the North East (‘Health at Work: A North East<br />
Perspective’)<br />
• Professor Chris Drinkwater, Head of the Primary Care Development Centre (‘GPs and Sickness <strong>Absence</strong>’)<br />
• Dr Paul Nicholson, Director of Personnel, Proctor & Gamble (Europe/Middle East) (’Promoting Health in a<br />
Multi-National - A Case Study’)<br />
5.11 Timing of this event was particularly useful, as emerging themes from the review could be tested with experts.<br />
d) Feedback and Reporting …<br />
5.12 To ensure a dialogue with staff representatives, the Vice-Chairman met with Trade Unions at the Development<br />
& Regeneration Directorate Joint Consultative Committee on 3rd March, 2006.<br />
5.13 A timetable for delivering recommendations/lead for each recommendation is set out below:<br />
Recommendation<br />
Delivery<br />
Timetable<br />
Lead<br />
1. Manager Ownership Update December, 2006<br />
2. Healthy Workforce Update December, 2006<br />
3. Policy Update December, 2006<br />
4. Process Update December, 2006<br />
Corporate Head of<br />
Personnel<br />
Corporate Head of<br />
Personnel<br />
Corporate Head of<br />
Personnel<br />
Corporate Head of<br />
Personnel<br />
5.14 Recommendations from our review were agreed by the <strong>Council</strong>’s Cabinet on 7th June, 2006 and are now<br />
<strong>Council</strong> policy.<br />
5.15 Copies of all our agenda papers and minutes can be found at www.sunderland.gov.uk or telephone<br />
0191 553 1345.<br />
5.16 As a Committee, we will monitor recommendations by update reports over 2006/07 and 2007/08. Updates<br />
will be scheduled for timely evaluation of progress and take the form of a written report. The Corporate Head<br />
of Personnel will be invited to present the report.<br />
11
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
6. Our Findings<br />
6.1 Findings are set out under each of the Committee’s four recommendations. We have also given an indication<br />
of what our key aspirations are to aid those looking at delivery/future monitoring:<br />
R1: MANAGER OWNERSHIP: The <strong>Council</strong> should support managers to take more ownership of absence in<br />
their teams<br />
A large part of managing absence is about ensuring staff can raise issues before they escalate. Successful<br />
interventions appear to be based on early and informed communication with staff by line managers.<br />
Key aspirations:<br />
• Implementation of a new Payroll/HR System in the autumn of 2006<br />
• Continued ownership of the <strong>Council</strong>’s policy by regularly reviewing manager application<br />
• Data no longer ‘qualified’ by the Audit Commission<br />
• Richer data added, eg from exit interviews<br />
• Continued briefings to staff (including at Team meetings)<br />
• Transferable information across service Business Plans and for exit interviews<br />
• Manager training on absence<br />
• <strong>Management</strong> appraisal on absence management<br />
• Consultation with staff representatives and early roll-out of ‘what works locally’ solutions from the MACS<br />
project<br />
• Further work on:<br />
- Rewards for good attendance - this is a particular issue for us<br />
- The role of the <strong>Council</strong> as an employer of people with a disability<br />
- Assessing the impact of major health inequalities, eg smoking in the workforce<br />
- Contact with employees when ill at home<br />
6.2 The Ministerial Task Force for Health, Safety and Productivity - established by the 2004 Spending Review -<br />
provided two key recommendations on reducing both long-term sickness and self-certification of short-term<br />
absence. These were:<br />
• “Boards (ie the <strong>Council</strong>’s Cabinet) should see absence management as one of their functions”, and<br />
• “In order to influence an attendance culture, absence management should be built into … performance,<br />
efficiency plans and formal reporting”<br />
6.3 We consider action taken by Cabinet to fund a new Payroll/HR system represents a real commitment to<br />
providing tools to understand and manage absence. This decision goes a long way to meeting the first Task<br />
Force recommendation above. We anticipate new and robust data will make full coding of absence possible<br />
and enable benchmarking, target setting and auditing for compliance against policy a lot easier. It is also<br />
envisaged <strong>Council</strong> performance will no longer be classified as ‘qualified’ by the Audit Commission. We believe<br />
that only through effective corporate overview can the <strong>Council</strong> understand where it has a problem, the extent<br />
of illhealth and the best way to tackle it. This is also evidenced, from the 2004/05 Annual Report of the<br />
Occupational Health Unit where it is recognised ‘the unavailability of accurate and current sickness absence<br />
data hampered the management of attendance from a medical perspective’. Paragraph 5.6 above indicates<br />
the largest internal coding for illhealth is at present ‘vague conditions’. This must hinder focus in<br />
Directorates. Although we realise coding is based on national guidance, without internal data or paper search,<br />
in-depth data is difficult to produce and use.<br />
12
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
6.4 We also consider real-time information necessary to test equality and other policies that have a cultural (but<br />
presently unmapped) impact on absence.<br />
6.5 With its new system in place, the <strong>Council</strong> can produce/interrogate data to identify patterns of absence, possible<br />
underlying causes and address ‘hotspots’ early - all evidence we consider necessary for managers and staff<br />
themselves to reduce absence. Phase one of the new system, we understand, is for completion in ‘autumn’ 2006.<br />
6.6 In terms of update reports to this Committee, we look forward to hearing about the impact rich data has<br />
made on managing staff attendance. We pass on a word of caution, however, from colleagues in St Helens<br />
who indicated that because of improved collection, absence figures might initially rise. St Helens also<br />
highlighted that, in their experience as the best performing <strong>Council</strong>, there are no ‘quick fixes’ to be had and<br />
improvements are likely to take a considerable number of years of consistent effort to achieve significant and<br />
sustained reductions in absence. Focus also needs to consider organisational/cultural change issues as well<br />
as an individual’s own absence record. In time we hope, given the flexibilities of the new system, to hear<br />
about how other information - say from exit interview - has been added to aid holistic analysis of cultural<br />
issues. This might assist in understanding some of the mixed messages we received about working for the<br />
<strong>Council</strong>. As an aside, we would suggest that to make information transferable across the organisation a<br />
standard approach is taken both in Business Plans and exit interviews with maybe divisional targets to<br />
achieving the aspiration of fewer days lost are set.<br />
6.7 With an umbrella of corporate information, we suggest data can be used to support an understanding of absence<br />
‘on the shop floor’. We consider there is, for the majority of staff, a deeply engrained culture of attendance bridging<br />
periods of constant change, re-organisation and other workplace stress. 43% of staff took no sick leave at all in<br />
2003/04 for example and only 4% of employees took individual days off. From our research, however, we are not<br />
certain staff understand what is expected of them, what support is available and where to go for help. Our evidence<br />
suggests that, whilst corporate advice has been prepared, it is not always communicated or easy to source when ill.<br />
Not all employees have access to the intranet for example - to self-teach - and D&R staff expressed a mixed picture<br />
about if/when absence was discussed at Team meetings.<br />
6.8 We congratulate Corporate Personnel on two awards in 2005 for delivering flexible working to staff. We also<br />
welcome recent moves to enhance information to employees particularly through the intranet and <strong>City</strong> Talk<br />
(that has a 75% ‘reach’ across employees (2005 Staff Attitude Survey)). We believe this demonstrates a clear<br />
intent to give staff confidence over the corporate commitment to management of attendance, but wonder if<br />
- as ever - more could be done to inform. From our questionnaire, only 19% of D&R staff believed they could<br />
explain the <strong>Council</strong>’s absence policy and 60% of staff were not confident they could at all. 53% of staff<br />
indicated they found out informally about how the policy works and only 34% indicated knowledge came<br />
from induction.<br />
6.9 We also note the corporate commitment to offering alternatives to the ‘nine to five’ that will better fit an<br />
individual’s work/life balance and are pleased, from the 2005 Staff Survey, 72% of staff responding are<br />
satisfied with flexible working opportunities. We note from our survey there appear to be ‘pockets of<br />
dissatisfaction’ (eg around access to career breaks - that might be difficult to plan - for example), but were<br />
generally very impressed with the way D&R had responded to the broad range of absence ‘issues’. We also<br />
commend the service for taking management ownership at Departmental <strong>Management</strong> Team and Head of<br />
Service level of both absence and working to support wellness/work-life balance. This has led to all managers<br />
being provided with details of absences/long-term absence and Return to Work/‘trigger’ point interviews<br />
being promoted through Directorate Personnel. An extension of this cascading of information in other<br />
Directorates - based on experiential feedback from D&R - would be most welcome.<br />
13
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
6.10 In terms of areas for new development, the visits to Manchester and St Helens indicated firmly to us the<br />
importance of ownership by managers to support corporate intent. We believe managers corporately need to<br />
have improved communication with staff in terms of both absence and well-being. There was a 50-50 split<br />
from our D&R survey on whether staff felt managers were sufficiently trained and equipped to deliver support.<br />
We consider that, at present, there may be under-managed sickness as a result of:<br />
• Managers not being fully trained<br />
• A culture in some parts of the organisation suspicious of the management of illhealth (as witnessed by<br />
25% non-attendance at Occupational Health Unit appointments - 252 appointments in 2004/05).<br />
We are confident there are plenty of examples of good practice internally and these need to be shared (eg<br />
communication in D&R). 70% of D&R staff perceived Directorate Support Services to be a useful contact and<br />
these local contacts need to be encouraged.<br />
6.11 We welcome Corporate Personnel’s MACS Project (<strong>Management</strong> of <strong>Absence</strong> Case Study) to provide a firm<br />
business case around manager interventions. The project compares processes in all Directorates using a ‘live’<br />
and a ‘control’ group. Advice can then be given as to interventions, preventions and procedures that are<br />
known to reduce absence. We consider such initiatives are crucial and are based on ‘what works’. We would<br />
ask that messages emerging are shared widely and there is dialogue with the Trade Unions and staff as<br />
further information is published and proposals formalised. To illustrate the impact of MACS interventions, an<br />
outline of two real cases are set out below:<br />
Children’s Services:<br />
£580 Consultant Fee: This early intervention<br />
prevented 3 months absence had the employee had<br />
to wait for an NHS appointment. Not only did the<br />
intervention save 3 months of sickness, it enabled an<br />
approximate saving of £12,000 (12 weeks of supply<br />
teaching costs at £200 per day). The early<br />
intervention also allowed for the recovery period to<br />
be during the summer and, as such, will not count as<br />
sickness.<br />
Although the employee is yet to return to work the<br />
cost of £580 has saved at least £12,000.<br />
Children’s Services:<br />
£110 Consultant Fees. £580 MRI scan. There is a an<br />
18/19 week wait for a MRI scan on the NHS*.<br />
By funding a private scan the <strong>Council</strong> achieved a<br />
potential saving of £20,000 (20 weeks of supply<br />
teaching at a cost of £200 per day).<br />
As the employee accessed an MRI scan as a preventive<br />
measure, they had no prolonged periods of sickness<br />
absence. Therefore, £690 has achieved a saving of at<br />
least £20,000,<br />
*<strong>City</strong> Hospitals <strong>Sunderland</strong>, May, 2006<br />
6.12 To provide a corporate framework we would see, as a first step, all manager training in key responsibilities<br />
(responsibilities likely to already be in their written contacts). There is presently no corporate approach to<br />
manager training on absence. In terms of ‘selling’ this development, we consider managers themselves<br />
would be key beneficiaries as they would be better equipped to manage absence actively rather than<br />
passively that appears to be the case in a number of areas at present. We believe key inter-personal skills do<br />
not automatically come from being appointed ‘a manager’. It is appreciated the <strong>Council</strong> operates a number<br />
of courses managers might access (some of which address absence), but we would expect absence<br />
management training to become mandatory so all managers are aware of support available to them and<br />
necessary competencies around:<br />
14
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
• Policies and procedures<br />
• Their role in absence management (including well-being)<br />
• Legal and disciplinary issues<br />
• Significant Occupational Health inputs available to improve team health<br />
• Operation of trigger points<br />
• Return to Work interview<br />
• Counselling (where they may be required to look at job roles, targets and challenges at work impacting<br />
negatively on attendance)<br />
We also understand that particularly for the management of long-term sickness, managers need crucial skills<br />
to make the right interventions and maintain an appropriate level of contact. Without suitable training, it<br />
would not be surprising if managers were unable to:<br />
• Plan any work to return strategy<br />
• Access professional advice guide/understand treatment or<br />
• Co-ordinate outstanding work<br />
We appreciate this is a big training task - significantly in excess of say the 20 ‘one-off’ sessions provided by<br />
<strong>City</strong> Solicitors on Freedom of Information. Whilst there is no hard evidence to prove it, we also feel - from<br />
anecdotal evidence - ‘rotten eggs stay in the basket the longest’ and perhaps without an element of<br />
compulsion those managers ‘set in their ways’ will never change. For us there is a cultural issue here.<br />
6.13 We would see manager responsibility also formally appraised in terms of:<br />
• service performance over time (reflecting different pressures on each service)<br />
• other types of leave advocated - for example compassionate leave, flexible working arrangements or temporary<br />
redeployment as an alternative to absence<br />
• speed of processing medical certificates and Return to Work interviews<br />
• how staff were apprised of key issues - including specifically at induction and in contact with staff where<br />
reminders/action are required<br />
• how staff accessed corporate support and training<br />
• how staff were appointed and maintained in their work<br />
• how staff were briefed about organisatuional change so that this does not adversely impact on say<br />
stress/illhealth<br />
• discussion at Team meetings. Our survey of D&R indicated absence/well-being support was very rarely<br />
discussed. There were also low levels of recognition for support already available to staff (eg 77% of<br />
respondents were not aware of early intervention stress clinics, 54% of the <strong>Council</strong>’s stop smoking service)<br />
6.14 We would particularly hope for monitoring and support around Return to Work interviews. These are key to<br />
ensuring short-term problems are identified at an early stage and enable mangers to plan cover, for example,<br />
for recovery post elective surgery. We are concerned, from the D&R survey, 47% of staff indicated Return to<br />
Work Interviews do not take place. We accept there may be perceptions at play. However, we would<br />
anticipate all staff would be aware of this process.<br />
6.15 In terms of referral to Occupational Health, we note significant variations across Directorates. In 2004/05,<br />
Education staff made up 45% of all staff (6,478) but accessed only 9% of both health surveillance screening<br />
(24 referrals) and eye tests (68 referrals). D&R, with 5% of staff (709), accessed 19% of health surveillance<br />
screening (49 referrals), and 26% of eye tests (186 - the largest number of referrals of any Directorate).<br />
15
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
6.16 We would argue that better management by managers will reduce the direct cost of absence, better maintain<br />
the quality of public service and improve the satisfaction of other staff working within sections. There were a<br />
number of comments from staff in our survey that particular long-term illhealth by others was having an<br />
impact on their own work. Others thought managers needed to be ‘tougher’ on persistent absentees. We<br />
consider that this might, again, be down to training and recognise that not all mangers have been skilled in<br />
communicating with employees about their health and welfare.<br />
6.17 We would hope that from establishing robust accountability with managers ‘soft’ as well as ‘hard’ information<br />
can be obtained that might be useful in reducing absence. This can be used to promote a virtuous circle to<br />
inform future revisions of policy and practical guidance and suitable future interventions.<br />
6.18 In time, we hope rich information might become available on a number of areas where we feel further work is<br />
required and where we are not able to conclude any firm findings given the need to conclude our review in<br />
2005/06 and the lack of information available. These includes:<br />
• Possible ‘rewards’ for good attendance. We note incentives are valued as a method of rewarding good<br />
attendance in schools and colleges. We wonder why, when someone starts work, initiatives cease to be<br />
viewed as appropriate. Research by the CIPD indicates only 18% of organisations use attendance<br />
initiatives or bonuses as a tool of absence management (CIPD <strong>Absence</strong> <strong>Management</strong>: A survey of policy and practice).<br />
Professional bodies (such as the CIPD) have detailed analysis on possible benefits and we would appreciate<br />
more information. Our questionnaire indicated staff feel more could be done, but we wonder if this is<br />
really appropriate. Colleagues off with say cancer or mental illhealth did not ask to be ill and is 100%<br />
attendance a no guarantee of 100% productivity ?<br />
• Scope for the <strong>Council</strong> to act as community leader and take more risks in say appointing a member of<br />
staff with a limiting disability. In <strong>Sunderland</strong> 32.4% of the adult population are inactive according to the<br />
Department for Work & Pensions. 54% of these are on Incapacility Benefit. In terms of creating a<br />
prosperous and inclusive <strong>City</strong> (<strong>Sunderland</strong> Strategy ambitions) the largest employer in the <strong>City</strong> might want<br />
to support more of this group into jobs. Government’s ambition is that 80% of adults should eventually<br />
be in work, but wouldn’t this have a negative impact on BVPI 12 ?<br />
• The impact of <strong>City</strong> health inequalities. These are already likely to be having an impact on workforce illhealth<br />
although pleasingly 96% of respondents to the 2005 Staff Survey indicated their own state of health was<br />
generally ‘healthy’ to ‘very fit and healthy’. We would not want the <strong>Council</strong> to be complacent about this, however,<br />
as this may be a response based on lowered expectation given the poor heath of the background population. We<br />
would hope the <strong>Council</strong> could progress, for example, systematic plans to address smoking cessation with staff,<br />
diet (in restaurant meal choices) and exercise (through publicising Fitness@ membership) - all of which might be<br />
‘costed’ in terms of long-term benefit v support cost<br />
• Contact at home. Our D&R survey asked if employees would be happy to be contacted or visited at<br />
home. We wanted to see from this what channels of communication were most supported. As a<br />
development area there was some resistance, but not as much as we had expected<br />
R2: HEALTHY WORKFORCE: The <strong>Council</strong> should seek to mainstream, across all Directorates, equal<br />
access to work-based wellness initiatives<br />
Employers, staff and the Trade Unions all have a role to play in establishing environments that<br />
support healthy choices<br />
Our key aspirations:<br />
• A report on how consistency will be assured in accessing Occupational Health across services<br />
• A report on how the <strong>Council</strong> will be responding to chapter 7 of the Choosing Health White Paper<br />
• Access for all office-based staff to a <strong>Council</strong> approved health-based internet site(s), eg NHS Direct<br />
16
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
6.19 It is estimated individuals spend up to 60% of their waking work day hours at their place of employment<br />
(Effectiveness of health promotion in the workplace Peersman, Harden & Oliver, 1998). It is therefore an important place in terms of<br />
physical and mental well-being. Adults who are physically active are up to 50% less likely to develop chronic<br />
health problems of stroke, diabetes, cancer & heart disease (British Heart Foundation). Good physical health is also<br />
associated with reduced stress, anxiety, osteoporosis, osteoarthritis, back pain and hypertension (World Health<br />
Organisation, 2002); all key issues for an employer reflecting on absence management.<br />
6.20 We hear experience from across industry that there are excellent ‘business’ reasons for developing proactive<br />
action and support - particularly through Occupational Health. Proctor & Gamble highlighted how its<br />
approach aimed to achieve ‘zero business interruptions, maintain a productive workforce, optimise employee<br />
productivity and ensure the flow to skills’. This is as true for the production of shampoo as it is for the<br />
delivery of personal services. But for us, as stated at the beginning of the review, staff are our biggest<br />
resource and any absence management framework needs to reflect this at its heart too.<br />
6.21 We feel the <strong>Council</strong> has a big outward looking role in helping to meet the <strong>Sunderland</strong> Partnership aspiration<br />
of a Healthy <strong>City</strong>. With 14,000 employees it can make a big impact on this goal. We recognise the <strong>Council</strong>’s<br />
written commitment to improving the diversity and accessibility of employment for all groups. This has seen<br />
the <strong>Council</strong>’s Human Resources Strategies and Workforce Development Plans aligned to key <strong>Sunderland</strong><br />
Partnership priorities of Creating a Prosperous <strong>City</strong> and Creating Inclusive Communities. For us, there remains<br />
a natural and appropriate ‘trade off’ as Community Leader between median rates of absence and facilitating<br />
access to work for perhaps those with a long-term medical condition.<br />
6.22 Unfortunately the health of the North East (where the majority of staff live) is not good. It has the highest levels of<br />
illness, reported disability and chronic disease in England. According to the Acting Director of Public Health the<br />
region has, in many ways, the health of an eastern - rather than western - European country. This is not to say<br />
health and social care services are poor. Hospitals have high average ‘star’ ratings, there are low/no waiting lists for<br />
acute and elective surgery and there is easy access into primary care and dentistry compared to the rest of<br />
England. Economic factors, a history of high levels of worklessness and longstanding health inequalities have<br />
naturally had their impact on the local labour market. BVPI 12 gives no weight to these wider issues and will<br />
naturally impact on <strong>Sunderland</strong>’s level of sickness absence. We feel that as an indicator BVPI is misleading. No<br />
organisation - particularly one with circa 14,000 staff covering several thousand types of jobs - will ever reach the<br />
‘target’ of 0 days off average per employee. In addition, the composition of the workforce varies between Local<br />
Authorities depending on services they have contracted out.<br />
6.23 We note too that very few workers in the local economy have access to a company occupational health<br />
scheme (estimated by the <strong>Sunderland</strong> Teaching Primary Care Trust to be only 15% - and as low as 3% for<br />
access to a comprehensive service). This is also likely to have an impact on the ‘pool’ of labour available to<br />
the <strong>Council</strong>. We agree the <strong>Council</strong>’s Occupational Health Unit demonstrates a real commitment to well-being<br />
and provides the vital tools to improve the medical management of attendance and to educate and inform<br />
existing staff about maintaining good health. It undertakes significant pre-employment screening and health<br />
assessments (2,720 and 215 cases respectively in 2004/05) and ensures new starters are fit for work. There<br />
will, however, likely remain an impact on the actual level of fitness given the picture of local health<br />
inequalities.<br />
6.24 We welcome significant developments in the <strong>Council</strong>’s Occupational Health Service. This has seen, for<br />
example, a counselling service from June, 2005 and service redesign to create 50% additional capacity. We<br />
believe this new focus will likely have a major and positive impact on reducing absence. Together with<br />
building a secure income-base from work with other authorities/businesses, including a mobile screening<br />
unit (that visited 55 sites in 2004/05) we see a real future for the service. We are concerned, however, at the<br />
growing waiting list for appointments. This is only to be expected as more and more access is encouraged<br />
within limited resources. We hope there is detailed thought being given to service development and would<br />
identify, in terms of Gershon Efficiency savings, there may be opportunities here of ‘spending to save’. We<br />
would see a continued eye being given to management of the service and appreciate the <strong>Council</strong> is<br />
recruiting a new medical practitioner. We also note the <strong>Council</strong> is further reviewing and seeking to<br />
commission in collaboration with others (possibly with Gateshead MBC). This will, no doubt, give synergies<br />
and opportunities to develop corporate intent and roll out access consistently to more and more staff.<br />
17
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
6.25 We are pleased to receive some positive statements on the quality of Occupational Health from D&R staff.<br />
We wonder, however, how well known its services are. 54% of respondents were neutral in terms of how<br />
confident they were the Unit was helping to reduce corporate absence. We would also hope Occupational<br />
Health is not seen culturally in Directorates as ‘an end in itself’ and that managers and staff take full<br />
responsibility to both prevent illhealth (eg time for smoking cessation courses and stabilise illhealth through<br />
referral/attendance at musculo-skeletal injuries sessions). We have a suggestion too at recommendation 4.<br />
to provide more detail on what staff are able to do when ill. As is recognised in the 2004/05 Annual Report,<br />
Occupational Health needs to reflect on how it moves forward. The increased monitoring of attendance<br />
management over the past 12 months has identified the need for a stricter and consistent ‘business<br />
like’application by all those responsible for referral to the service. The need to improve management training<br />
and foster closer co-operation is still very clear. The visit to Manchester <strong>City</strong> <strong>Council</strong> indicates how a more<br />
costed approach benefited both staff (in avoiding manager passivity) and the organisation (in reduced<br />
absence). Is it always fair to every employee to pretend they will be returning to work ?<br />
6.26 We recognise environmental interventions are also key. The Department of Health White Paper Choosing<br />
Health contains a chapter highlighting the importance of wellbeing at work. The White Paper sets out<br />
‘actions for employers, employees and others to extend healthy choices by: improving working conditions to<br />
reduce the cause of ill health related to work’ and ‘promoting the working environment as a source of better<br />
health’. In this vein, the recent extension of the smoke-free environment to all of the Civic Centre and its<br />
grounds is most welcome. Smoking is the biggest cause of preventable death in the <strong>City</strong> (Director of Public Health<br />
Annual Report, 2005). We look forward to extending this to all <strong>Council</strong> buildings as soon as possible and note recent<br />
legislative changes in this area. We also welcome the start of <strong>Council</strong> stop-smoking services and are<br />
disappointed that despite a number of different messages so few staff accessed the service in 2004/05. We<br />
are satisfied in relation to Health & Safety and no concerns were expressed to us by staff during the<br />
consultation survey or discussion with the Trade Unions.<br />
6.27 We welcome work within Corporate Personnel in 2005 to improve the level and accuracy of data on disability<br />
and caring responsibilities. This information, we believe, will address some underlying issues in absence not<br />
considered before. Also welcome are specific questions in the 2005 Staff Survey about staff well-being<br />
shared with us on 20th October, 2005. Key questions measured psychological health, job satisfaction and<br />
workload. Questions were also asked of how people felt about working for the <strong>City</strong> <strong>Council</strong>, addressing issues<br />
of: perceptions of work/job, relations with managers, communication, equality and harassment and<br />
organisational culture - dealing with ‘softer’, but real absence issues for employees. Information on 20th<br />
October also highlighted the ageing workforce that (without wanting to be ageist) will naturally have an<br />
impact of levels of attendance. In 2004/05 58.7% of staff were over 40 years (13.06% over 56).<br />
6.29 As an example of good practice, we welcome the significant commitment of D&R to promote wellness with staff.<br />
This has meant that all Directorate staff have been able to access Know your Numbers (providing information on<br />
blood pressure, stress levels, cholesterol and body mass). Good use is also made of work/life balance tools -<br />
reflecting the fact that staff do not live in a ‘work bubble’ but have carer and other responsibilities. Consultation<br />
with the Trade Unions through the Joint Consultative Committee also provides an opportunity to share ideas and<br />
development. It also gave us some ideas about how we might consult in the future.<br />
6.29 We note, however, that the promotion of wellness is not standard throughout the <strong>Council</strong> and there are<br />
varying degrees of awareness amongst staff. A pilot group of only 30 volunteers are accessing a ‘Wellness’<br />
Programme that includes lifestyle advice and free membership to Fitness@ leisure centres. The Staff Survey<br />
indicated also that 25% of employees were not aware of the 24-7-365 Employee Assistance Programme. For<br />
us workplaces should not be underutilised as a setting for promoting health and well-being. This is<br />
something that employees cannot do for themselves but need assistance from employers - and also the<br />
Trade Unions through promotion - to deliver. The <strong>Council</strong>’s policies permit a flexible element of job and<br />
environmental design and we note that from 2007 new ‘health’ indices will be built in to the Investors in<br />
People Standard and look forward to seeing this integrated as soon as possible in <strong>Sunderland</strong>.<br />
18
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
Phil Barrett, Director of Development & Regeneration (centre) enjoys the Wellness Programme<br />
6.30 We note a number of companies empower staff to monitor their own health through access to established<br />
internet sites. Sites include NHS Direct, the Mayo Clinic and others. We suggest a publicised link from the<br />
<strong>Council</strong>’s own intranet site. NHS Direct, for example, enables employees to find a doctor or dentist, check on<br />
illness, tests and treatment and get advice on common health problems and self help. It also has interactive<br />
quizzes and calculations on say safe drinking and smoking. Professional advice could therefore be extended<br />
to a lot of staff at very little (if any cost) to the <strong>Council</strong>.<br />
6.31 We note from the Vice-Chairman’s visit to Manchester and St Helens there are a range of ‘low level’<br />
interactions that the <strong>Council</strong> could consider. These include:<br />
• ‘Back clubs’ where staff met informally and have lunchtime walks, discussion and support (St Helens)<br />
• Tai Chi - that had proved popular in Manchester<br />
• Volunteer ‘Conciliation Officers’ (Manchester) to provide a ‘friendly ear’<br />
Some of the support available in the North West was through Health Action Zone and local PCT funding - that<br />
may be applicable to <strong>Sunderland</strong> too. We would suggest also that Directorates and the Trade Unions try and<br />
stimulate interest from staff themselves.<br />
R3: POLICY: The <strong>Council</strong> should consider including in its formal policy a written statement about the<br />
role of the Occupational Health Service and the role of the employee’s ‘friend’<br />
There are advantages in setting out the precise role of the Occupational Health Unit and the<br />
employee’s friend<br />
Our key aspiration is:<br />
• Including, within <strong>Council</strong>’s policies, a statement on the role of Occupational Health and the employee’s friend<br />
6.32 We are satisfied the <strong>Council</strong>’s policy meets its obligations under the Employment Rights Act 1999 to both<br />
support the organisation’s business objectives and culture and set out ‘any terms and conditions relating to<br />
incapacity for work due to sickness or injury, including any provision for sick pay’. In addition we believe it<br />
adequately reflects the importance of developing the well-being of the workforce.<br />
19
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
6.33 Although there appears to be no significant difference between the <strong>Council</strong>’s written policy and those of best<br />
performing authorities, we note both Manchester <strong>City</strong> and St Helens identify a specific role for Occupational<br />
Health and the employee’s ‘friend’ throughout the process. Whilst we did not have time to evaluate the<br />
statistical impact of these statements on the performance of the North West authorities, we think spelling<br />
out formal links/standard response times in Occupational Health and the actuality of help from a ‘friend’ is<br />
worth Personnel professionals exploring. We note the <strong>Council</strong>’s policy is under periodic review by a dedicated<br />
Team within Corporate Personnel and look forward to hearing feedback on this idea in due course. What is<br />
clear from all of our research is that Occupational Health needs to have a pro-active and possibly expanded<br />
role to intervene in individual cases at the point most appropriate to that case. This is not just according to<br />
an artificial timetable with ‘trigger points’ set at intervals that may be far too late for the employee. From our<br />
visits, we saw that the main aim of Manchester’s Occupational Health service was to get the employee back<br />
into work. External services were also secured to provide a second opinion for illhealth retirements. We think<br />
this approach offers a number of lessons for <strong>Sunderland</strong> given our own Unit culturally sees itself as working<br />
on behalf of the employee and supports them in their medical condition.<br />
R4: PROCESS: The <strong>Council</strong> should consider reviewing correspondence with employee’s Medical<br />
Practitioners to establish if an alternative to absence is appropriate considering the nature of the<br />
employee’s illness<br />
Further engagement is needed to establish what occupationally can be done to support a medical<br />
diagnosis on a sick note<br />
Our key aspiration is:<br />
• A review of correspondence to ask employee’s GPs specific questions about absence<br />
6.34 We note self-certification by staff is the commonest form of sickness absence (78% of all absence in the<br />
<strong>Council</strong> in 2003/04). It is also where there is most data particularly when supported by a Return to Work<br />
Interview. For GPs we appreciate there is always a duty of care to the patient who may ask for a private sick<br />
note for a certain period of time. For the manager, there may be frustration at a lack of input - particularly if<br />
absence comes ‘out of the blue’ when practical arrangements could have been made for say work at home, a<br />
phased return or reasonable adjustments to the workplace. It is therefore important there is communication<br />
between the <strong>Council</strong> and an employee’s doctor(s). This is an area relatively silent in the <strong>Council</strong>’s policies and<br />
procedures. For us, it is best to focus on what an employee can do rather than a global statement in a sick<br />
note of whether someone is ‘fit’ or ‘unfit’. We feel this applies equally to short and long-term illhealth based<br />
on individual circumstances. If developed (following consultation with staff representatives, such as Trade<br />
Unions) we feel there will be benefits for all including GPs - who we heard had concern at a ‘policing’ role for<br />
employers. We believe strongly it will also give employees a sense they are fully appreciated even if on limited<br />
duties and a win for the <strong>Council</strong> in reduced absence rates. It is worthy of note that in St Helens, the<br />
Occupational Health service and employing Department do not wait until an employee is off for 6 months<br />
before deciding whether to end an employee’s contact on grounds of ill health if there is severe ill health.<br />
This has had a significant impact on their sickness figures<br />
20
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
6.35 We note from Dr Sayeed Khan, Chief Medical Adviser at the Engineering Employers Federation, 2005 research<br />
indicated waiting for the expiry of a sick note was responsible for 26% of all absence. We also note the<br />
importance of early intervention for all parties. If an employee is off work for six months nationally they stand<br />
a 50% chance of returning. If the absence is for one year, there is a 25% likelihood of return and if an<br />
employee is off for two years + there is virtually no chance of return (Clinical Standards Advisory Group report on back pain, 1994).<br />
This is re-enforced throughout the <strong>Council</strong>’s policy & procedures and has been a particular focus for action in<br />
recent months through Case Conferencing. In 2003/04, 4.83% of all <strong>Council</strong> absence was as a result of 32<br />
members of staff being absent for at least one year. This mirrors the national picture. Despite long-term<br />
absence making up 5% of all incidences of absence it accounts for a third of total days lost (Chartered Institute of<br />
Personnel Development, 2001). Whilst every support should be given to staff, Trade Unions and other ‘friends’ to<br />
articulate on behalf of employees in dispute, we believe what should remain central is staff provide services<br />
to the public. <strong>Absence</strong> particularly if medium to long-term adds pressure to service delivery and presents<br />
work pressures to colleagues.<br />
6.36 We would suggest that Corporate Personnel reviews its <strong>Management</strong> of Sickness <strong>Absence</strong> procedures to ask<br />
GPs to produce a letter indicating:<br />
• What is the actual functional problem - rather than a medical diagnosis. What precisely is preventing X<br />
from returning eg stamina, manual handling, mobility, dexterity, levels of concentration ?<br />
• Is the illhealth permanent or temporary - if so for how long ?<br />
• Are there treatments/investigations that might help ? Is he/she on an NHS waiting list?<br />
• What modifications might allow a return to work ?<br />
6.37 In essence, we believe more focussed communication between GPs (and other medical practitioners as<br />
appropriate), managers and the <strong>Council</strong>’s Occupational Health Unit can work together to support an<br />
employee back to work/onto illhealth retirement, etc as soon as possible as this will is only fair to the<br />
employee.<br />
6.38 We note that for both Short/Medium Term and Long-term ill-health procedures, medical input is available<br />
from the <strong>Council</strong>’s Occupational Health Unit, but consider this would be assisted greatly by an earlier<br />
indication of the precise nature of any illness and the views of an employee’s own GP. It will also empower<br />
managers and employees to know the actual impact of illhealth on work, rather than just looking at a medical<br />
prognosis. Given the growth of Practice Based Commissioning for GPs, there is also a likelihood more and<br />
more rehabilitation will become available in community settings - particularly as Doctors under the Quality<br />
Outcome Framework have a new basis for payments by broader well-being outcomes. This may, in part<br />
reduce any pressures on the <strong>Council</strong>’s Occupational Health Service and result in local solutions nearer the<br />
employee’s home.<br />
6.39 In terms of further development, we heard from St Helens <strong>Council</strong> that as a result of developing a partnership<br />
across staff, managers, GPs and Occupational Health it had been possible to have pre-surgical consultation<br />
that would look at the time needed before a return/phased return. This would mean that the employer and<br />
member of staff were not reliant upon a sick note; that experience had indicated was for a longer period than<br />
might actually be necessary for the employee to return to ‘light duties’. This would also mesh with existing<br />
policies including use of public transport/taxis if someone’s only reason for not being at work is because they<br />
couldn’t drive.<br />
21
Report of the Policy & Co-ordination Review Committee<br />
<strong>Absence</strong> <strong>Management</strong><br />
7. Bibliography<br />
2004 Spending Review<br />
(HM Treasury)<br />
2005 Annual Report of the Director of Public Health<br />
(<strong>Sunderland</strong> TPCT)<br />
2005 Staff Attitude Survey Extract<br />
(Policy & Co-ordination Review Committee 20th October, 2005)<br />
2004/05 Annual Audit & Inspection Letter 2004/05<br />
(paragraph 19)<br />
<strong>Absence</strong> <strong>Management</strong>: A survey of policy and practice<br />
(2005, CIPD)<br />
Analysis of Sickness <strong>Absence</strong> in the Home Civil Service 2004<br />
(RED Scientific Ltd)<br />
Annual Efficiency Statement 2005/06 – Mid Year Review<br />
(Cabinet report, 7th December, 2005)<br />
Attendance <strong>Management</strong> Policy & Guidance<br />
(<strong>Sunderland</strong> <strong>City</strong> <strong>Council</strong>)<br />
Best Value Performance Indicator 12 for <strong>Sunderland</strong> <strong>City</strong> <strong>Council</strong>, Tyne & Wear authorities, Solihull Borough,<br />
Manchester <strong>City</strong> and St Helens <strong>Council</strong>s<br />
CB1-AXA Annual Survey of Workplace <strong>Absence</strong><br />
(2004)<br />
Clinical Standards Advisory Group report on back pain<br />
(1994)<br />
<strong>Council</strong>’s Attendance <strong>Management</strong> Policy and Guidance<br />
(2003)<br />
Choosing Health White Paper<br />
(2004 Department of Health)<br />
Effectiveness of health promotion in the workplace<br />
(1998, Peersman, Harden & Oliver)<br />
Employment Rights Act 1996<br />
Health of <strong>Sunderland</strong>, Director of Public Health (2004 Annual Report)<br />
The Labour Force Survey<br />
(Office of National Statistics)<br />
Personnel Committee Agenda, 30th September, 2004<br />
Releasing Resources for the Frontline: Independent Review of Public Sector Efficiency<br />
(July, 2004, report by Sir Peter Gershon for HM Treasury, )<br />
www.nhsdirect.nhs.uk<br />
22