Referrals, referrals, referrals . . . - TOPRA
Referrals, referrals, referrals . . . - TOPRA
Referrals, referrals, referrals . . . - TOPRA

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
focus<br />
Focus<br />
2<br />
The <strong>TOPRA</strong><br />
<strong>Referrals</strong>,<br />
2nd North America<br />
Annual Symposium Meeting Report<br />
<strong>referrals</strong>, <strong>referrals</strong> . . .<br />
Authors<br />
Anne Lenihan (Pfizer Ltd, Tadworth, Surrey, UK), Vincent Wek<br />
(Bluefinch, London, UK), Karen Cox (Pfizer Ltd, Tadworth, Surrey, UK)<br />
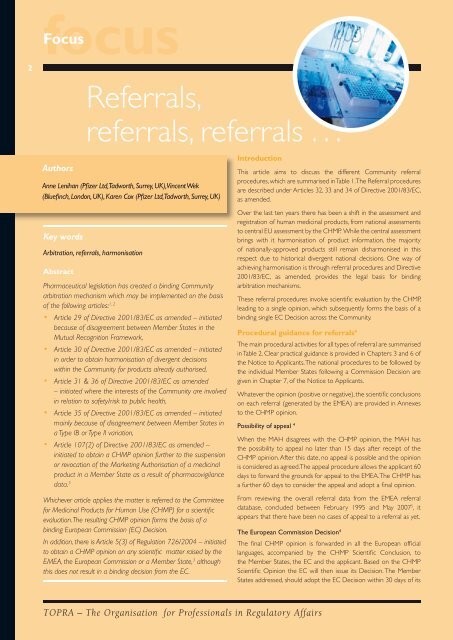
Introduction<br />
This article aims to discuss the different Community referral<br />
procedures, which are summarised in Table 1. The Referral procedures<br />
are described under Articles 32, 33 and 34 of Directive 2001/83/EC,<br />
as amended.<br />
Speakers<br />
to central EU assessment by the CHMP. While the central assessment <br />
Key words<br />
brings with it harmonisation Dombroski, of product and Chris information, Griffett. the majority<br />
Monique Garrett (Octagon Research Solutions, Inc, Pennsylvania, USA) of with nationally-approved products<br />
The meeting<br />
still remain<br />
was co-chaired<br />
disharmonised<br />
by Susanne<br />
in this<br />
Arbitration, <strong>referrals</strong>, harmonisation<br />
contributions from Carlos Langezaal (Sanofi-Aventis, New Jersey, USA), respect due to historical<br />
Dorn,<br />
divergent<br />
Amylin<br />
national<br />
Pharmaceuticals<br />
decisions. One<br />
and<br />
way<br />
Dr<br />
of<br />
Susanne Dorn (Amylin, California, USA), Paolo Biffignandi (VI.REL Pharma, achieving Italy) harmonisation and is through referral procedures and Directive<br />
Abstract<br />
Paolo Biffignandi, VI.REL Pharma S.r.l. Italy<br />
Christopher Bailey (<strong>TOPRA</strong>)<br />
2001/83/EC, as amended, provides the legal basis for binding<br />
and member of the Board of Directors of<br />
Pharmaceutical legislation has created a binding Community arbitration mechanisms.<br />
<strong>TOPRA</strong>. The usual housekeeping rules were<br />
arbitration mechanism which may be implemented on the basis<br />
These referral procedures mentioned, involve scientific and the evaluation morning by session the CHMP, was<br />
of the following articles: 1, 2<br />
This second <strong>TOPRA</strong> leading North to a America single opinion, started. which subsequently forms the basis of a<br />
Article 29 of Directive 2001/83/EC as amended Symposium, – initiated was well binding attended single EC Decision by across the Community.<br />
Paediatric Regulation:<br />
because of disagreement between Member approximately States in the 40 delegates and speakers<br />
A perspective from the European<br />
from the European<br />
Procedural<br />
Medicines Agency<br />
guidance for <strong>referrals</strong><br />
Mutual Recognition Framework,<br />
4<br />
Medicines Agency<br />
(EMEA), the United States The main of procedural America activities for all types of referral are summarised<br />
Article 30 of Directive 2001/83/EC as amended – initiated<br />
Food and Drug Administration Table 2. (FDA) Clear practical and Dr guidance Natalie is Seigneuret provided in (EMEA) Chapters 3 and 6 of<br />
in order to obtain harmonisation of divergent decisions<br />
various pharmaceutical the companies, Notice to CROs, Applicants. Dr The Seigneuret national procedures spoke to about be followed Paediatric by<br />
within the Community for products already authorised,<br />
etc. The topics for this the symposium individual Member were States Regulations following and supporting a Commission activities Decision occurring are<br />
Article 31 & 36 of Directive 2001/83/EC Paediatric as amended Regulations in<br />
given<br />
the<br />
in<br />
morning<br />
Chapter<br />
and<br />
7, of the at Notice the EMEA. to Applicants. She noted that the objective<br />
– initiated where the interests of the Community Risk Management are involved Plans in Whatever the afternoon, the opinion and (positive of the regulation, or negative), which the scientific came into conclusions force in relation to safety/risk to public health, the scientific portion of on the each day referral was closed (generated January by the 26, EMEA) 2007, was are focused provided on in improving Annexes<br />
Article 35 of Directive 2001/83/EC as amended out with – a initiated round table to discussion the CHMP with opinion. the health of children by increasing the quality,<br />
mainly because of disagreement between presenters Member States and industry representatives. ethical research into medicines for children<br />
Possibility of appeal 4<br />
and increasing the availability of authorised<br />
a Type IB or Type II variation,<br />
Opening remarks<br />
When the MAH disagrees medicines with the for CHMP children, opinion, without the MAH delaying has<br />
Article 107(2) of Directive 2001/83/EC as Dr amended Carlos – Langezaal, the as <strong>TOPRA</strong>’s possibility North to appeal authorisation no later than for 15 adults. days after Natalie receipt described of the<br />
initiated to obtain a CHMP opinion further America to the suspension Head opened CHMP the 2007 opinion. North After this four date, key no “pillars” appeal of is the possible regulation: and the opinion<br />
or revocation of the Marketing Authorisation America of a medicinal Annual Symposium is considered by welcoming as agreed. The appeal procedure allows the applicant 60<br />
product in a Member State as a result of pharmacovigilance<br />
Paediatric Committee (PDCO) is to be<br />
the delegates and speakers. days to He forward introduced the grounds for appeal to the EMEA. The CHMP has<br />
data. 3<br />
established by July 26, 2007. This committee<br />
<strong>TOPRA</strong> as a global a further organisation 60 days for to consider the appeal and adopt a final opinion.<br />
includes CHMP members, patient, family<br />
regulatory professionals and for those who<br />
Whichever article applies the matter is referred to the Committee From reviewing the overall and healthcare referral data professionals, from the EMEA experts referral from<br />
have an interest in Regulatory Affairs in the<br />
for Medicinal Products for Human Use (CHMP) for a scientific database, concluded between national February competent 1995 authorities and May and EEA. 2007 5 , it<br />
healthcare sector. The current<br />
appears<br />
membership<br />
that there have been no cases of appeal to a referral as yet.<br />
evaluation. The resulting CHMP opinion forms the<br />
is drawn<br />
basis of<br />
from<br />
a<br />
over 50 countries. Effective Paediatric Investigation Plan (PIP) – An<br />
binding European Commission (EC) Decision. regulatory professionals The need European to get Commission the applicant Decisionmust 4 submit a request for PIP<br />
In addition, there is Article 5(3) of Regulation 726/2004 right information – initiated delivered The at final the CHMP right level opinion is at forwarded end of Phase in I all unless the European duly justified.This official<br />
to obtain a CHMP opinion on any scientific matter the raised right by time, the and languages, that’s what accompanied <strong>TOPRA</strong> by milestone the CHMP requires Scientific early Conclusion, dialog and the to<br />
EMEA, the European Commission or a Member provides State, 3 through although its educational the Member programme, States, the EC need and the for applicant. procedures Based for on modifications the CHMP<br />
this does not result in a binding decision from the including EC. symposia like Scientific today. Subsequently, Opinion the EC will are then foreseen issue as its with Decision. amendments. The Member The<br />
Carlos introduced <strong>TOPRA</strong>’s States North addressed, America should adopt PIP the must EC define Decision the within overall 30 strategy days of for its<br />
paediatric development by the applicant.<br />
<strong>TOPRA</strong> – The Organisation for Professionals in Regulatory Affairs<br />
Over the last ten years there has been a shift in the assessment and<br />
registration of human medicinal Team members, products, Susanne from national Dorn, Gillian assessments Ivers-
Focus<br />
3<br />
Table 1: Community Referral Overview 4<br />
Article of<br />
2001/83/EEC<br />
as amended<br />
29<br />
30<br />
31<br />
35<br />
Referral type<br />
“Mutual Recognition<br />
referral”<br />
“Divergent decision<br />
referral”<br />
“Community interest<br />
referral”<br />
Who may start<br />
referral?<br />
MS concerned<br />
by MRP<br />
Any MS, EC or<br />
MAH<br />
Any MS, EC or<br />
MAH<br />
Which parties are<br />
concerned?<br />
All MS involved in the<br />
MRP (RMS and CMSs)<br />
All MS where MA<br />
granted, refused,<br />
suspended, withdrawn<br />
All MS (MA granted,<br />
refused, withdrawn)<br />
“Follow up referral” MS or MAH All MS involved in the<br />
MRP (RMS and CMSs)<br />
Can application be withdrawn or<br />
referral stopped?<br />
MAH may withdraw at any time.<br />
However, the CHMP may continue<br />
under an Article 31 procedure<br />
regardless of the MAH withdrawal<br />
MAH may withdraw from all<br />
markets at any time<br />
MAH may withdraw at any time.<br />
However, the CHMP may continue<br />
procedure regardless of the MAH<br />
withdrawal<br />
MAH may withdraw at any time.<br />
However, the CHMP may continue<br />
the procedure regardless of the<br />
MAH withdrawal<br />
36 “Follow up referral” MS or MAH All MS where MA is<br />
authorised<br />
MAH may withdraw at any time.<br />
However, the CHMP may continue<br />
the procedure regardless of the<br />
MAH withdrawal<br />
WAINWRIGHT_<strong>TOPRA</strong>_half:WAINWRIGHT_<strong>TOPRA</strong>_half 27/4/2007 12:00 Page 1<br />
MS = Member State, MAH = Marketing Authorisation Holder, CMSs = Concerned Member States, RMS = Reference Member State, MRP = Mutual Recognition Procedure<br />
We have more<br />
services than<br />
meet the eye...<br />
Our services span most product<br />
types and therapeutic areas:<br />
Regulatory affairs<br />
Pharmaceutical and clinical<br />
consultancy<br />
eCTD<br />
User testing<br />
Pharmacovigilance<br />
Licensing<br />
With our network of local advisors<br />
in all relevant fields both in Europe<br />
and worldwide, the chances are if<br />
we can’t help, no-one can.<br />
To find out how we could help you,<br />
visit our website or contact us by<br />
any of the ways shown.<br />
REGULATORY AFFAIRS & LICENSING CONSULTANTS<br />
Wainwright Associates Limited<br />
Wessex House, Marlow Road<br />
Bourne End, Buckinghamshire SL8 5SP<br />
United Kingdom<br />
Tel: +44 (0)1628 530554<br />
Fax: +44 (0)1628 530559<br />
Email: admin@wainwrightassociates.co.uk<br />
www.wainwrightassociates.co.uk<br />
Regulatory Rapporteur – September Issue 2007
Focus<br />
4<br />
Table 2: Referral – Standard Timetable 4<br />
Day 0 • Notification of a referral to the CHMP<br />
Day 1 • CHMP meeting to discuss and adopt questions to be addressed in the referral<br />
• Appointment of the Rapporteur/(Co) – Rapporteur<br />
Clock stop • For the applicant(s)/Marketing Authorisation Holder(s) to answer the list of questions raised by the CHMP<br />
Clock re-start (day 2) • First CHMP meeting after submission of responses<br />
• Adoption by the CHMP of timetable for the rest of the procedure. (Potential negotiation for response time)<br />
Day 45 • (Co)-Rapporteur(s) prepare(s) assessment reports<br />
Day 55 • Comments from the CHMP members on the (Co)-Rapporteur(s) assessment report(s)<br />
Day 60 • Discussion at the CHMP<br />
• Need to have an oral explanation: (Co)-Rapporteur(s) and EMEA to liaise with the applicant(s)/Marketing<br />
Authorisation Holder(s)<br />
• Applicant(s)/Marketing Authorisation Holder(s) should submit the translations of draft SmPC in all EU<br />
official languages<br />
Clock stop • If necessary, for the preparation and submission of oral explanations<br />
Clock re-start • If necessary, oral explanations<br />
Day 90 • Adoption of the CHMP opinion<br />
notification. The Decision is also transmitted to the Member States<br />
not involved in the procedure for information.<br />
The countries with national licences, if applicable, should take appropriate<br />
measures to harmonise their authorisation and SmPC with the one<br />
approved by the EC. The EC Decision is binding to all addresses.<br />
Overview and discussion of the different <strong>referrals</strong><br />
This section will discuss each of the different referral procedures<br />
separately. Details of all completed <strong>referrals</strong> can be accessed from<br />
the EMEA referral website. 5<br />
Article 29 “Mutual Recognition referral”<br />
Arbitration procedures under Article 29 of Directive 2001/83/<br />
EC, as amended are initiated because of disagreement between<br />
Member States during the Mutual-Recognition Procedure (MRP)<br />
or Decentralised Procedure (DCP). 4 A Member State that cannot<br />
approve an authorisation within a MRP/DCP procedure may, under<br />
Article 29, refer the matter for consideration to the Coordination<br />
Group for Mutual Recognition and Decentralised Procedures –<br />
Human (CMD(h)). 6 The grounds for the referral must be “on the<br />
basis of potential serious risk to public health”. 7<br />
A referral to the CMD(h) was introduced with the aim of creating a<br />
procedure that would prevent the need for arbitration by the CHMP.<br />
Prior to this, issues raised often remained unresolved because the<br />
applicant withdrew the application in the disagreeing Member State.<br />
Now, even if an application is withdrawn, a claim of a serious risk to<br />
public health must be investigated by the CMD(h). 6<br />
If the issues cannot be resolved by the CMD(h) then the matter is<br />
referred for arbitration by the CHMP, which then follows the usual<br />
referral procedure. Member States that are willing to accept the<br />
RMS position can grant a Marketing Authorisation for the product<br />
concerned without prejudice to the outcome of the referral.<br />
Article 30 “Divergent decision referral”<br />
If Member States have adopted divergent decisions concerning the<br />
authorisation of a particular medicinal product or its suspension or<br />
withdrawal from the market, a Member State, or the Commission,<br />
or the Marketing Authorisation Holder may refer the matter to<br />
the CHMP under Article 30 of Directive 2001/83/EC as amended.<br />
The CHMP will then issue an opinion which aims to resolve the<br />
divergences between the national decisions. 4<br />
SmPC harmonisation<br />
The remit for SmPC harmonisation came about following the implementation<br />
of Directive 2001/83/EC, as amended. Article 30(2) of<br />
EU Directive 2001/83/EC as amended, which provides the basis for<br />
SmPC harmonisation, states that “In order to promote harmonisation<br />
of authorisations for medicinal products authorised in the Community,<br />
Member States shall, each year, forward to the coordination group a<br />
list of medicinal products for which a harmonised summary of product<br />
characteristics should be drawn up”. The CMD(h) Sub-group on<br />
Harmonisation of SmPCs has been given the mandate by this article to 8 :<br />
1. Advise Member States in choosing products suitable for harmonisation<br />
by giving examples of criteria to be used.<br />
2. Recommend to CMD which products, suggested by Member<br />
States, should be included in the list of medicinal products for<br />
which a harmonised SmPC should be drawn up<br />
3. Have contact with interested parties, in an appropriate way and<br />
time, to ensure that their views will be considered<br />
<strong>TOPRA</strong> – The Organisation for Professionals in Regulatory Affairs
Focus<br />
5<br />
4. Be a forum for discussions with the EC on which party will make<br />
the referral for which product, the order and timing for <strong>referrals</strong><br />
and the practical arrangements such as a pre-referral meeting<br />
with MAH/EMEA etc.<br />
The criteria for selection of products for SmPC harmonisation was<br />
endorsed by the CMD(h) during its January 2006 meeting and is as<br />
follows 9 :<br />
Significant differences in core parts of the SmPC (Sections 4.1- 4.4)<br />
<br />
<br />
<br />
Exclusivity/patent expiry dates, which are linked to entry of<br />
generic products<br />
Extent of the use of the product<br />
Number of MS where the product is authorised.<br />
Once every year the list of products for SmPC harmonisation drawn<br />
up by the CMD(h), is forwarded to the EU Commission. 10 Before<br />
a referral is triggered under Article 30(2), the list of products for<br />
proposed harmonisation is made publicly available for comments<br />
from interested parties to be taken into account.<br />
Article 31 “Community interest referral”<br />
In specific cases where the interests of the Community are involved,<br />
a Member State, or the Commission, or the Marketing Authorisation<br />
Holder may refer the matter to the CHMP under an Article 31 of<br />
Directive 2001/83/EC as amended, before taking a decision on a request<br />
for a Marketing Authorisation, or on the suspension, or withdrawal of<br />
a Marketing Authorisation or on any other variation to the terms<br />
of a Marketing Authorisation which appears necessary. The CHMP<br />
will then issue an Opinion on the concerns raised in the questions<br />
involving Community interests. The Decision of the Commission must<br />
In the majority of Article 31 cases from the EMEA website this<br />
referral procedure has been used for matters relating to drug safety<br />
issues and sometimes involve all medicinal products belonging to one<br />
therapeutic class. 5<br />
Article 35 “Follow up referral”<br />
Arbitration procedures under Article 35 of Directive 2001/83/<br />
EC, as amended are initiated because of disagreement between<br />
Member States during a Type IB or Type II variation procedure.<br />
Article 35 provides for an Article 5(11), 6(12) or 6(13) referral<br />
under Commission Regulation No 1084/2003. Article 5(11) and<br />
Article 6(13) are for situations where a Type IB or Type II variation,<br />
respectively, is refused and Article 6(12) where a Member State does<br />
not consider it possible to mutually recognise a Type II variation. 4<br />
Article 36 “Follow up referral”<br />
In specific cases where a change/variation, suspension or withdrawal<br />
of a harmonised Marketing Authorisation is necessary for the<br />
protection of public health, a Member State may refer the matter to<br />
the CHMP under Article 36 of Directive 2001/83/EC as amended. 4<br />
Article 5(3) “Scientific matter referral” and Article 107(2) “Pharmacovigilance<br />
referral”<br />
Within this paper Article 5(3) and Article 107(2) procedures will not<br />
be discussed in detail, due to the fact that these referral procedures are<br />
new legislative tools and the experience in 2006 has been very limited.<br />
<strong>Referrals</strong> under Article 5(3) of Regulation 726/2004 are initiated to<br />
obtain a CHMP opinion on any scientific matter raised by the EMEA,<br />
the European Commission or a Member State. 3 It does not result in<br />
a binding decision of the European Commission.<br />
be implemented in all Member States concerned. 4 Regulatory Rapporteur – September Issue 2007<br />
Figure 1: Completed <strong>Referrals</strong> from May 1996 to May 2007 5<br />
20<br />
15<br />
No. of Articles<br />
10<br />
Article 36<br />
Article 35<br />
Article 31<br />
Article 30<br />
Article 29<br />
5<br />
0<br />
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Focus<br />
6<br />
<strong>Referrals</strong> under Article 107(2) under Directive 2001/83/EC as<br />
amended are initiated to obtain a CHMP Opinion further to the<br />
suspension or revocation of the Marketing Authorisation of a medicinal<br />
product in a Member State as a result of pharmacovigilance data. It<br />
is expected that <strong>referrals</strong> relating to pharmacovigilance concerns will<br />
concern therapeutic classes rather than individual products. 3<br />
EMEA Referral database analysis 5<br />
This section provides a summary of Articles 29, 30, 31, 35, and 36 from the<br />
EMEA referral database concluded between May 1996 and May 2007. 5<br />
From the graphical representation (Figure 1) there has been a<br />
substantial increase in <strong>referrals</strong> in 2000, 2002 and again in 2006,<br />
particularly Article 29 and 30 of Directive 2001/83/EC as amended.<br />
The main reasons for the increase in <strong>referrals</strong> include:<br />
• SmPC harmonisation project (2001 – Heads of Agencies, CMD(h))<br />
• Ongoing activities of the Pharmacovigilance Working Party<br />
• Shift of regulatory environment from national to pan-European<br />
• Increased focus on the benefit/risk profile of products.<br />
Further analysis of Articles 29, 30, 31, 35, and 36 <strong>referrals</strong> from the<br />
EMEA referral database was conducted which is shown in Table 3. 5<br />
From reviewing the data the following was observed for each of the<br />
<strong>referrals</strong>:<br />
• Article 29 <strong>Referrals</strong> – a total of 33 completed. A review of the<br />
data showed the median duration was 8 months, the shortest was<br />
6 months, and the longest was 18 months (see Figure 2).<br />
• Article 30 <strong>Referrals</strong> – a total of 24 completed. A review of the<br />
data showed the median duration was 15 months, the shortest<br />
was 8 months and, the longest was 24 months (see Figure 2).<br />
• Article 31 <strong>Referrals</strong> – a total of 22 completed. A review of the<br />
data showed the median duration was 19 months, the shortest<br />
was 7 months and the longest was 37 months (see Figure 2).<br />
• Article 35 <strong>Referrals</strong> – a total of 12 completed. A review of the<br />
data showed the median duration was 13 months, the shortest<br />
was 5 months, and the longest was 19 months (see Figure 2).<br />
• Article 36 <strong>Referrals</strong> – a total of 3 completed. A review of the data<br />
showed the median duration was 11 months, the shortest was 8<br />
months, and the longest was 43 months (see Figure 2).<br />
In summary, the duration for the different types of <strong>referrals</strong> varied<br />
due to the complexities of the issues raised. Overall, the data show<br />
that in 11 years from May 1996 to May 2007 there have been a total<br />
of 94 <strong>referrals</strong> procedures concluded (see Table 3), and that Article<br />
31 and Article 36 <strong>referrals</strong> took longer to resolve followed closely by<br />
Article 30 <strong>referrals</strong>. 5<br />
Table 3: Summary of Completed <strong>Referrals</strong> from May 1996 to May 2007 5<br />
Counts<br />
Year of Completion<br />
Article 29 Article 30 Article 31 Article 35 Article 36 Total<br />
1996 1 4 5<br />
1997 1 1 2<br />
1998 1 1 2<br />
1999 1 1 2<br />
2000 2 1 3 6<br />
2001 1 1<br />
2002 2 5 2 3 12<br />
2003 3 8 2 3 16<br />
2004 4 4 5 3 16<br />
2005 4 1 5 1 11<br />
2006 13 4 1 2 20<br />
2007 1 1<br />
Grand Total 33 24 22 12 3 94<br />
<strong>TOPRA</strong> – The Organisation for Professionals in Regulatory Affairs
Focus<br />
7<br />
Figure 2: Duration of the Different <strong>Referrals</strong> from May 1996 to May 2007 5<br />
45<br />
40<br />
35<br />
30<br />
Months<br />
25<br />
20<br />
Minimum<br />
Median<br />
Maximum<br />
15<br />
10<br />
5<br />
0<br />
Article 29 Article 30 Article 31 Article 35 Article 36<br />
Overall practical aspect for managing a referral<br />
Box 1 highlights some overall practical aspects for managing a referral procedure.<br />
Box 1<br />
Overall practical aspects<br />
<br />
<br />
Develop a good relationship with your designated EMEA<br />
Product Team Leader (PTL) and Administrator. This is<br />
essential and will help the process to go smoothly.<br />
Seek clarity on all the steps in the referral procedure.<br />
Upon initiation of a referral<br />
In certain circumstances, for example Article 30, 31<br />
and 36, Marketing Authorisation Holders (MAHs) can<br />
group together to submit a single response. In these<br />
circumstances the following applies:<br />
Each MAH must provide a signed Letter of<br />
Representation allowing a single contact to act on their<br />
behalf.<br />
The products covered by the referral will be provided in<br />
a list from the EMEA (designated as Annex 1).<br />
A single fee may be payable to the EMEA. 11<br />
During the referral<br />
<br />
<br />
<br />
<br />
It is useful to generate and maintain a chronological<br />
summary of events throughout the procedure.<br />
For older products consider that it may be more challenging<br />
to respond to EMEA questions within the timelines, due to<br />
locating all relevant historical data.<br />
For complex issues there exists an opportunity for<br />
applicants to have an Oral Explanation (OE) with the<br />
CHMP.<br />
Ensure the accuracy of Annex 1 particulars (eg, List of the<br />
Invented Names, pharmaceutical forms, strengths of the<br />
medicinal products, route of administration and Marketing<br />
Authorisation Holders in the Member States), as this is<br />
legally binding following the EC Decision.<br />
Regulatory Rapporteur – September Issue 2007
Focus<br />
8<br />
Box 1 continued<br />
Upon completion of a referral<br />
The decision-making process (from CHMP Opinion to<br />
Commission Decision) is the same as for the Centralised<br />
Procedure.<br />
Be prepared for the translations into all the EU official<br />
languages.<br />
MAHs can liaise with each other to provide a single version of<br />
the translated Annexes to the EMEA.<br />
Once a referral is finalised, consider external communications,<br />
eg, press releases, and updates to promotional materials.<br />
It may be necessary to disseminate a Direct Healthcare<br />
Professional Communication or other educational materials in<br />
accordance with Volume 9A of the Rules Governing Medicinal<br />
Products in the EU.<br />
The EMEA may request MAHs to collaborate on certain<br />
documents to finalise the referral.<br />
After completion of a referral, the MA should enter into<br />
a procedure that allows the MAH to improve and/or<br />
develop the product further in a harmonised manner. These<br />
recommendations are outlined in the MRFG guidance<br />
document on “Recommendations for MRP after finalisation of<br />
an arbitration procedure…” 12 .<br />
Conclusion<br />
automatic referral of Article 29 arbitrations and<br />
continue to increase, due to: 3<br />
With the ever increasing focus on continued positive benefit: risk <br />
profiles of medicinal products, referral procedures provide a<br />
framework to address safety matters in a pan-European way. From<br />
reviewing the EMEA referral database, <strong>referrals</strong> have increased over<br />
the years, especially Article 29 and Article 30. Due to complexities of<br />
the particular referral procedure the referral duration can be as short<br />
as 5 months and as long as 43 months (see Figure 2).<br />
References<br />
In the immediate future <strong>referrals</strong> are here to stay and will probably<br />
continue to increase. The number of Article 29 and 30 <strong>referrals</strong> will<br />
Special Interest<br />
Groups<br />
Are you in the food and feed<br />
additives industry and preparing<br />
for REACH ?<br />
<strong>TOPRA</strong> is aware that regulations of the food<br />
and feed additives industry are becoming more<br />
complex. There has been interest expressed in<br />
creating an email network for <strong>TOPRA</strong> members<br />
working in regulatory affairs in the area, in order to<br />
provide a forum for the discussion and exchange of<br />
information and experiences in this changing field.<br />
If you would be interested in becoming a member<br />
of the network, send your details to:<br />
spin@topra.org<br />
the legislative requirement for the CMD(h) to prepare an annual<br />
list of medicinal products for harmonisation (ie, Article 30s).<br />
It will be interesting to observe whether there will be further<br />
increases in <strong>referrals</strong> as more experienced is gained with Article 5(3)<br />
and Article 107(2).<br />
1. Directive 2001/83/EC of the European Parliament and of the<br />
Council of November 6, 2001 on the Community Code Relating to<br />
Medicinal Product for human use http://www.emea.europa.eu/pdfs/<br />
human/pmf/2001-83-EC.pdf (accessed June 18, 2007).<br />
2. Annual Report of the European Medicines Agency (2006) www.<br />
emea.europa.eu/pdfs/general/direct/emeaar/EMEA_Annual_Report_<br />
2006_full.pdf (accessed June 18, 2007).<br />
3. EMEA Work Programme 2007 – http://www.emea.europa.eu/htms/<br />
general/direct/wp.htm (accessed June 18, 2007).<br />
4. Notice to Applicants http://ec.europa.eu/enterprise/<br />
pharmacWalcot56euticals/eudralex/homev2.htm (accessed June 18,<br />
2007).<br />
5. EMEA Referral website – extensive list of referred applications to<br />
date http://www.emea.europa.eu/htms/human/referral/referral.htm<br />
(accessed June 18, 2007).<br />
6. CMD(h) <strong>Referrals</strong> – http://www.hma.eu/26.html (accessed June 18,<br />
2007).<br />
7. Guideline on the definition of a potential serious risk to public health<br />
in the context of Article 29(1) and (2) of Directive 2001/83/EC<br />
– March 2006 http://eurlex.europa.eu/LexUriServ/site/en/oj/2006/<br />
c_133/c_13320060608en00050007.pdf (accessed June 18, 2007).<br />
8. SmPC Harmonisation mandate htp://www.hma.eu/uploads/media/<br />
SG_SPC_harmon_mandate.pdf (accessed June 18, 2007).<br />
9. CMD (h) Sub-Group on Harmonisation of SmPCs http://www.hma.<br />
eu/uploads/media/SG_SPC_harmo_selection_criteria.pdf (accessed<br />
June 18, 2007).<br />
10. CMD(h) List of Products for SmPC Harmonisation 2006 http://hma.<br />
eu/uploads/media/CMD_product_list_SPC_Harmonisation_2006.pdf<br />
(accessed June 18, 2007).<br />
11. Explanatory Note on Fees Payable to the EMEA http://www.emea.<br />
europa.eu/htms/human/presub/39418705en.pdf (accessed June 18,<br />
2007).<br />
12. Recommendation for Mutual Recognition Procedure after finalisation<br />
of an arbitration procedure with a Positive Opinion by the CPMP<br />
and a Positive Decision by the EU Commission http://www.hma.<br />
eu/uploads/media/rec_arbitration.pdf (accessed June 18, 2007).<br />
<strong>TOPRA</strong> – The Organisation for Professionals in Regulatory Affairs