Texas HealTH sTeps - Fostercare Texas
Texas HealTH sTeps - Fostercare Texas
Texas HealTH sTeps - Fostercare Texas

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Texas</strong> Health Steps<br />
Child Health Record Forms<br />
These forms are intended to assist providers<br />
in documenting all required components of the<br />
<strong>Texas</strong> Health Steps medical checkup.<br />
Online Forms<br />
http://www.dshs.state.tx.us/thsteps/forms.shtm<br />
02/2012
Free CE credits. Available 24/7.<br />
Now you can choose the time and place to take the courses you need and want.<br />
We’ve made it easy to take free CE courses online. We offer 24/7 access to more<br />
than 40 courses, including when to refer to a pediatric specialist. And even when you’re<br />
not taking a course, you can access the latest references and resources you need.<br />
The CE courses were developed by the <strong>Texas</strong> Department of State Health<br />
Services and the <strong>Texas</strong> Health and Human Services Commission. All courses are<br />
comprehensive and accredited. *<br />
*Accredited by the <strong>Texas</strong> Medical Association, American Nurses<br />
Credentialing Center, National Commission for Health Education<br />
Credentialing, <strong>Texas</strong> State Board of Social Worker Examiners,<br />
Accreditation Council of Pharmacy Education, UTHSCSA Dental<br />
School Office of Continuing Dental Education, <strong>Texas</strong> Dietetic<br />
Association, <strong>Texas</strong> Academy of Audiology, and International<br />
Board of Lactation Consultant Examiners. Continuing Education<br />
for multiple disciplines will be provided for these events.<br />
Taking New Steps<br />
To view courses online, visit www.txhealthsteps.com.<br />
CE Courses Include:<br />
• When to Refer to a Geneticist<br />
• Children with Diabetes<br />
• Children with Asthma<br />
• Newborn Screening<br />
• Case Management<br />
• Developmental Screening<br />
• Many others<br />
Referral Guidelines<br />
• Pediatric Depression<br />
• High Blood Pressures<br />
in the Office<br />
• Atopic Dermatitis<br />
• Gastroesophageal Reflux<br />
in Infants<br />
• Exercise-Induced Dyspnea<br />
• Referral Guidelines Overview<br />
2/2012 OPE001
How to Complete thE<br />
<strong>Texas</strong> Health Steps<br />
Checkup Forms<br />
The <strong>Texas</strong> Health Steps (THSteps) checkup forms serve as a complete documentation tool for each<br />
specific age (excluding the newborn examination) on the <strong>Texas</strong> Health Steps Periodicity Schedule.<br />
The use of these forms is not mandatory for THSteps providers, but the forms will assist the providers<br />
in assuring documentation of all required components of a THSteps medical checkup.<br />
The front side of each form includes areas of documentation<br />
for the federally mandated components of the checkup,<br />
including “History,” “Immunizations,” “Laboratory,” “Unclothed<br />
Physical Examination,” and “Health Education Including<br />
Anticipatory Guidance.” There is also space available for<br />
“Assessment” of the current checkup and any follow-up<br />
planning and/or recommended referrals to other providers.<br />
Beginning at 6 months of age, the form also includes space for<br />
the required dental referral.<br />
These instructions are organized by each mandated<br />
component. Not all items on the forms are included in these<br />
instructions, as some items are self-explanatory. Items that are<br />
not required for a specific age checkup are not included on the<br />
form for that age.<br />
A notation should be made in each area using the check<br />
boxes or lines provided and space, if needed, to elaborate<br />
on findings. If using the forms in an electronic format, the<br />
spaces are able to be edited and may have a blue shading<br />
that shows over some sections. If that happens and is not<br />
wanted, click on the “Highlight Existing Fields” box in the<br />
upper right-hand corner, and the blue shading will disappear<br />
but the editing feature will remain. The tab feature will move<br />
the cursor through the form. If notations are not made on the<br />
form, supplemental documentation must be maintained in the<br />
medical record. The provider may write “N/A” if not applicable,<br />
use the symbol “Ø” for “None noted,” or write “None.” In areas<br />
with a Y (Yes) or N (No) or a P (Pass) or F (Fail) check box ,<br />
check one of the boxes and notate findings, if appropriate, in<br />
the space provided. If there is a box for a section heading,<br />
check the box if any item(s) was/were addressed.<br />
Demographics<br />
Complete the patient demographic section for each periodic<br />
checkup:<br />
Name = the patient’s name<br />
Medicaid ID = the patient’s Medicaid number<br />
DOB = the patient’s date of birth<br />
Primary Care Giver = the name of the person whom<br />
the patient lives with and who provides care of the patient<br />
Gender = the gender of the patient<br />
Phone = the telephone number where the Primary Care<br />
Giver may be reached for contact<br />
Date of Service = the date of the checkup<br />
Informant = the name of the person accompanying the<br />
patient and who is giving and receiving the information<br />
needed on the patient’s history and the Health Education<br />
and Anticipatory Guidance<br />
NAME:<br />
DOB:<br />
GENDER: MALE FEMALE<br />
DATE OF SERVICE:<br />
hiStorY<br />
MEDICAID ID:<br />
PRIMARY CARE GIVER:<br />
PHONE:<br />
INFORMANT:<br />
uNClothEd phYSiCal ExaM<br />
02/2012<br />
See new patient history form<br />
iNtErVal hiStorY:<br />
NKDA Allergies:<br />
Current Medications:<br />
– 1 –<br />
See growth graph<br />
Weight: ( %) Height: ( %)<br />
BMI: ( %) Heart Rate:<br />
Blood Pressure: / Respiratory Rate:<br />
Temperature (optional):<br />
Normal (Mark here if all items are WNL)<br />
Abnormal (Mark all that apply and describe):<br />
ECord
HISTORY<br />
UNC<br />
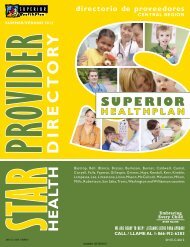
Left side of the front of the checkup form<br />
HISTORY<br />
A comprehensive health and developmental history is a<br />
federally mandated component of the medical checkup and<br />
must be completed at every checkup.<br />
A comprehensive new patient personal and family history form<br />
of the provider’s choosing is completed at the initial checkup as<br />
NAME:<br />
a separate form. It must be retained in the medical record for<br />
reference DOB: at future checkups. For the initial checkup, this box<br />
may GENDER: be checked without the need for further completion of the<br />
interval DATE history OF section. SERVICE: The box is checked at all subsequent<br />
checkups to indicate there is a comprehensive new patient<br />
personal and family health history completed and in the record.<br />
HISTORY<br />
See new patient history form<br />
NAME:<br />
INTERVAL<br />
DOB:<br />
HISTORY:<br />
If the NKDA Allergies:<br />
NAME:<br />
initial comprehensive personal and family health history<br />
GENDER:<br />
was completed previously and is in the record, it is not<br />
DOB:<br />
required<br />
DATE<br />
Current<br />
to<br />
OF<br />
be<br />
Medications:<br />
completed<br />
SERVICE:<br />
at subsequent checkups.<br />
GENDER:<br />
INTERVAL HISTORY<br />
DATE OF HISTORY: SERVICE:<br />
This Visits section to other is completed health-care as an providers, interim history facilities: to supplement<br />
the initial See history new patient and includes history form<br />
HISTORY<br />
documentation of mental<br />
health, INTERVAL developmental, HISTORY: nutritional, and tuberculosis screening.<br />
It also Parental<br />
See NKDA includes new<br />
concerns/changes/stressors<br />
patient items Allergies: that history may form have changed in family since or home: the<br />
comprehensive INTERVAL personal HISTORY: and family health history was<br />
recorded<br />
Psychosocial/Behavioral<br />
or may include additional<br />
Health<br />
information<br />
Issues: Y<br />
that<br />
N<br />
would<br />
Current<br />
NKDA<br />
Medications:<br />
Allergies:<br />
impact Findings: the current checkup.<br />
Current<br />
Visits to<br />
Medications:<br />
other health-care providers, facilities:<br />
Lead questionnaire, risk identified: Y N<br />
TB questionnaire*, risk identified: Y N<br />
List Visits *TB Parental all known skin to other<br />
concerns/changes/stressors test visits if health-care indicated to hospitals, providers, other PPD providers facilities:<br />
in family placed such or home: as<br />
specialists, (See back primary for care forms) physician (PCP) if this checkup is not<br />
performed by the PCP, or facilities, such as radiology or other<br />
Parental DEVELOPMENT:<br />
Psychosocial/Behavioral<br />
concerns/changes/stressors<br />
Health Issues:<br />
in family<br />
Y<br />
or<br />
N<br />
home:<br />
outpatient facilities.<br />
Use Findings: of standardized tool: P F<br />
ASQ* ASQ-SE* PEDS* Other:<br />
Psychosocial/Behavioral *ASQ, ASQ-SE, PEDS, required Health for Issues, use as of including 9/1/11<br />
Maternal<br />
Lead questionnaire,<br />
Depression: Y<br />
risk identified:<br />
N<br />
Y N<br />
Findings:<br />
TB questionnaire*, risk identified: Y N<br />
*TB NUTRITION*: skin test if indicated PPD placed<br />
Problems: (See back Y for forms) N<br />
Mental<br />
DEVELOPMENT:<br />
Assessment:<br />
health screening of the patient is required as part of<br />
• Gross and fine motor development<br />
the comprehensive<br />
DEVELOPMENT:<br />
history. In early infancy, the possibility of<br />
• Communication skills/language development<br />
maternal Use • Self-help/care of depression standardized should skills tool: be considered, P since F this could<br />
impact *See ASQ* • the Social, Bright infant’s Futures ASQ-SE* emotional health. Nutrition development<br />
Document PEDS* Book if needed findings, Other: if any, as space<br />
allows, *ASQ, • on Cognitive ASQ-SE, the form development<br />
PEDS, or on required additional for paper use as as of 9/1/11 needed.<br />
IMMUNIZATIONS<br />
• Mental health<br />
NUTRITION*:<br />
Up-to-date<br />
NUTRITION*:<br />
Problems: Deferred Y - Reason: N<br />
Assessment: Breastmilk<br />
Min per feeding: Number of feedings in last 24 hrs:<br />
Given<br />
Formula<br />
today:<br />
(type)<br />
DTaP HAV HBV HIB IPV<br />
Oz *See Meningococcal<br />
per Bright feeding: Futures Nutrition Number<br />
MMR Book of if feedings needed Pneumococcal<br />
in last 24 hrs:<br />
Water<br />
Varicella<br />
source:<br />
MMR-V HIB-HBV<br />
fluoride: Y<br />
DTap-HIB<br />
N<br />
IMMUNIZATIONS<br />
Solids<br />
DTaP-HB-IPV DTaP-IPV-HIB Influenza<br />
02/2012<br />
– 2 –<br />
See new patient history form<br />
INTERVAL<br />
NAME:<br />
HISTORY:<br />
NKDA Allergies:<br />
DOB:<br />
Lead risk assessment should be done beginning at six months<br />
through<br />
GENDER:<br />
six years through<br />
MALE<br />
anticipatory<br />
FEMALE<br />
guidance. The back of<br />
Current Medications:<br />
the form DATE contains OF SERVICE: questions related to lead risk factors and<br />
information about Form Pb-110, Lead Risk Questionnaire.<br />
Visits hiStoRY<br />
other health-care providers, facilities:<br />
The form is available at<br />
http://www.dshs.state.tx.us/thsteps/forms.shtm See new patient history and may<br />
be completed Parental concerns/changes/stressors for reporting purposes and in faxed family or or mailed home:<br />
inteRVal hiStoRY:<br />
as noted<br />
NKDA<br />
on the bottom<br />
Allergies:<br />
of the form to the Department of<br />
MEDICAID State Health ID: Services (DSHS) Lead Program for every child<br />
PRIMARY screened,<br />
Psychosocial/Behavioral<br />
whether CARE GIVER: or not the<br />
Health<br />
results<br />
Issues:<br />
show a<br />
Y<br />
risk of<br />
N<br />
lead<br />
Findings: Current Medications:<br />
PHONE: exposure. Blood lead screening is required at 12 and 24<br />
INFORMANT:<br />
months.<br />
Visits Lead to questionnaire, other health-care risk providers, identified: facilities: Y N<br />
NAME: TB questionnaire*, risk identified: Y N<br />
UNCLOTHED PHYSICAL EXAM<br />
DOB: *TB skin test if indicated PPD placed<br />
See Parental (See back<br />
growth concerns/changes/stressors for forms)<br />
GENDER: graph MALE FEMALEin family or home:<br />
MEDICAID ID:<br />
Weight:<br />
Screening DATE DEVELOPMENT:<br />
OF for tuberculosis SERVICE:<br />
PRIMARY CARE<br />
(<br />
GIVER:<br />
%)<br />
(TB)<br />
Height:<br />
is a required part<br />
(<br />
of the<br />
%)<br />
history<br />
BMI: at certain Use of ages. standardized ( The questions %) tool: Heart contained Rate: in P the THSteps F TB<br />
Blood MEDICAID PHONE: questionnaire<br />
Psychosocial/Behavioral<br />
Pressure: ID: are located / on<br />
Health<br />
Respiratory the back<br />
Issues:<br />
of Rate:<br />
Y<br />
checkup<br />
N<br />
ASQ* ASQ-SE* PEDS* Other: forms<br />
Temperature:<br />
PRIMARY INFORMANT:<br />
for specific<br />
hiStoRY<br />
Findings:<br />
*ASQ, ASQ-SE, ages CARE and PEDS, GIVER: can required serve as for documentation use as of 9/1/11 for TB<br />
PHONE: screening. Normal See (Mark new patient here if history all items form are WNL)<br />
Abnormal UNCLOTHED INFORMANT: inteRVal NUTRITION*: (Mark all hiStoRY: PHYSICAL that apply and describe): EXAM<br />
Appearance Problems: NKDA deVelopMental Y N Allergies: Nose SCReeninG: Lungs<br />
Head See Assessment: growth graph Mouth/throat Abdomen<br />
UNCLOTHED<br />
Use of standardized<br />
Weight: Skin PHYSICAL<br />
tool: P<br />
( Teeth EXAM<br />
F<br />
%) Height: Genitalia<br />
Current ASQ Medications: PEDS<br />
( %)<br />
BMI: Eyes ( %) Neurological Heart Rate: Extremities<br />
See Autism<br />
Blood Ears<br />
growth screening: graph P F<br />
*See Pressure: M-CHAT Bright Futures / Nutrition Heart Respiratory Book if needed Rate: Back<br />
Weight:<br />
Temperature:<br />
Visits to other ( health-care %) providers, Length: facilities: Musculoskeletal ( %)<br />
Head Abnormal IMMUNIZATIONS<br />
Circumference: findings: ( %)<br />
Heart Normal Rate: (Mark here if all items Respiratory are WNL) Rate:<br />
Temperature:<br />
Abnormal<br />
Developmental Parental nutRition*: concerns/changes/stressors<br />
(Mark<br />
surveillance<br />
all that apply<br />
through<br />
and describe):<br />
6 years in family of age or is home:<br />
Up-to-date<br />
required<br />
as Appearance part Breast Bottle Cup<br />
Normal Deferred of the history,<br />
(Mark- here Reason: with<br />
if Nose use of a validated<br />
all items are WNL) Lungs and standardized<br />
developmental Head Psychosocial/Behavioral Milk (%): screening Mouth/throat tool Health Ounces specific Issues: per ages. day:<br />
Abdomen Y Check N the box in<br />
Abnormal Additional: Solid foods:<br />
front Skin Findings: of the<br />
(Mark<br />
tool used.<br />
all that<br />
Teeth<br />
apply and describe):<br />
Genitalia<br />
Teeth Appearance Juice:<br />
Eyes Given # today: DTaP Nose<br />
Neurological HAV HBV Abdomen<br />
Extremities HIB IPV<br />
OrHead/fontanels Water source:<br />
Ears<br />
Mouth/throat<br />
Heart<br />
Genitalia fluoride: Y N<br />
Meningococcal MMR Back Pneumococcal<br />
Visual Skin Varicella Acuity Screening: MMR-V Neurological HIB-HBV Extremities<br />
Musculoskeletal DTap-HIB<br />
OD Abnormal<br />
Eyes *See deVelopMental / Bright Futures<br />
findings: OS Heart/pulses Nutrition / Book OU if needed<br />
DTaP-HB-IPV DTaP-IPV-HIB<br />
SuRVeillanCe: Back / Influenza<br />
Hearing Ears • Gross Checklist and for fine Parents: Lungs motor development<br />
P F Musculoskeletal<br />
(See LABORATORY<br />
iMMunizationS<br />
• Communication back for form) skills/language development Hips<br />
Abnormal • Self-help/care findings: skills<br />
Up-to-date<br />
HEALTH • Up-to-date Social, EDUCATION/ANTICIPATORY<br />
emotional development<br />
Deferred Reason:<br />
Additional: GUIDANCE • Deferred Cognitive<br />
(See - Reason: development<br />
back for useful topics)<br />
Teeth<br />
• Mental<br />
#<br />
health<br />
Selected Given today: health topics DTaP addressed Hep A in Hep any B of the Hib IPV<br />
Additional:<br />
Visual following nutRition*:<br />
Ordered Acuity MMR areas*: Screening: today: PCV Meningococcal* Varicella<br />
Subjective At ages that<br />
OD • School MMRV /<br />
Vision do not<br />
Readiness<br />
Screening: require a standardized<br />
OS DTaP-Hib • / Nutrition<br />
P<br />
OU DTaP-IPV-Hep F screening tool, the<br />
Breast Bottle Cup / B<br />
Hearing checkup<br />
Hearing • Development DTaP-IPV/Hib<br />
Checklist must include<br />
Checklist<br />
for<br />
for<br />
Parents: a review<br />
Parents: • Safety Influenza<br />
of<br />
P<br />
P milestones<br />
F<br />
F as listed on the<br />
Milk (%):<br />
Ounces per day:<br />
form. (See<br />
•(See Physical<br />
back<br />
back<br />
for<br />
Activity for<br />
form)<br />
Solid<br />
Check<br />
*Special foods:<br />
the<br />
populations: form) box in front of “Developmental Surveillance”<br />
See ACIP<br />
to document Signature/title<br />
Juice: review of milestones.<br />
HEALTH ASSESSMENT<br />
Water laboRatoRY<br />
source: EDUCATION/ANTICIPATORY<br />
fluoride: Y N<br />
GUIDANCE (See<br />
(See<br />
back<br />
back<br />
for<br />
for<br />
useful<br />
useful<br />
topics)<br />
topics)<br />
*See Tests Bright ordered Futures today: Nutrition Book if needed<br />
Selected<br />
Selected<br />
Hgb/Hct<br />
health<br />
health<br />
topics<br />
topics<br />
addressed<br />
addressed<br />
in<br />
in<br />
any<br />
any<br />
of<br />
of<br />
the<br />
the<br />
following<br />
following areas*:<br />
areas*:<br />
• Parental/Maternal iMMunizationS<br />
School Readiness<br />
Well-Being<br />
• Nutrition<br />
• Nutritional Adequacy<br />
• Infant<br />
Development<br />
Behavior<br />
• Safety<br />
• Safety<br />
• Infant-Family<br />
Physical Up-to-date Activity<br />
Harmony<br />
Deferred - Reason:<br />
ASSESSMENT<br />
PLAN/REFERRALS<br />
ASSESSMENT<br />
Signature/title<br />
Dental Given Referral: today: Y DTaP Hep A Hep B Hib IPV<br />
ISIT CHILD CHILD HEALTH HEALTH CHILD RECORD HEALTH RECORD RECORD<br />
See<br />
Weigh<br />
MEDI<br />
BMI:<br />
Blood PRIM<br />
Tempe PHON<br />
INFO Nor<br />
Abnor<br />
unC App<br />
Hea<br />
Skin See<br />
Eye<br />
Weigh Ears<br />
Head<br />
Abnor Heart R<br />
Tempe<br />
Nor<br />
Abnor<br />
App<br />
MEDIC Additio<br />
Hea<br />
PRIMA<br />
Teeth<br />
Skin<br />
PHON Eye<br />
Visual<br />
Ears<br />
INFOR OD<br />
Nos<br />
Hearin<br />
(Se<br />
unCl Abnor<br />
HEAL<br />
See<br />
GUID<br />
Weigh<br />
Head SeleC<br />
Heart followi R<br />
Tempe<br />
Subjec • Sc<br />
Subjec Norm • De<br />
• Ph<br />
Abnorm<br />
heal<br />
ASS Appe<br />
Guid Hea<br />
Skin<br />
Eyes Sele<br />
follow Ears<br />
Nose • Fa<br />
Abnorm • De<br />
• Co<br />
*See B<br />
PLAN<br />
Denta<br />
aSS<br />
Other<br />
Subjec<br />
Return<br />
Subjec<br />
heal plan<br />
Guid<br />
Denta<br />
Signatu Other Sele<br />
followi<br />
• De<br />
Return • Be<br />
• Ro<br />
*See Br<br />
aSSe<br />
Signatu
DPAP-IPV DTaP-HB-IPV DTaP-IPV-HIB Influenza<br />
Current Maternal Medications: Depression: Y N<br />
Normal (Mark here if all items are WNL)<br />
Findings:<br />
Abnormal LABORATORY<br />
(Mark all that apply and describe):<br />
Visits to other health-care providers, facilities:<br />
Appearance Nose Lungs<br />
DEVELOPMENT:<br />
Additional: Head<br />
Up-to-date<br />
Mouth/throat Abdomen<br />
• Gross and fine motor development<br />
Subjective Skin<br />
Deferred - Reason:<br />
Vision Screening: Teeth P F Genitalia<br />
Document Parental • Communication<br />
abnormal concerns/changes/stressors findings<br />
skills/language<br />
and action<br />
development in family taken for home: both the Hearing that Eyes are Checklist ordered. for Separate Parents: Neurological forms P indicating F Extremities laboratory tests<br />
• Self-help/care skills<br />
standardized screenings and the review of milestones in the ordered/results<br />
Ears (See back for form) Heart Back<br />
• Social, emotional development<br />
Ordered today: also serve as sufficient documentation.<br />
Musculoskeletal<br />
space • Cognitive provided development<br />
or on additional paper as needed. Referral<br />
Psychosocial/Behavioral Health Issues: Y N<br />
Abnormal<br />
for further • Mental assessment health can be documented in the “Plan/ HEALTH findings: EDUCATION/ANTICIPATORY<br />
Findings:<br />
Referrals” section.<br />
GUIDANCE (See back for useful topics)<br />
Signature/title<br />
Selected health topics addressed in any of the<br />
NUTRITION*:<br />
Lead questionnaire, risk identified: Y N<br />
Additional:<br />
following areas*:<br />
TB Breastmilk questionnaire*, risk identified: Y N<br />
Teeth The person # completing the checkup and the staff assisting<br />
• Parental/Maternal Well-Being • Nutritional Adequacy<br />
*TB Min per skin feeding: test if indicated Number of feedings PPD placed in last 24 hrs: in completion of the checkup sign on the line with their title<br />
• Infant Behavior<br />
• Safety<br />
(See Formula back (type) for forms)<br />
Audiometric included. Screening:<br />
• Infant-Family Harmony<br />
Oz per feeding: Number of feedings in last 24 hrs: R 1000Hz 2000HZ 4000HZ<br />
Water source: fluoride: Y N L<br />
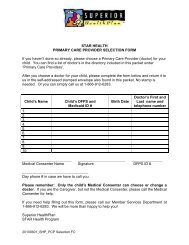
ASSESSMENT<br />
Right 1000Hz side of the 2000HZ checkup form4000HZ<br />
DEVELOPMENT:<br />
Solids<br />
NAME:<br />
MEDICAID ID:<br />
Use of standardized tool: P F<br />
Visual Acuity Screening:<br />
*See ASQ* Bright DOB: Futures ASQ-SE* Nutrition PEDS* Book if needed Other:<br />
OD Unclothed PRIMARY / CARE OS Physical GIVER: / OU Exam/<br />
*ASQ, GENDER: ASQ-SE, PEDS, required for use as of 9/1/11<br />
A comprehensive PHONE: unclothed physical examination including a<br />
ORIMMUNIZATIONS<br />
HEALTH EDUCATION/ANTICIPATORY<br />
DATE OF SERVICE:<br />
graphic INFORMANT: recording over time of measurements for comparison<br />
GUIDANCE (See back for useful topics)<br />
NUTRITION*:<br />
Up-to-date<br />
to national norms for the patient’s age is a federally required<br />
Problems: Deferred Y - Reason:<br />
component of the checkup.<br />
HISTORYN<br />
Selected UNCLOTHED health topics PHYSICAL addressed in any EXAM of the<br />
Assessment:<br />
NAME:<br />
following MEDICAID areas*: ID:<br />
See new patient history form<br />
• School See Readiness/Limitations<br />
growth graph<br />
• Nutrition<br />
Given DOB: NAME: today: DTaP HBV HIB IPV<br />
• Personal PRIMARY Hygiene<br />
• Safety<br />
*See Pneumococcal Bright INTERVAL Futures Nutrition HISTORY:<br />
MEDICAID CARE<br />
HIB-HBV Book if needed DTap-HIB PLAN/REFERRALS<br />
Weight: ID: GIVER:<br />
( %) Height: ( %)<br />
GENDER:<br />
Rotavirus DOB: NKDA<br />
DTaP-IPV-HBV<br />
Allergies:<br />
Check PHONE:<br />
DTaP-IPV-HIB Other PRIMARY BMI: the box CARE to ( indicate GIVER: %) the growth Heart graph Rate: has been<br />
IMMUNIZATIONS<br />
Referral(s):<br />
ASSESSMENT<br />
DATE completed Blood Pressure: and measurements / are Respiratory notated on Rate: the graph<br />
GENDER: OF SERVICE:<br />
INFORMANT:<br />
PHONE:<br />
Nutrition screening is a required part of the history. For younger<br />
LABORATORY<br />
NAME:<br />
retained MEDICAID Temperature: in the record. ID: Resources for growth may be found<br />
ages, Up-to-date notate DATE Current the OF Medications:<br />
type SERVICE: of nutrition and the amount received as at http://www.dshs.state.tx.us/thsteps/forms.shtm.<br />
INFORMANT:<br />
Normal (Mark here if all items are WNL) The<br />
appropriate. Up-to-date Deferred HISTORY<br />
DOB:<br />
For - Reason: ages without an age-specific nutrition review,<br />
UNCLOTHED PRIMARY CARE PHYSICAL GIVER: EXAM<br />
measurement area provided for notating during the visit is<br />
check Deferred the GENDER: Y or - N Reason: box assessed and notate any appropriate Return PHONE: Abnormal to office: (Mark all that apply and describe):<br />
HISTORY<br />
Visits See to new other patient health-care history form<br />
then UNCLOTHED optional<br />
providers, facilities:<br />
See Appearance growth for use. graphPHYSICAL Nose EXAMLungs<br />
findings DATE in the “Assessment” space in this section. If needed<br />
Ordered Given INTERVAL NAME:<br />
OF SERVICE:<br />
INFORMANT:<br />
today: today: DTaP HAV HBV HIB IPV<br />
Head Mouth/throat Abdomen<br />
for completion See new of this patient HISTORY:<br />
item, history refer to form<br />
Weight: MEDICAID ID:<br />
Bright Futures at http://www. See<br />
Meningococcal Other<br />
MMR Pneumococcal<br />
Skin<br />
growth graph ( %) Length: ( %)<br />
DOB: NKDA Allergies:<br />
BMI: PRIMARY ( CARE %) GIVER: Head Teeth Circumference: Genitalia ( %)<br />
brightfutures.org/nutrition<br />
Varicella HISTORY<br />
INTERVAL Parental concerns/changes/stressors MMR-V HISTORY: as indicated<br />
HIB-HBV<br />
by the in asterisk. family DTap-HIB or home: PLAN/REFERRALS<br />
UNCLOTHED Heart Weight: Eyes Rate: ( PHYSICAL Neurological %) Respiratory Length: EXAMExtremities<br />
( %)<br />
GENDER:<br />
DPAP-IPV NKDA MALE<br />
DTaP-HB-IPV Allergies: FEMALE<br />
DTaP-IPV-HIB Influenza The<br />
BMI: PHONE:<br />
Rate:<br />
Temperature: form<br />
Ears<br />
allows<br />
(<br />
space<br />
%)<br />
for<br />
Head Heart<br />
documenting<br />
Circumference:<br />
the physical<br />
Back ( %)<br />
Current<br />
Immunizations<br />
DATE See new OF Medications: SERVICE: patient history form<br />
Dental Heart INFORMANT:<br />
See Referral: Rate: growth Y graph Respiratory Rate: Musculoskeletal<br />
Signature/title LABORATORY<br />
Psychosocial/Behavioral Health Issues: Y N Signature/title<br />
Other examination<br />
Temperature:<br />
Abnormal Referral(s) Normal and (Mark findings.<br />
findings: here if all items are WNL)<br />
Age-appropriate<br />
INTERVAL Current Medications:<br />
Findings: screening<br />
HISTORY:<br />
and administration of<br />
Weight: ( %) Length: ( %)<br />
Visits to other health-care providers, facilities:<br />
Abnormal Normal (Mark here all that if all apply items and are describe):<br />
immunizations hiStorY NKDA Allergies:<br />
BMI:<br />
Up-to-date according to the schedule established by uNClothEd ( %) WNL)<br />
Appearance phYSiCal Head Circumference:<br />
Nose ExaM ( %)<br />
the Advisory Deferred<br />
Visits Committee to<br />
- Reason:<br />
other health-care on Immunization providers, Practices facilities: (ACIP) Return<br />
Heart Abnormal to office:<br />
Rate: (Mark all that apply Respiratory and describe): Rate:<br />
Abdomen<br />
Check<br />
Head/fontanels<br />
is a federally Lead mandated questionnaire, component risk identified: of the checkup. Y The N<br />
Additional: Appearance the box if all items<br />
Mouth/throat<br />
Nose in the table are within<br />
Genitalia<br />
Abdomen normal limits<br />
Current Parental See new Medications:<br />
concerns/changes/stressors patient history form in family or home: Temperature: See growth graph<br />
Skin Teeth Extremities<br />
(WNL).<br />
form allows Parental iNtErVal TB space questionnaire*, concerns/changes/stressors for<br />
hiStorY:<br />
documenting risk identified: up-to-date in family or Y deferred or N home: Weight: Teeth Eyes Normal Head/fontanels # (Mark here ( if Neurological Mouth/throat all %) items Height: are WNL) Back Genitalia ( %)<br />
immunizations, Ordered Psychosocial/Behavioral *TB today: skin<br />
including<br />
test if indicated<br />
rationale for deferral.<br />
PPD placed<br />
Skin Teeth Extremities<br />
Visits<br />
NKDA<br />
other health-care<br />
Allergies: Health providers, Issues: facilities: Y N<br />
Abnormal BMI: Ears (Mark ( all that %) Heart/pulses apply and describe): Rate: Musculoskeletal<br />
Findings: (See back for forms)<br />
Blood Audiometric Eyes Screening: Neurological Back<br />
Appearance Pressure: / Lungs Nose Respiratory Abdomen Hips Rate:<br />
Each form Psychosocial/Behavioral also includes the age-appropriate Health Issues: vaccine Y N<br />
R Ears 1000Hz 2000HZ Heart/pulses 4000HZ Musculoskeletal<br />
Findings:<br />
Check<br />
Abnormal Temperature Head/fontanels only the<br />
findings: (optional):<br />
box adjacent Mouth/throat<br />
choices. Check the box for any vaccines given the day of the L 1000Hz 2000HZ Lungs to the body part Genitalia<br />
Parental 4000HZ Hips with the<br />
Current Medications:<br />
concerns/changes/stressors in family or home:<br />
Signature/title TB questionnaire*, risk identified: Y N<br />
Signature/title abnormal Skin<br />
checkup. DEVELOPMENT:<br />
Abnormal Normal result (Mark findings: here if Teeth all items are WNL) Extremities<br />
*TB The skin separate test if indicated immunization PPD record placed also serves as Eyes Neurological Back<br />
sufficient<br />
Use TB documentation.<br />
questionnaire*, of standardized risk tool: identified: Y P N F<br />
Abnormal Visual Acuity (Mark Screening: all that apply and describe):<br />
Psychosocial/Behavioral (See back for form) Health Issues: Y N<br />
Ears Heart/pulses Musculoskeletal<br />
Findings: *TB Visits ASQ* skin to test other ASQ-SE* if indicated health-care PEDS* providers, PPD Other: placed facilities:<br />
OD Appearance / OS Nose / OU Lungs<br />
Lungs<br />
Hips/<br />
*ASQ, DEVELOPMENT:<br />
(See ASQ-SE, back for PEDS, form) required for use as of 9/1/11<br />
Additional: Head Mouth/throat GI/abdomen<br />
Abnormal findings:<br />
Laboratory<br />
Use of standardized tool: P F<br />
Teeth HEALTH Skin # EDUCATION/ANTICIPATORY<br />
Teeth Extremities<br />
Parental TB DEVELOPMENT:<br />
questionnaire*, Additional:<br />
Laboratory ASQ* concerns/changes/stressors risk identified: Y<br />
services with PEDS* screening for Other in family N or home:<br />
age-appropriate<br />
GUIDANCE Eyes (See back Neck for useful topics) Back<br />
*TB Use NUTRITION*:<br />
skin of standardized test if indicated tool: P PPD F placed<br />
Teeth #<br />
laboratory<br />
Autism<br />
tests<br />
screening<br />
are a federally<br />
if not performed<br />
required component<br />
at 18 months:<br />
of the<br />
P F Subjective Ears Vision Screening: Heart P F Musculoskeletal<br />
Problems: ASQ* (See back<br />
MCHAT* Y<br />
for PEDS* form)<br />
Other N Other<br />
Hearing Selected Checklist health for topics Parents: addressed P in F any<br />
Neurological<br />
of the<br />
checkup. Autism Assessment:<br />
This section screening includes if not performed age-appropriate at 18 months: required P F Subjective<br />
following areas*:<br />
Vision Screening: *ASQ, Psychosocial/Behavioral PEDS, M-CHAT required Health<br />
DEVELOPMENT:<br />
use Issues: as of Y 9/1/11 N<br />
Abnormal (See back findings:<br />
Additional: for form)<br />
laboratory Findings: MCHAT* tests. The form Other allows space for documenting tests Hearing<br />
• School<br />
Checklist<br />
Readiness/Limitations<br />
for Parents: P F<br />
Use of standardized tool: P F<br />
Teeth #<br />
• Nutrition<br />
*ASQ, PEDS, M-CHAT required for use as of 9/1/11<br />
(See<br />
• Personal<br />
back for<br />
Hygiene<br />
form)<br />
HEALTH EDUCATION/ANTICIPATORY • Safety<br />
NUTRITION*:<br />
*See ASQ* Bright Futures PEDS* Nutrition Book Other if needed<br />
Autism screening if not performed at 18 months: P F Subjective GUIDANCE Vision (See Screening: back for useful P F topics)<br />
Problems: TB questionnaire*, Y N risk identified: Y N<br />
HEALTH ASSESSMENT EDUCATION/ANTICIPATORY<br />
Assessment:<br />
NUTRITION*:<br />
IMMUNIZATIONS<br />
MCHAT* Other<br />
Hearing Checklist for Parents: P F<br />
*TB skin test if indicated PPD placed<br />
GUIDANCE (See back for useful topics)<br />
*ASQ, Problems: PEDS, Y M-CHAT N required for use as of 9/1/11<br />
(See Selected back health for form) topics addressed in any of the<br />
(See back for forms)<br />
Assessment: Up-to-date<br />
following areas*:<br />
Selected health topics addressed in any of the<br />
Deferred - Reason:<br />
HEALTH • Communication EDUCATION/ANTICIPATORY<br />
• Discipline<br />
NUTRITION*:<br />
dEVElopMENtal SCrEENiNG:<br />
following Visual Acuity<br />
• Development/Behaviors<br />
areas*: Screening:<br />
GUIDANCE (See back for useful • Nutrition topics)<br />
*See Bright Futures Nutrition Book if needed<br />
Communication<br />
Discipline<br />
12/1/2011Problems: Use of standardized Y N tool: P F<br />
OD / OS / OU /<br />
– 3 – • Social Interaction<br />
• Safety<br />
Assessment: ASQ ASQ:SE PEDS<br />
Subjective Development/Behaviors<br />
Hearing Screening: P<br />
F Nutrition<br />
IMMUNIZATIONS<br />
*See Given Bright today: Futures DTaP Nutrition HAV Book if needed HBV HIB IPV Selected health topics addressed in any of the<br />
• Social Interaction<br />
• Safety<br />
4 YEAR VISIT 2 MONTH VISIT CHILD CHILD HEALTH HEALTH RECOR<br />
T Child CHILD HEALTH hEalth HEALTH CHILD RECORD rECord<br />
RECORD HEALTH RECORD<br />
Dental R<br />
Other R<br />
Return<br />
Signatur
s:<br />
s:<br />
e:<br />
e:<br />
e:<br />
PV<br />
l<br />
-HIB<br />
nza<br />
e:<br />
Abnormal Appearance Skin Visits Lead to (Mark questionnaire, other all health-care that Teeth Nose apply risk and providers, identified: describe): facilities: Genitalia Lungs Y N<br />
Appearance Eyes Head TB questionnaire*, Neurological Mouth/throat Nose risk identified: Abdomen Extremities GI/abdomen Y N<br />
Ears Skin Head/fontanels Psychosocial/Behavioral<br />
*TB skin test if indicated Heart Teeth Mouth/throat Health Issues:<br />
PPD Back Extremities Genitalia placed<br />
Y N<br />
Eyes Skin Findings: Parental (See back concerns/changes/stressors for forms)<br />
Neurological in Musculoskeletal<br />
Back Extremities family or home:<br />
Abnormal Ears Eyes findings:<br />
Heart/pulses Musculoskeletal<br />
Back<br />
Ears Lungs Musculoskeletal<br />
Document Abnormal DEVELOPMENT:<br />
Psychosocial/Behavioral Lead all findings: abnormal questionnaire, findings risk Health in identified: the space Issues: Hips below Y the N<br />
table<br />
or on Abnormal additional Use Findings: TB<br />
of<br />
questionnaire*, findings: standardized paper as needed. risk<br />
tool:<br />
identified: Y<br />
P<br />
N<br />
F<br />
*TB<br />
ASQ*<br />
skin test<br />
ASQ-SE*<br />
if indicated<br />
PEDS*<br />
PPD<br />
Other:<br />
placed<br />
Additional: *ASQ,<br />
(See<br />
ASQ-SE,<br />
back for<br />
PEDS,<br />
forms)<br />
required for use as of 9/1/11<br />
Teeth Lead # questionnaire, risk identified: Y N<br />
The form TB contains questionnaire*, space for risk additional identified: documentation. Y N<br />
Visual Additional: DEVELOPMENT:<br />
*TB NUTRITION*:<br />
Acuity skin test Screening: if indicated PPD placed<br />
OD Breasts Additional: Use<br />
Problems: (See / of back standardized /5 Y for Genitalia OS forms) N / tool: /5 OU / P F<br />
Hearing Assessment:<br />
ASQ* Checklist ASQ-SE* for Parents: PEDS* P P F F Other:<br />
Document Subjective (See *ASQ, back the ASQ-SE, Hearing Tanner for form)<br />
PEDS, stages Screening: required on the P for lines F use provided. as of 9/1/11<br />
Subjective<br />
MEDICAID<br />
DEVELOPMENT:<br />
Vision Screening: P P F F<br />
*See Bright ID: Futures Nutrition Book if needed<br />
HEALTH Newborn Use of Hearing EDUCATION/ANTICIPATORY<br />
standardized Screening: tool: P F<br />
GUIDANCE HEALTH PRIMARY Completion CARE GIVER:<br />
NUTRITION*:<br />
ASQ*<br />
IMMUNIZATIONS<br />
EDUCATION/ANTICIPATORY<br />
date: ASQ-SE* (See back / for PEDS* / useful Results: Other: topics)<br />
GUIDANCE PHONE: Problems: *ASQ, ASQ-SE, Y (See PEDS, N back required for useful for topics) as of 9/1/11<br />
Document<br />
INFORMANT:<br />
HEALTH Selected Assessment: Up-to-date the EDUCATION/ANTICIPATORY<br />
health results topics and completion addressed date in any of of the the newborn<br />
hearing following GUIDANCE Selected test Deferred areas*: in health this -(See section. Reason: topics back Results addressed for useful may in be any topics) accessed of the at<br />
https://www.provideraccess.tehdi.com following • School NUTRITION*: areas*: Readiness • Nutrition using a current user<br />
name UNCLOTHED Selected • Development<br />
and<br />
School *See Problems: Bright<br />
password.<br />
Activity health Futures Y<br />
If PHYSICAL topics N Nutrition no user<br />
• addressed Safety Oral Book<br />
name<br />
Health EXAM if needed<br />
or<br />
in<br />
password<br />
any of the<br />
has yet<br />
following • Physical Development<br />
been<br />
See<br />
established, Given<br />
Assessment: areas*: today: Activity<br />
growth graph<br />
contact DTaP • Nutrition<br />
TEHDI HAV at call HBV 512-458-7726 HIB or IPV<br />
512-<br />
• Physical Newborn IMMUNIZATIONS<br />
458-7111<br />
Meningococcal Activity Care<br />
• Safety Parental/Maternal<br />
ext. 2128, or contact<br />
MMR<br />
OZ Systems<br />
Pneumococcal Well-Being<br />
ASSESSMENT<br />
at 866-427-5768<br />
Weight: • Newborn Varicella Transition ( MMR-V •%) Safety Height: HIB-HBV ( DTap-HIB %)<br />
option 2 *See or email: Bright Futures OzHelp@oz-systems.com Nutrition Book if needed to obtain the<br />
BMI: ASSESSMENT<br />
• Nutrional<br />
Up-to-date<br />
DPAP-IPV ( Adequacy DTaP-HB-IPV %) Heart Rate: DTaP-IPV-HIB Influenza<br />
required<br />
Blood<br />
login Deferred<br />
Pressure:<br />
information. - Reason:<br />
IMMUNIZATIONS / Respiratory Rate:<br />
Standardized Temperature: ASSESSMENT<br />
LABORATORY<br />
sensory screenings for vision and hearing are<br />
required Normal Given as Up-to-date part (Mark today: of here the DTaP physical if all items HAV examination, are WNL) HBV including HIB visual IPV<br />
Up-to-date<br />
acuity<br />
Abnormal<br />
and Meningococcal Deferred<br />
Deferred<br />
audiometric<br />
- Reason:<br />
(Mark- all Reason: that<br />
screening MMR<br />
apply and<br />
tests<br />
describe):<br />
at specific Pneumococcal ages.<br />
Visual Appearance acuity Varicella and audiometric MMR-V<br />
Nose screening HIB-HBV tests Lungs performed DTap-HIB<br />
during PLAN/REFERRALS<br />
Head the<br />
DPAP-IPV<br />
Given checkup today: may<br />
DTaP-HB-IPV<br />
DTaP be Mouth/throat documented<br />
DTaP-IPV-HIB<br />
HAV HBV on GI/abdomen the HIB lines<br />
Influenza<br />
IPV<br />
provided Skin Ordered Meningococcal or maintained today: as Teeth supplemental MMR documentation Extremities Pneumococcal in<br />
LABORATORY<br />
the Dental PLAN/REFERRALS<br />
medical Eyes Varicella Referral: record. Y MMR-V Neurological HIB-HBV Back DTap-HIB<br />
Other Ears Referral(s) DPAP-IPV DTaP-HB-IPV Heart DTaP-IPV-HIB Musculoskeletal Influenza<br />
Documentation PLAN/REFERRALS<br />
Up-to-date of test results received from a school vision<br />
Dental<br />
and Abnormal hearing Signature/title Deferred Referral: - Y Reason:<br />
LABORATORY<br />
program findings: or other source may replace the required<br />
Other Referral(s)<br />
visual<br />
Referral(s):<br />
Return acuity to office: or audiometric screening if conducted within<br />
the 12 months Ordered Up-to-date prior today:<br />
the checkup. If testing was completed<br />
elsewhere, Return Deferred to documentation office: - Reason: of the results including the date<br />
and the name of the provider who completed the screening<br />
must be retained in the medical record.<br />
Additional:<br />
Return Signature/title to office:<br />
Ordered today:<br />
The Breasts actual results /5 must Genitalia be maintained /5 in the record.<br />
Signature/title<br />
Subjective Hearing Screening: P F<br />
Signature/title<br />
Subjective Vision Screening: P F<br />
Signature/title<br />
The HEALTH Hearing Checklist EDUCATION/ANTICIPATORY<br />
for Parents is available on the back<br />
of the GUIDANCE checkup form (See for reference back for for useful specific topics) ages as<br />
an optional tool. Subjective sensory screenings through<br />
provider<br />
Selected<br />
observation<br />
health<br />
and/or<br />
topics addressed<br />
informant report<br />
in any<br />
are<br />
of the<br />
documented<br />
following areas*:<br />
by checking the appropriate box when a visual acuity or<br />
• School Activity • Oral Health<br />
audiometric • Development screening test is • not Nutrition required.<br />
• Physical Activity • Safety<br />
ASSESSMENT<br />
12/1/2011<br />
PLAN/REFERRALS<br />
ISIT CHILD DISCHARGE 7 YEAR 3 HEALTH VISIT RECORD TO 5 DAY VISIT CHILD CHILD HEALTH REC R R<br />
– 4 –<br />
Current Additional: Appearance<br />
Medications:<br />
Ears Heart Nose Back Lungs<br />
Teeth Head #<br />
Mouth/throat Abdomen Musculoskeletal<br />
Skin Teeth Genitalia<br />
Visits<br />
Abnormal<br />
Audiometric Eyes<br />
to other<br />
findings:<br />
Screening: health-care<br />
Neurological<br />
providers, facilities:<br />
Extremities<br />
R Ears 1000Hz 2000HZ Heart 4000HZ Back<br />
L 1000Hz 2000HZ 4000HZ Musculoskeletal<br />
Parental<br />
Abnormal<br />
concerns/changes/stressors<br />
findings:<br />
in family or home:<br />
Additional:<br />
Health Teeth<br />
Visual Acuity<br />
# Education/Anticipatory<br />
Screening:<br />
Guidance OD / (See OS back for / useful OU topics) /<br />
Psychosocial/Behavioral Health Issues: Y N<br />
Health Findings:<br />
Audiometric<br />
HEALTH Education<br />
Screening:<br />
EDUCATION/ANTICIPATORY<br />
Including Anticipatory Guidance is a<br />
R Additional: 1000Hz 2000HZ 4000HZ<br />
federally GUIDANCE required component (See back of for the useful checkup.<br />
L Teeth 1000Hz #<br />
2000HZ 4000HZ topics)<br />
Audiometric<br />
Lead questionnaire,<br />
Selected health risk identified: Y N<br />
Visual topics addressed in any of the<br />
R<br />
TB<br />
following 1000Hz<br />
questionnaire*,<br />
Acuity Screening:<br />
risk<br />
areas*: 2000HZ<br />
identified:<br />
4000HZ<br />
Y N<br />
*TB<br />
OD<br />
L • 1000Hz<br />
skin test<br />
/<br />
if indicated<br />
OS /<br />
School Readiness/Limitations<br />
2000HZ<br />
PPD<br />
OU<br />
• 4000HZ<br />
placed<br />
/<br />
Nutrition<br />
(See back for forms)<br />
HEALTH • Personal EDUCATION/ANTICIPATORY<br />
Hygiene<br />
• Safety<br />
GUIDANCE Visual Acuity Screening:<br />
(See back for useful topics)<br />
General<br />
OD ASSESSMENT<br />
categories<br />
/<br />
for<br />
OS<br />
useful<br />
/<br />
health education<br />
OU /<br />
DEVELOPMENT:<br />
topics are<br />
listed Use Selected in of this standardized section, health topics specific tool: addressed age-appropriate in any P of the F topics are<br />
HEALTH EDUCATION/ANTICIPATORY<br />
listed following ASQ* on the areas*: back ASQ-SE* of the form. PEDS* Checking Other:<br />
box indicates that<br />
GUIDANCE (See back for useful topics)<br />
health *ASQ, • education School ASQ-SE, Readiness/Limitations<br />
and PEDS, anticipatory required for guidance use as • of Nutrition 9/1/11 were provided<br />
• Personal Hygiene<br />
• Safety<br />
as required. Selected There health is topics no requirement addressed to in document any of the specific<br />
subject(s) following covered, areas*: although the provider may choose to do<br />
NUTRITION*:<br />
ASSESSMENT<br />
so<br />
Problems:<br />
separately • School<br />
Y<br />
from Readiness/Limitations<br />
N<br />
the form. If there is a • problem Nutrition requiring an<br />
action Assessment: PLAN/REFERRALS<br />
• or Personal outcome, Hygiene documentation may be • Safety made in the space<br />
provided for “Assessment” and “Plan/Referrals.”<br />
Dental ASSESSMENT<br />
Referral: Y<br />
ASSESSMENT<br />
*See Other Bright Referral(s) Futures Nutrition Book if needed<br />
IMMUNIZATIONS<br />
Plan/Referrals<br />
PLAN/REFERRALS<br />
Return to office:<br />
Up-to-date<br />
Dental Deferred Referral: - Reason: Y<br />
Other Referral(s)<br />
Beginning PLAN/REFERRALS<br />
Given today:<br />
at 6 months<br />
DTaP<br />
of age,<br />
HAV<br />
a dental<br />
HBV<br />
referral<br />
HIB<br />
is a required<br />
IPV<br />
component<br />
Dental Referral:<br />
of the checkup<br />
Y<br />
until a dental home is established<br />
Return Meningococcal to office: MMR Pneumococcal<br />
and Signature/title<br />
Other may Varicella Referral(s) be documented MMR-V here HIB-HBV or with supplemental DTap-HIB<br />
information DPAP-IPV maintained DTaP-HB-IPV in the medical DTaP-IPV-HIB record. Influenza<br />
LABORATORY<br />
Return to office:<br />
The time<br />
Up-to-date<br />
that is recommended for a return appointment may<br />
be Signature/title Deferred - Reason:<br />
documented in this section. It does not have to include<br />
the exact date but may include a time frame for the return<br />
checkup Ordered or follow-up today: visit.<br />
Signature/title<br />
Signature/title<br />
The person completing the checkup and the staff assisting<br />
in completion of the checkup sign on the line with their title<br />
included.<br />
4 YEAR 4 YEAR VISIT 4 YEAR VISIT VISIT CHILD CHILD HEALTH CHILD HEALTH REC<br />
Norm<br />
Abnorm<br />
Appe<br />
Head<br />
Skin<br />
Eyes<br />
Ears<br />
Abnorm<br />
Addition<br />
Teeth<br />
Audiom<br />
R 1000<br />
L 1000<br />
Visual A<br />
OD<br />
HEALT<br />
GUIDA<br />
Selec<br />
followin<br />
• Sch<br />
• Per<br />
ASSE<br />
PLAN<br />
Dental R<br />
Other R<br />
Return<br />
Signatur
Back of forms<br />
The back of each form includes age-appropriate Health<br />
Education and Anticipatory Guidance and modified versions of<br />
screening questionnaires.<br />
Typical Developmentally Appropriate Health Education Topics<br />
The health topics included in the list for each age group are<br />
age-specific. No notation is required on the back of the form;<br />
only the check in the box on the front of the form is required.<br />
Reference materials may be found at http://brightfutures.aap.org/.<br />
Hearing Checklist for Parents (optional)<br />
TB Questionnaire<br />
LEAD RISK FACTORS<br />
02/2012<br />
– 5 –