HPV Vaccine Consent form - Grey Bruce Health Unit
HPV Vaccine Consent form - Grey Bruce Health Unit
HPV Vaccine Consent form - Grey Bruce Health Unit

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
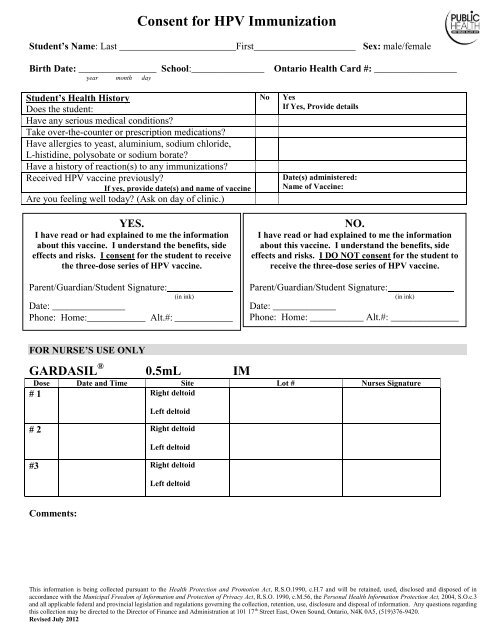
<strong>Consent</strong> for <strong>HPV</strong> Immunization<br />
Student’s Name: Last ________________________First_____________________ Sex: male/female<br />
Birth Date: ________________ School:_______________ Ontario <strong>Health</strong> Card #: _________________<br />
year month day<br />
Student’s <strong>Health</strong> History<br />
Does the student:<br />
Have any serious medical conditions?<br />
Take over-the-counter or prescription medications?<br />
Have allergies to yeast, aluminium, sodium chloride,<br />
L-histidine, polysobate or sodium borate?<br />
Have a history of reaction(s) to any immunizations?<br />
Received <strong>HPV</strong> vaccine previously?<br />
If yes, provide date(s) and name of vaccine<br />
Are you feeling well today? (Ask on day of clinic.)<br />
No<br />
Yes<br />
If Yes, Provide details<br />
Date(s) administered:<br />
Name of <strong>Vaccine</strong>:<br />
YES.<br />
I have read or had explained to me the in<strong>form</strong>ation<br />
about this vaccine. I understand the benefits, side<br />
effects and risks. I consent for the student to receive<br />
the three-dose series of <strong>HPV</strong> vaccine.<br />
Parent/Guardian/Student Signature:<br />
(in ink)<br />
Date: _______________<br />
Phone: Home:____________ Alt.#: ____________<br />
NO.<br />
I have read or had explained to me the in<strong>form</strong>ation<br />
about this vaccine. I understand the benefits, side<br />
effects and risks. I DO NOT consent for the student to<br />
receive the three-dose series of <strong>HPV</strong> vaccine.<br />
Parent/Guardian/Student Signature:<br />
(in ink)<br />
Date: _____________<br />
Phone: Home: ___________ Alt.#: ______________<br />
FOR NURSE’S USE ONLY<br />
GARDASIL ® 0.5mL IM<br />
Dose Date and Time Site Lot # Nurses Signature<br />
# 1 Right deltoid<br />
Left deltoid<br />
# 2 Right deltoid<br />
Left deltoid<br />
#3 Right deltoid<br />
Left deltoid<br />
Comments:<br />
This in<strong>form</strong>ation is being collected pursuant to the <strong>Health</strong> Protection and Promotion Act, R.S.O.1990, c.H.7 and will be retained, used, disclosed and disposed of in<br />
accordance with the Municipal Freedom of In<strong>form</strong>ation and Protection of Privacy Act, R.S.O. 1990, c.M.56, the Personal <strong>Health</strong> In<strong>form</strong>ation Protection Act, 2004, S.O.c.3<br />
and all applicable federal and provincial legislation and regulations governing the collection, retention, use, disclosure and disposal of in<strong>form</strong>ation. Any questions regarding<br />
this collection may be directed to the Director of Finance and Administration at 101 17 th Street East, Owen Sound, Ontario, N4K 0A5, (519)376-9420.<br />
Revised July 2012