Pulse Oximetry - Department of Critical Care Medicine
Pulse Oximetry - Department of Critical Care Medicine
Pulse Oximetry - Department of Critical Care Medicine

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
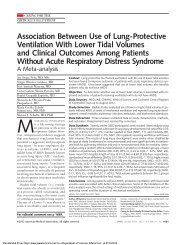
T h e n e w e ngl a nd j o u r na l o f m e dic i n e<br />
videos in clinical medicine<br />
<strong>Pulse</strong> <strong>Oximetry</strong><br />
Rafael Ortega, M.D., Christopher J. Hansen, M.A., Kelly Elterman, M.D.,<br />
and Albert Woo, M.D.<br />
Overview<br />
<strong>Pulse</strong> oximetry has become the standard <strong>of</strong> care in operating rooms, intensive care<br />
units (ICUs), and hospital wards in the United States and many other nations. 1<br />
Before pulse oximetry was available, physicians relied on invasive procedures, such<br />
as arterial puncture for blood gas analysis, to identify the presence <strong>of</strong> hypoxemia.<br />
Unlike arterial blood gas analysis, pulse oximetry allows for noninvasive and continuous<br />
monitoring <strong>of</strong> arterial blood oxygen saturation. Although the pulse oximeter<br />
is easy to use, the clinician must understand the principles <strong>of</strong> pulse oximetry<br />
and must know how the equipment works in order to interpret the information it<br />
provides.<br />
From the <strong>Department</strong> <strong>of</strong> Anesthesiology,<br />
Boston Medical Center, Boston University<br />
School <strong>of</strong> <strong>Medicine</strong>, Boston. Address reprint<br />
requests to Dr. Ortega at the <strong>Department</strong><br />
<strong>of</strong> Anesthesiology, Boston Medical<br />
Center, Boston University School <strong>of</strong> <strong>Medicine</strong>,<br />
88 E. Newton St., Boston, MA, 02118,<br />
or at rortega@bu.edu.<br />
N Engl J Med 2011;364:e33.<br />
Copyright © 2011 Massachusetts Medical Society.<br />
Definitions<br />
Oxygen is present in two forms in the blood: dissolved and bound to hemoglobin.<br />
Hemoglobin can be functional or nonfunctional in terms <strong>of</strong> oxygen binding and<br />
transport. Functional hemoglobin binds and transports oxygen and is present as<br />
oxyhemoglobin, which is hemoglobin that contains bound oxygen, and deoxyhemoglobin,<br />
which is reduced hemoglobin, without bound oxygen. Nonfunctional<br />
hemoglobin is unable to bind or transport oxygen and is present as carboxyhemoglobin<br />
and methemoglobin. Carboxyhemoglobin is hemoglobin bound to carbon<br />
monoxide. Methemoglobin is hemoglobin that contains ferric iron, Fe 3+ , an oxidized<br />
form <strong>of</strong> the oxygen-carrying ferrous iron, Fe 2+ .<br />
The partial pressure <strong>of</strong> oxygen dissolved in arterial blood is termed PaO 2 . The<br />
percent saturation <strong>of</strong> oxygen bound to hemoglobin in arterial blood is termed<br />
SaO 2 . When measured by a pulse oximeter, this value is called SpO 2 .<br />
Indications<br />
<strong>Pulse</strong> oximetry is indicated in all clinical settings in which hypoxemia may occur,<br />
such as operating rooms, ICUs, postanesthesia care units, emergency departments<br />
and ambulances, endoscopy suites, sleep laboratories, cardiac catheterization laboratories,<br />
delivery suites, and wards. The use <strong>of</strong> pulse oximetry in these settings may<br />
reduce the need for arterial blood gas analyses and may allow titration <strong>of</strong> the fraction<br />
<strong>of</strong> inspired oxygen (FiO 2 ) in patients requiring oxygen or mechanical ventilation.<br />
<strong>Pulse</strong> oximetry can also be used to screen for cardiopulmonary disease.<br />
Contraindications<br />
There are no contraindications to pulse oximetry. It is generally safe to use in<br />
monitoring all patients.<br />
Principles <strong>of</strong> Operation<br />
<strong>Pulse</strong> oximeters consist <strong>of</strong> a peripheral probe and a microprocessor unit. Traditionally,<br />
the peripheral probe contains a photodetector and two light-emitting diodes.<br />
n engl j med 364;16 nejm.org april 21, 2011<br />
The New England Journal <strong>of</strong> <strong>Medicine</strong><br />
Downloaded from nejm.org by MICHAEL PINSKY on May 2, 2011. For personal use only. No other uses without permission.<br />
Copyright © 2011 Massachusetts Medical Society. All rights reserved.<br />
e33
The new england journal <strong>of</strong> medicine<br />
Figure 1. Emitted Red Light Reaching<br />
the Photodetector.<br />
Figure 2. <strong>Pulse</strong>-Oximeter Waveform.<br />
Figure 3. <strong>Pulse</strong>-Oximeter Probe<br />
on Earlobe.<br />
The light-emitting diodes each emit light <strong>of</strong> a different wavelength. The light emitted<br />
by the diodes is absorbed by tissues, and the amount <strong>of</strong> absorption is determined<br />
by the photodetector (Fig. 1). Using this information, the microprocessor<br />
determines the concentration <strong>of</strong> oxyhemoglobin and deoxyhemoglobin. It then calculates<br />
the percentage <strong>of</strong> oxyhemoglobin and displays the hemoglobin oxygen saturation<br />
in arterial blood, a waveform corresponding to the pulsatile flow in arterial<br />
vessels, and the heart rate.<br />
<strong>Pulse</strong> oximeters function on the principle that oxygenated hemoglobin and deoxygenated<br />
hemoglobin absorb red and infrared light differently. One light-emitting<br />
diode emits light in the red spectrum, at a wavelength <strong>of</strong> 660 nm, at which the light<br />
absorption <strong>of</strong> deoxyhemoglobin is greater than that <strong>of</strong> oxyhemoglobin. The other<br />
diode emits light in the infrared spectrum, at a wavelength <strong>of</strong> 940 nm, at which<br />
oxyhemoglobin absorbs more light than deoxyhemoglobin. The microprocessor<br />
analyzes the light absorption <strong>of</strong> the tissues at each wavelength to determine the<br />
concentrations <strong>of</strong> oxyhemoglobin and deoxyhemoglobin, respectively. It then divides<br />
the concentration <strong>of</strong> oxyhemoglobin by the concentration <strong>of</strong> both oxyhemoglobin<br />
and deoxyhemoglobin to yield the SpO 2 .<br />
The probe is positioned so that the photodetector and light-emitting diodes face<br />
each other, with layers <strong>of</strong> tissue between them. The photodiodes turn on and <strong>of</strong>f<br />
several hundred times per second to record the light absorption during pulsatile<br />
and nonpulsatile flow. During pulsatile flow, the light absorption <strong>of</strong> arterial blood,<br />
background tissues, and venous blood is detected. During nonpulsatile flow, only<br />
the light absorption <strong>of</strong> background tissues and venous blood is detected. The microprocessing<br />
unit compares the light absorption during both pulsatile and nonpulsatile<br />
flow to isolate the light absorption <strong>of</strong> arterial blood and thus determine<br />
the SpO 2 . 2<br />
Data Interpretation<br />
<strong>Pulse</strong> oximetry provides both qualitative and quantitative data. The qualitative data<br />
are obtained through the sounds emitted by the pulse oximeter; these sounds correlate<br />
with the level <strong>of</strong> oxygen saturation. A higher pitch indicates higher oxygen<br />
saturation, and a lower pitch warns <strong>of</strong> decreasing oxygen saturation. The quantitative<br />
data are obtained through the display <strong>of</strong> a pulsatile waveform that corresponds<br />
to the flow <strong>of</strong> arterial blood (Fig. 2), and the display <strong>of</strong> numbers indicates the SpO 2<br />
and the heart rate.<br />
Proper Use <strong>of</strong> <strong>Pulse</strong> <strong>Oximetry</strong><br />
The ideal site for placement <strong>of</strong> the pulse-oximeter probe is one that is well perfused,<br />
relatively immobile, comfortable for the patient, and easily accessible. The earlobes<br />
(Fig. 3) and the fingers are commonly used sites. However, other sites, including<br />
toes, cheeks, nose, and tongue, may be used in cases <strong>of</strong> low peripheral perfusion.<br />
In adults, the probe can be placed on either side <strong>of</strong> the body. However, in newborns,<br />
in which SpO 2 measurements can aid in the diagnosis <strong>of</strong> congenital cardiac disease,<br />
placement on the right upper arm is preferable. This is because some newborns<br />
may have a patent ductus arteriosus, in which blood flowing to the right<br />
upper arm is least diluted by the shunt and is therefore the most oxygenated. 3<br />
It is important to choose a probe that is the proper size for the patient. If the<br />
probe is not the right size, the light-emitting diodes may not line up correctly with<br />
the photodetector and may produce inaccurate data. For example, a probe that is<br />
too large for a patient’s finger may slip, and the light may not pass completely<br />
across the finger. Venous pulsations may occur if a probe is too small or is placed<br />
too tightly on the finger (Fig. 4). These venous pulsations will produce interfer-<br />
n engl j med 364;16 nejm.org april 21, 2011<br />
The New England Journal <strong>of</strong> <strong>Medicine</strong><br />
Downloaded from nejm.org by MICHAEL PINSKY on May 2, 2011. For personal use only. No other uses without permission.<br />
Copyright © 2011 Massachusetts Medical Society. All rights reserved.
<strong>Pulse</strong> <strong>Oximetry</strong><br />
ence, resulting in a falsely low pulse-oximeter reading. <strong>Pulse</strong>-oximeter probes with<br />
adhesive sensors can minimize motion and may yield more accurate results than<br />
nonadhesive sensors.<br />
Common Problems and Limitations<br />
Although easy to use, the pulse oximeter can produce erroneous data in certain<br />
circumstances. One common problem is the occurrence <strong>of</strong> movement artifacts if<br />
there is movement at the probe placement site. This may interfere with proper function,<br />
and most <strong>of</strong>ten occurs if a patient is shivering, has seizures, or is being transported<br />
by ambulance or helicopter. The waveform <strong>of</strong> the pulse oximeter will be<br />
distorted in such circumstances, and the clinician should recognize that the measurement<br />
displayed is inaccurate. Similarly, it is important to recognize that the<br />
accuracy <strong>of</strong> pulse oximeters deteriorates when the SpO 2 falls below 80%.<br />
A bright light, such as an operating room lamp, may cause light interference,<br />
leading to an erroneous reading. Electromagnetic radiation, such as that emitted<br />
by magnetic resonance imaging (MRI), may also interfere with pulse oximetry.<br />
Only MRI-compatible pulse oximeters should be used for patients undergoing<br />
MRI. If the probe is poorly placed or is the wrong size, light from only one lightemitting<br />
diode may pass through tissues or the light may not reach the detectors,<br />
either <strong>of</strong> which may result in falsely elevated or depressed results. The presence <strong>of</strong><br />
intravascular dyes, such as methylene blue or indigo carmine, may alter the red<br />
and infrared light-absorption properties <strong>of</strong> tissues, which can also lead to an inaccurate<br />
reading. Nail polish that absorbs light at 660 nm or 940 nm may interfere<br />
with the ability <strong>of</strong> the pulse oximeter to interpret the SaO 2 . This problem can be<br />
avoided by removal <strong>of</strong> the nail polish.<br />
Nonfunctional hemoglobin can also result in inaccurate data. At 940 nm, the<br />
light absorption <strong>of</strong> carboxyhemoglobin is minimal and does not affect the SpO 2 .<br />
However, at 660 nm, the light absorption <strong>of</strong> carboxyhemoglobin is similar to that<br />
<strong>of</strong> oxyhemoglobin. The pulse oximeter cannot differentiate between oxyhemoglobin<br />
and carboxyhemoglobin in this instance and may erroneously display a normal<br />
or near-normal measurement <strong>of</strong> SpO 2 when the actual SaO 2 is low.<br />
Methemoglobin absorbs more light than either deoxyhemoglobin or oxidized<br />
hemoglobin at 940 nm, but at 660 nm, the light absorption <strong>of</strong> methemoglobin is<br />
similar to that <strong>of</strong> deoxyhemoglobin. In this instance, the pulse oximeter cannot<br />
differentiate between methemoglobin and deoxyhemoglobin and may incorrectly<br />
perceive an elevated concentration <strong>of</strong> deoxyhemoglobin, which would result in a<br />
falsely low interpretation <strong>of</strong> SaO 2 . Carboxyhemoglobin may cause a falsely high<br />
SpO 2 , whereas methemoglobin may cause a falsely high or falsely low reading<br />
depending on the actual concentration <strong>of</strong> oxyhemoglobin. Newer pulse oximeters<br />
are able to emit light at up to eight different wavelengths, which makes it possible<br />
for the oximeter to measure carboxyhemoglobin and methemoglobin.<br />
The presence <strong>of</strong> peripheral vasoconstriction, hypoperfusion, hypothermia, and<br />
shock may yield an inaccurate measurement <strong>of</strong> SpO 2 . When peripheral blood flow<br />
is decreased, as it is in these conditions, the pulse oximeter may not properly differentiate<br />
between pulsatile and nonpulsatile flow, resulting in an erroneous<br />
measurement. It is important to remember that pulse oximeters function normally<br />
in anemic patients, who have reduced numbers <strong>of</strong> red cells. In an extremely<br />
anemic patient, the oxygen saturation may be normal, but there may be insufficient<br />
hemoglobin to carry an adequate amount <strong>of</strong> oxygen to the tissues. Finally,<br />
pulse oximetry is an indirect method <strong>of</strong> monitoring the patient’s breathing. A<br />
normal SpO 2 may be falsely reassuring in patients receiving supplemental oxygen<br />
because a drop in SpO 2 may occur only after the patient is severely hypercarbic.<br />
Figure 4. Overly Tight Placement<br />
<strong>of</strong> Adhesive <strong>Pulse</strong>-Oximeter Probe.<br />
n engl j med 364;16 nejm.org april 21, 2011<br />
The New England Journal <strong>of</strong> <strong>Medicine</strong><br />
Downloaded from nejm.org by MICHAEL PINSKY on May 2, 2011. For personal use only. No other uses without permission.<br />
Copyright © 2011 Massachusetts Medical Society. All rights reserved.
<strong>Pulse</strong> <strong>Oximetry</strong><br />
References<br />
1. Haynes AB, Weiser TG, Berry WR, et<br />
al. A surgical safety checklist to reduce<br />
morbidity and mortality in a global population.<br />
N Engl J Med 2009;360:491-9.<br />
2. Miller RD, ed. Miller’s anesthesia. 7th<br />
ed. Philadelphia: Churchill Livingstone,<br />
2010.<br />
3. Mahle WT, Newburger JW, Matherne<br />
GP, et al. Role <strong>of</strong> pulse oximetry in examining<br />
newborns for congenital heart disease:<br />
a scientific statement from the<br />
American Heart Association and American<br />
Academy <strong>of</strong> Pediatrics. Circulation<br />
2009;120:447-58.<br />
Copyright © 2011 Massachusetts Medical Society.<br />
New-generation pulse oximeters are manufactured with improved algorithms<br />
that minimize motion-related erroneous data by filtering out body motions. In<br />
addition, because they use multiple wavelengths, these new pulse oximeters are<br />
capable <strong>of</strong> measuring the concentration <strong>of</strong> hemoglobin, carboxyhemoglobin, and<br />
methemoglobin.<br />
Troubleshooting<br />
Artifacts should be the last explanation for changes in critical values. Therefore,<br />
when a clinician obtains a low SpO 2 reading, it is imperative to do a physical assessment<br />
<strong>of</strong> the patient before assuming that the value represents equipment malfunction.<br />
If the patient appears to be clinically stable, consider the possibility <strong>of</strong> a<br />
mechanical malfunction. Make sure the cable connecting the probe to the microprocessor<br />
is intact and is in fact connected to the microprocessor. The cable may<br />
become loose or detached, making it seem as though the pulse oximeter cannot<br />
determine the SaO 2 . If the cable is loose, adjust the connection as necessary. Make<br />
sure that the red light on the inside <strong>of</strong> the probe is evident. If you do not see the red<br />
light, check the power cable. If you can see the red light and have made sure the<br />
cable connecting the probe to the microprocessor is intact, clean the probe and<br />
place it on your own finger to see whether the issue is specific to the patient. If this<br />
is not the case, it is possible that either the probe or the microprocessor is not working<br />
properly. Replace the probe, the microprocessor, or both, as necessary.<br />
Complications<br />
Although the pulse oximeter is generally a safe device, its use still carries some risk<br />
<strong>of</strong> adverse events. Burning or blistering at the placement site may occur if the lightemitting<br />
diode becomes overheated. Ischemic pressure necrosis may result if the<br />
probe is placed too tightly on the patient. Perioperative corneal abrasion may occur<br />
if a patient with a probe on a finger rubs his or her eyes when awakening from<br />
anesthesia and in doing so scrapes the cornea. Prolonged placement <strong>of</strong> a pulseoximeter<br />
probe, which can occur in patients in the ICU, may lead to mechanical<br />
injury, such as finger stiffness, making it difficult for the patient to flex the finger<br />
after the probe has been removed. Although these complications have been documented,<br />
they remain uncommon.<br />
Summary<br />
When used correctly, pulse oximetry is a potentially lifesaving tool. Health care<br />
providers need to be aware <strong>of</strong> the indications, benefits, and disadvantages <strong>of</strong> pulse<br />
oximetry. More important, clinicians must be able to interpret the information<br />
pulse oximetry provides. With proper training and instruction, clinicians will find<br />
pulse oximetry an invaluable monitoring tool.<br />
No potential conflict <strong>of</strong> interest relevant to this article was reported.<br />
Disclosure forms provided by the authors are available with the full text <strong>of</strong> this article at NEJM.org.<br />
n engl j med 364;16 nejm.org april 21, 2011<br />
The New England Journal <strong>of</strong> <strong>Medicine</strong><br />
Downloaded from nejm.org by MICHAEL PINSKY on May 2, 2011. For personal use only. No other uses without permission.<br />
Copyright © 2011 Massachusetts Medical Society. All rights reserved.