Spatial hemineglect in humans - Cisi
Spatial hemineglect in humans - Cisi
Spatial hemineglect in humans - Cisi

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
G. Kerkho€ / Progress <strong>in</strong> Neurobiology 63 (2001) 1±27 3<br />
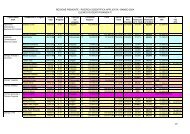
Table 1<br />
Summary of sensory, motor and representational neglect phenomena occurr<strong>in</strong>g after unilateral lesions <strong>in</strong> <strong>humans</strong><br />
Type of neglect<br />
Visual<br />
Auditory<br />
Somatosensory<br />
Olfactory<br />
Motor<br />
Representational<br />
De®nition and typical behaviour<br />
Patient searches for stimuli with eye- and head-movements preferentially <strong>in</strong> the ipsilesional hemispace. Omission of<br />
contralesional stimuli dur<strong>in</strong>g read<strong>in</strong>g, writ<strong>in</strong>g, draw<strong>in</strong>g of geometric stimuli, bisect<strong>in</strong>g horizontal l<strong>in</strong>es, or eat<strong>in</strong>g<br />
from a plate. Ipsilesional deviation of the perceived subjective straight ahead.<br />
Patient does not react to sound/speech stimuli from the contralateral hemispace. He/she may turn to the<br />
ipsilesional side when addressed from the contralesional. When several speakers are present the patient responds<br />
preferentially to the most ipsilesional one, irrespective of who has spoken. Ipsilesional deviation of the perceived<br />
auditory midl<strong>in</strong>e position <strong>in</strong> front space.<br />
Ignor<strong>in</strong>g of tactile stimulation (i.e. touch) or pa<strong>in</strong>ful stimuli (cold/hot stimuli, jammed ®ngers <strong>in</strong> wheel or spokes of<br />
the wheelchair) on the contralesional body half. Mislocalization of tactile stimuli <strong>in</strong> this part. Subjective shift of<br />
own body-midl<strong>in</strong>e (i.e. position of the sp<strong>in</strong>e) to the ipsilesional side.<br />
Ignor<strong>in</strong>g smells delivered to one nostril. Rarely observed <strong>in</strong> daily life s<strong>in</strong>ce stimuli are easily detected with the other<br />
nostril.<br />
Reduced use of contralesional arm/leg which is not completely attributable to a sensorimotor loss. Reduced arm<br />
sway dur<strong>in</strong>g walk<strong>in</strong>g; reduced use of contralesional arm dur<strong>in</strong>g bimanual activities (i.e. eat<strong>in</strong>g, carry<strong>in</strong>g loads);<br />
dragg<strong>in</strong>g beh<strong>in</strong>d the contralesional leg/foot dur<strong>in</strong>g walk<strong>in</strong>g.<br />
Patient describes few items located <strong>in</strong> the contralesional part of an imag<strong>in</strong>ed scene (i.e. a famous city place, the<br />
own liv<strong>in</strong>g room or house), but describes much more items when describ<strong>in</strong>g the same scene from a di€erent<br />
perspective (1808 rotated).<br />
lesioned patients 1 (Stone et al., 1991) when tested immediately<br />
(with<strong>in</strong> 7 days) after lesion onset. The absolute<br />
percentage of neglect depends critically on the<br />
criterion or test used but the asymmetry <strong>in</strong> the occurrence<br />
of contralesional neglect has been found across<br />
di€erent samples and methods (Schenkenberg et al.,<br />
1980). Recovery is considerably quicker and more<br />
complete <strong>in</strong> neglect after left-hemisphere lesions as<br />
opposed to right-hemisphere lesions (Stone et al.,<br />
1991). Thus, there is a clear hemispheric asymmetry<br />
show<strong>in</strong>g that neglect is more frequent, more severe and<br />
more permanent follow<strong>in</strong>g right-hemispheric lesions.<br />
However, transient rightsided neglect after left unilateral<br />
lesions occurs <strong>in</strong> some cases (Welman, 1969; Peru<br />
and P<strong>in</strong>na, 1997; Kerkho€ and Zoelch, 1998). More<br />
long-last<strong>in</strong>g rightsided neglect occurs <strong>in</strong> patients with<br />
bilateral cerebral lesions (We<strong>in</strong>traub et al., 1996).<br />
2.2. Mechanisms of recovery<br />
1 S<strong>in</strong>ce leftsided neglect after right cerebral lesions is the most frequent<br />
type of neglect the term ``neglect'' <strong>in</strong> this review refers always<br />
to leftsided neglect <strong>in</strong> <strong>humans</strong> if not <strong>in</strong>dicated otherwise. Of course,<br />
this does not exclude the fact that rightsided neglect after uni- or bilateral<br />
lesions may occur (more rarely) as well.<br />
Recovery from the most obvious signs of neglect<br />
(i.e. the tendency to orient to the ipsilesional side and<br />
the lack of visual exploration <strong>in</strong> the contralesional<br />
hemispace) has been noted <strong>in</strong> the majority of patients<br />
with<strong>in</strong> the ®rst 6 months (Lawson, 1962; Hier et al.,<br />
1983). In the rema<strong>in</strong><strong>in</strong>g 25% neglect may persist for<br />
up to 12 years (Zarit and Kahn, 1974) and performance<br />
<strong>in</strong> tasks which are sensitive to neglect may decl<strong>in</strong>e<br />
aga<strong>in</strong> after cessation of apparently successful rehabilitation<br />
treatment <strong>in</strong> the cl<strong>in</strong>ic (Paolucci et al., 1998;<br />
Hier et al., 1983). Recovery from neglect is more prom<strong>in</strong>ent<br />
after left compared with right-sided cerebral<br />
lesions (Stone et al., 1991). Furthermore, recovery<br />
from ``frontal'' neglect is more rapid and more complete<br />
<strong>in</strong> <strong>humans</strong> than from the classical ``parietal''<br />
neglect syndrome (Matt<strong>in</strong>gley et al., 1994a). Substantial<br />
recovery is less likely after large lesions and <strong>in</strong><br />
those patients with di€use bra<strong>in</strong> atrophy <strong>in</strong> addition to<br />
the focal right hemispheric lesion (Lev<strong>in</strong>e et al., 1986)<br />
Little is known about the mechanisms guid<strong>in</strong>g spontaneous<br />
recovery and/or those enabl<strong>in</strong>g treatmentguided<br />
improvements dur<strong>in</strong>g rehabilitation. Pantano et<br />
al. (1992) reported a concomitant <strong>in</strong>crease <strong>in</strong> regional<br />
cerebral blood ¯ow (rCBF) <strong>in</strong> the posterior areas of<br />
the damaged right hemisphere and the anterior areas<br />
of the <strong>in</strong>tact, left hemisphere probably <strong>in</strong>clud<strong>in</strong>g the<br />
frontal eye ®elds after a speci®c neglect treatment <strong>in</strong><br />
their patients. Only the left frontal activation, <strong>in</strong> the<br />
region of the frontal eye ®elds, covaried with improved<br />
visual scann<strong>in</strong>g behavior after treatment. The authors<br />
concluded that the left (<strong>in</strong>tact) frontal eye ®elds are<br />
crucial for recovery of visual scann<strong>in</strong>g <strong>in</strong> neglect. In a<br />
later PET study with three neglect patients, this ®nd<strong>in</strong>g<br />
was not uniformly replicated (Pizzamiglio et al., 1998).<br />
In this study, behavioral recovery seemed to covary<br />
with improved blood ¯ow <strong>in</strong> surviv<strong>in</strong>g areas of the<br />
lesioned hemisphere.<br />
Similar results have been obta<strong>in</strong>ed <strong>in</strong> primate studies<br />
where neglect was <strong>in</strong>duced by lesion<strong>in</strong>g the frontal<br />
polysensory association cortex. Metabolic mapp<strong>in</strong>g for<br />
local glucose utilization (2-DG) showed a widespread<br />
reduction of glucose <strong>in</strong> ipsilesional striatal and partially<br />
thalamic nuclei connected with the frontal lobe<br />
whereas no reductions were found <strong>in</strong> cortical areas