All Counties - Community Care Behavioral Health
All Counties - Community Care Behavioral Health
All Counties - Community Care Behavioral Health

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
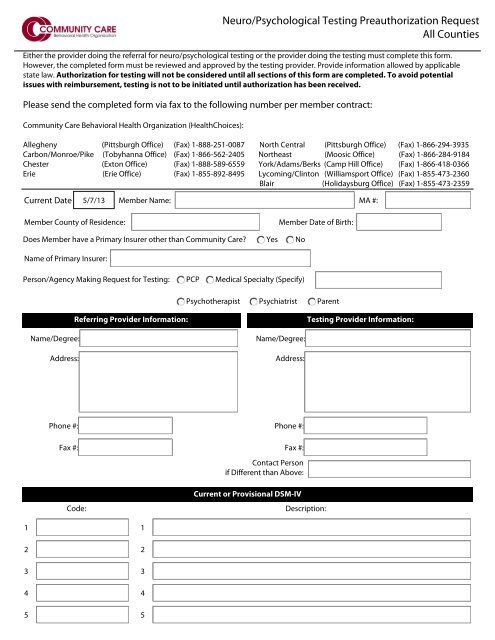
Neuro/Psychological Testing Preauthorization Request<br />
<strong>All</strong> <strong>Counties</strong><br />
Either the provider doing the referral for neuro/psychological testing or the provider doing the testing must complete this form.<br />
However, the completed form must be reviewed and approved by the testing provider. Provide information allowed by applicable<br />
state law. Authorization for testing will not be considered until all sections of this form are completed. To avoid potential<br />
issues with reimbursement, testing is not to be initiated until authorization has been received.<br />
Please send the completed form via fax to the following number per member contract:<br />
<strong>Community</strong> <strong>Care</strong> <strong>Behavioral</strong> <strong>Health</strong> Organization (<strong>Health</strong>Choices):<br />
<strong>All</strong>egheny (Pittsburgh Office) (Fax) 1-888-251-0087 North Central (Pittsburgh Office) (Fax) 1-866-294-3935<br />
Carbon/Monroe/Pike (Tobyhanna Office) (Fax) 1-866-562-2405 Northeast (Moosic Office) (Fax) 1-866-284-9184<br />
Chester (Exton Office) (Fax) 1-888-589-6559 York/Adams/Berks (Camp Hill Office) (Fax) 1-866-418-0366<br />
Erie (Erie Office) (Fax) 1-855-892-8495 Lycoming/Clinton (Williamsport Office) (Fax) 1-855-473-2360<br />
Blair (Holidaysburg Office) (Fax) 1-855-473-2359<br />
Current Date Member Name: MA #:<br />
Member County of Residence:<br />
Member Date of Birth:<br />
Does Member have a Primary Insurer other than <strong>Community</strong> <strong>Care</strong>? Yes No<br />
Name of Primary Insurer:<br />
Person/Agency Making Request for Testing: PCP Medical Specialty (Specify)<br />
Psychotherapist Psychiatrist Parent<br />
Referring Provider Information:<br />
Testing Provider Information:<br />
Name/Degree:<br />
Address:<br />
Name/Degree:<br />
Address:<br />
Phone #:<br />
Fax #:<br />
Code:<br />
Phone #:<br />
Fax #:<br />
Contact Person<br />
if Different than Above:<br />
Current or Provisional DSM-IV<br />
Description:<br />
1<br />
2<br />
3<br />
4<br />
5<br />
1<br />
2<br />
3<br />
4<br />
5
Page 2 of 2<br />
What information is testing expected to<br />
provide that cannot be determined by a<br />
diagnostic interview, review of<br />
psychological/psychiatric records, or a<br />
second opinion?<br />
How would results of testing affect the<br />
treatment plan?<br />
What are the current symptoms related<br />
to the referral question?<br />
What is the referral question to be<br />
answered by testing?<br />
Medical/Psychological Evaluation:<br />
Has client had a diagnostic interview?<br />
No<br />
Yes<br />
Date of interview:<br />
Previous Psych Testing? No Yes When, Basic Focus,<br />
and Results:<br />
Medications Prescribed?<br />
Anti-anxiety Agents<br />
Anti-Parkinsonian<br />
Anti-convulsants<br />
Anti-psychotic<br />
Agents<br />
Anti-depressants<br />
Sedatives/<br />
Hypnotics<br />
Anti-manic<br />
Agents<br />
NONE<br />
Other:<br />
Is member currently attending school? No Yes If Yes, where?<br />
Is member currently abusing any substance? No Yes If Yes, Elaborate:<br />
Requested Testing:<br />
Psychological Testing<br />
(Children/Adolescents) 5 Hours<br />
Psychological Testing<br />
Neuropsychological Testing<br />
(Children/Adolescents) 7 Hours<br />
Neuropsychological Testing<br />
Date to be Administered:<br />
Number of Hours Requested:<br />
Names and Types of Tests: