Pain - The British Pain Society
Pain - The British Pain Society
Pain - The British Pain Society

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>The</strong> <strong>Pain</strong> <strong>Society</strong><br />
<strong>The</strong> <strong>British</strong> and Irish Chapter of the International<br />
Association for the Study Of <strong>Pain</strong><br />
21 Portland Place<br />
London<br />
W1B 1PY United Kingdom<br />
Telephone (020) 7631 8870<br />
Fax (020) 7323 2015<br />
Email info@painsociety.org<br />
www.painsociety.org<br />
Council Members and Officers 2002-2003<br />
President Dr. Beverly Collett<br />
Immediate Past President<br />
Honorary Secretary<br />
Honorary Treasurer<br />
Honorary Assistant<br />
Secretary<br />
Nursing<br />
Anaesthesia / <strong>Pain</strong><br />
Medicine<br />
Nursing<br />
<strong>Pain</strong> Research<br />
Nursing<br />
Psychology<br />
<strong>Pain</strong> Medicine<br />
National Occupational<br />
<strong>The</strong>rapy <strong>Pain</strong> Association<br />
<strong>The</strong> views of the IASP<br />
Chair, Patient Liaison<br />
Committee<br />
Association of Palliative<br />
Medicine<br />
Chair, Courses and<br />
Meetings Committee<br />
Editor, <strong>The</strong> <strong>Pain</strong> <strong>Society</strong><br />
Newsletter<br />
Association of<br />
Anaesthetists of Great<br />
Britain and Ireland<br />
Chair, Local Organising<br />
Committee ASM 2003<br />
<strong>The</strong> <strong>Pain</strong> <strong>Society</strong> Newsletter is<br />
published quarterly.<br />
Circulation 1650.<br />
<strong>The</strong> editor welcomes<br />
contributions including letters,<br />
short clinical reports and<br />
news of interest to members<br />
including notice of meetings.<br />
Comments on the format of<br />
the Newsletter are welcome.<br />
Dr. Douglas Justins<br />
Dr. Karen Simpson<br />
Dr. George Harrison<br />
Dr. Andrew Vickers<br />
Dr. Eloise Carr<br />
Dr. Kate Grady<br />
Ms. Ruth Day<br />
Dr. Andrew Rice<br />
Dr. Patricia Schofield<br />
Dr. Amanda C de C<br />
Williams<br />
Dr. Cathy Stannard<br />
Mrs. Louise Aylwin<br />
Prof. Sir Michael Bond<br />
Mrs. Jean Gaffin<br />
Dr. Paresh Gajjar<br />
Dr. Paul Watson<br />
Dr. Stephen Ward<br />
Dr. Alastar Chambers<br />
Dr. Chris Spanswick<br />
Material should be sent to:<br />
Dr Stephen P Ward<br />
Editor, <strong>The</strong> <strong>Pain</strong> <strong>Society</strong><br />
Newsletter<br />
<strong>Pain</strong> Management Unit<br />
Brighton and Sussex<br />
University Hospitals NHS Trust<br />
Princess Royal Hospital<br />
Haywards Heath<br />
West Sussex RH16 4EX<br />
Tel 01444 892276<br />
Email drspward@yahoo.co.uk<br />
<strong>The</strong> opinions expressed in the <strong>Pain</strong> <strong>Society</strong> Newsletter do not<br />
necessarily reflect those of the <strong>Pain</strong> <strong>Society</strong> Council.<br />
Editorial<br />
STEPHEN WARD<br />
For the most part, the<br />
‘new-look’ newsletter has<br />
been well received and I<br />
am grateful for your kind<br />
words and<br />
encouragement. Two<br />
criticisms have been<br />
levelled though and I think both deserve<br />
attention. Firstly, I have been informed that<br />
the cover design is ‘too masculine’. Being<br />
the registered bearer of a Y chromosome, I<br />
can’t see it myself – is it the colour scheme?<br />
Not enough pink? Is the typeface too<br />
Neanderthal?<br />
<strong>The</strong> second criticism was of greater<br />
importance and relevance. More than one of<br />
you has noted that the Newsletter has<br />
become somewhat downbeat and selfdepreciating<br />
and that the content tends to<br />
favour articles of a ‘moany’ nature. What<br />
would the lay reader think of us as a <strong>Society</strong><br />
if he were to flick through our publication?<br />
Almost certainly that we are unloved,<br />
undervalued, underfunded, stressed to<br />
breaking point and that we would much<br />
rather write about our bad experiences in<br />
pain management than our good.<br />
Ok….I agree…it’s a fair cop. Whilst I’m as<br />
much in favour of a good old whinge as the<br />
next man the content of the newsletter<br />
needs to change. I’m not saying that we<br />
pretend all is rosy in <strong>Pain</strong>land as patently it<br />
is not, but let’s pat our own backs a bit<br />
more and try to appear, at least outwardly, a<br />
little less downtrodden. Say it with me…’I<br />
work in <strong>Pain</strong> Management and I’m proud!’<br />
Allow me to start the ball rolling and<br />
address some of the popular misconceptions<br />
we and others seem to have about pain<br />
management:<br />
We are not undervalued or unloved – in<br />
fact, whenever I spend time looking at our<br />
waiting list figures I feel positively<br />
overvalued! If you believe for a moment<br />
that your patients don’t value the time and<br />
effort you invest in their wellbeing or that<br />
the local GPs and hospital consultants do<br />
not value your opinion and your expertise<br />
then you might as well give up now.<br />
Are we underfunded as a specialty?<br />
Definitely – but name a specialty that isn’t.<br />
Chronic pain has always been considered a<br />
soft target when it comes to resource<br />
allocation and allowing patients to linger on<br />
the waiting list for years has been the norm.<br />
After all, if a patient has had back pain for<br />
25 years, what’s the rush? All fine and<br />
dandy until Big Al Milburn had the barmy<br />
idea of introducing waiting time<br />
targets…… these days if Mrs Jones isn’t<br />
seen within 17 weeks, a manager<br />
somewhere is shot at dawn. On the face of<br />
it this is madness but it can actually work<br />
very much in our favour. A week or two ago<br />
it was suggested to me that I might like<br />
another couple of pain management<br />
sessions to enable me to meet the 17 week<br />
target. Sorely tempted as I was to see my<br />
manager shot that dawn I jumped at this<br />
chance and I am happy to report that I have<br />
finally joined the ever swelling ranks of the<br />
full time pain specialist. A few years ago it<br />
was virtually impossible to increase pain<br />
sessions without selling your soul to<br />
Beelzebub himself – now they’re throwing<br />
them at us?<br />
Are we stressed as a group? If the ASM is<br />
anything to go by I’d say, outwardly at least,<br />
quite the opposite – have you ever come<br />
across a more relaxed, easy going and fun<br />
loving group? If this is the portrait of a<br />
group under pressure then I’m off to join<br />
the Royal <strong>Society</strong> of Transcendental<br />
Meditants. As individuals, though, we all<br />
suffer stress at some point in our careers<br />
but I suspect this is down to administrative<br />
and managerial foul play and pressure<br />
rather than the nature of the specialty or the<br />
patients we deal with. I find pain<br />
management an immensely rewarding and<br />
fascinating occupation and defy you to find<br />
any specialty more interesting, challenging,<br />
or holistic (Did you hear about the holistic<br />
orthopaedic surgeon? He thought about the<br />
whole bone).<br />
Our specialty leads the field in terms of<br />
scientific expertise and integrity and has<br />
embraced evidence based medicine in its<br />
bosom like no other. We should, quite rightly<br />
feel an immense sense of pride in ourselves<br />
as a group.<br />
By and large the patients we encounter are<br />
pleasant, well informed (apart from the dear<br />
old lady I saw recently who came to clinic<br />
clutching a box of voltarol. ‘What<br />
medication are you taking?’ I asked<br />
‘Voldemort!’ she replied) and grateful for<br />
any help we can give them. Rarely are they<br />
2<br />
THE PAIN SOCIETY NEWSLETTER<br />
SUMMER 2003<br />
EDITORIAL
6<br />
14<br />
THE PAIN SOCIETY NEWSLETTER SUMMER 2003<br />
SARAH BARKER &<br />
AMANDA C DE C WILLIAMS<br />
THE PAIN SOCIETY NEWSLETTER<br />
1-3 Months - 54%<br />
1-3 Months - 74%<br />
Acceptable - 46%<br />
SUMMER 2003<br />
20 THE PAIN SOCIETY NEWSLETTER SUMMER 2003<br />
0-4 Weeks - 23%<br />
0-4 Weeks - 17%<br />
Excellent - 17%<br />
Good - 31%<br />
1-3 Months - 54%<br />
Always - 6%<br />
Rarely - 11%<br />
Sometimes - 11%<br />
4-6 weeks - 11%<br />
2-4 weeks - 54%<br />
NEWS FROM PORTLAND PLACE<br />
0-4 Weeks - 23%<br />
Mostly - 51%<br />
0-2 weeks - 14%<br />
FEATURES<br />
FEATURES<br />
the malingering, miserable,<br />
mad-as-a-badger malcontents<br />
that our colleagues seem to<br />
think they are.<br />
So there we are, a few musings<br />
from me. To be involved in any<br />
way in the treatment and<br />
management of pain is a<br />
privilege. To moan about the<br />
shortcomings of our specialty<br />
incessantly simply fuels the<br />
misconceptions of others that<br />
ours is a dreary, thankless world<br />
– and it simply isn’t.<br />
In this issue, you will see that I<br />
have received a handful of<br />
letters. One of these letters is,<br />
admittedly, a bit of a moan<br />
about private practice but I’ve<br />
let this one go on the grounds<br />
that I tend to agree with him.<br />
Another of the letters is from<br />
Professor Richard Dawkins and<br />
requires a brief explanation.<br />
Richard Dawkins is the Charles<br />
Simonyi Professor of the Public<br />
understanding of Science at<br />
Oxford and is, without doubt<br />
one of our most important<br />
evolutionary biologists. Having<br />
recently read his collection of<br />
selected essays entitled ‘A<br />
Devil's Chaplain’ and another of<br />
his books ‘<strong>The</strong> Selfish Gene’ I<br />
was intrigued by his firmly held<br />
Darwinist belief that genes<br />
survive or fail to survive within<br />
the gene pool of a species by<br />
virtue of their effects upon the<br />
survival of the individual<br />
organism (for example, genes<br />
coding for the various structures<br />
involved in pain pathways are<br />
important to our survival –<br />
acute pain tells us not to move<br />
so that we can heal and not to<br />
do it again!). When we consider<br />
chronic pain however, where is<br />
the evolutionary advantage?<br />
Tissue healing is complete, the<br />
message is useless and the<br />
condition a miserable one. One<br />
would have supposed that this<br />
glitch be ‘ironed’ out over a few<br />
million years but sadly not. Can<br />
it be that genetics plays no part<br />
in chronic pain? Are we more<br />
likely to survive if we are<br />
constantly reminded about an<br />
old injury – even ten years on –<br />
so that we don’t make the<br />
same mistake twice? Are our<br />
pain behaviours passed on like<br />
genes to the next generation so<br />
that they respond in the same<br />
way? Am I just rambling on?<br />
Anyway, he was kind enough to<br />
put his view forward and if any<br />
of you profess any expertise in<br />
this area I’d welcome<br />
comments.<br />
Lastly, thank you all for the<br />
submissions…please keep them<br />
coming.<br />
drspward@yahoo.co.uk<br />
Contents<br />
columns<br />
2 Editorial<br />
4 President’s message<br />
news<br />
6 Glasgow ASM 2003<br />
review<br />
6 <strong>Pain</strong> Meetings for<br />
Health Professionals<br />
8 Pfizer Prize Awards<br />
10 Obituary<br />
11 New Members<br />
13 Results of Glasgow<br />
ASM : session<br />
evaluations<br />
features<br />
14 Psychological<br />
Assessment and<br />
Interventions<br />
15 A Distress Motivation<br />
Axis<br />
18 Angina Pectoris : A<br />
Historical Perspective<br />
20 Nottingham <strong>Pain</strong> Clinic<br />
survey<br />
THE PAIN SOCIETY NEWSLETTER<br />
PAIN MEETINGS FOR<br />
HEALTH PROFESSIONALS<br />
CELLULAR AND MOLECULAR MECHANISMS OF PAIN<br />
a satellite symposium to the International Brain<br />
Research Organization (IBRO)<br />
7-9 July Prague, Czech Republic<br />
Email:palecek@biomed.cas.cz / wdwillis@utmb.edu<br />
Web: http://www.biomed.cas.cz/IBRO-PAIN/<br />
BATH PAIN FORUM - CATASTROPHISING ABOUT<br />
CHRONIC PAIN<br />
29 July, Royal National Hospital for Rheumatic Diseases, Bath<br />
Contact: Dr. Chris Eccleston<br />
Director, <strong>Pain</strong> Management Unit,<br />
University of Bath<br />
Email: pain@bath.ac.uk<br />
PAIN IN EUROPE IV - 4TH CONGRESS OF THE EUROPEAN<br />
FEDERATION OF IASP CHAPTERS (EFIC)<br />
2-6 September, Prague, Czech Republic<br />
Contact: Congress Business Travel<br />
Email: pain2003@cbttravel.cz<br />
Web: www.pain2003.cz<br />
9TH NATIONAL CONFERENCE ON PAIN MANAGEMENT<br />
PROGRAMMES<br />
Organised by the <strong>Pain</strong> Management Special Interest<br />
Group of the <strong>Pain</strong> <strong>Society</strong><br />
11-12 September, John Innes Centre and University of East Anglia<br />
Contact: Elaine Wellingham<br />
Conference Secretariat, Field End House<br />
Bude Close, Nailsea<br />
Bristol BS48 2FQ<br />
Tel/Fax: 01275 853311<br />
Email: Confsec@blueyonder.co.uk<br />
THE FUTURE OF PAIN THERAPUTICS 2003<br />
15-16 September 2003, London<br />
Email: sara.peerun@visiongain.com<br />
http://www.visiongain.com/futurepaindrugs.html<br />
PROVING OUR WORTH!<br />
Specialist Nurses & Nurse Consultants Conference<br />
25 September, Post Graduate Medical Centre, Worthing Hospital,<br />
West Sussex<br />
THE PAIN RELIEF FOUNDATION 4TH ANNUAL LECTURE<br />
2003<br />
<strong>Pain</strong> & Central Nervous System Reorganisation”<br />
Friday,17th October at 7:00 pm<br />
<strong>The</strong> <strong>Pain</strong> Research Institute, Clinical Sciences Centre, University<br />
Hospital Aintree, Liverpool<br />
Professor Troels Jensen, Danish <strong>Pain</strong> Research Centre, University of<br />
Åarhus, Denmark<br />
AN UNRECOGNISED PAIN CHALLENGE<br />
a one-day conference on Joint Hypermobility<br />
Syndrome<br />
21 October 2003, 9.30 - 4.40, Postgraduate Centre, Gassiot House,<br />
St Thomas' Hospital<br />
Psychological Asessment<br />
and Interventions<br />
Having a converted cupboard<br />
for an office makes<br />
psychological consultation at<br />
our hospital a cosy affair.<br />
Despite this, a patient’s first<br />
appointment with the clinical<br />
psychologist can seem scary,<br />
associated with psychiatric<br />
labels and ‘all in the mind’<br />
statements, which mark the end<br />
of the pain being taken<br />
seriously by doctors.<br />
Psychological assessment is a<br />
real deterrent for some who<br />
don’t attend the initial meeting.<br />
But there is no avoiding this<br />
meeting for the patient wanting<br />
a spinal cord stimulator or a<br />
peripheral nerve stimulator:<br />
psychological assessment is<br />
mandatory. Many patients<br />
spend the first minutes<br />
emphasising their sanity, the<br />
reality of their pain, and their<br />
entitlement to neuromodulation<br />
to make life worth living again.<br />
<strong>The</strong> aversive and chronic nature<br />
of patients’ pain makes the<br />
hope of a cure alluring. So what<br />
does the assessment consist of,<br />
and is it really essential?<br />
Nottingham <strong>Pain</strong> Clinic survey<br />
Although it is widely<br />
acknowledged in pain field that<br />
pain is a psychological<br />
experience as well as a physical<br />
one, the relationship between<br />
pain and psychological factors<br />
remains the subject of<br />
differences and debate. It would<br />
be encouraging to think that<br />
dualistic models are losing their<br />
hold, and that the attribution of<br />
pain in some patients to<br />
psychogenic factors is<br />
understood as an hypothesis<br />
not a finding, but this way of<br />
thinking still leads to<br />
stigmatisation and<br />
discrimination in many areas of<br />
health care. Although<br />
professionals working in the<br />
field of pain hopefully now have<br />
a broader perspective,<br />
misunderstandings can still<br />
occur about the role of<br />
psychology and how it can best<br />
be integrated with medical<br />
treatments.<br />
First: what requests can’t<br />
psychological assessment<br />
satisfy? It can’t establish the<br />
relative contributions of organic<br />
and psychological factors (nor<br />
can any other method, as the<br />
underlying model is erroneous),<br />
What do GPs’ want from the pain<br />
clinic and do we provide it?<br />
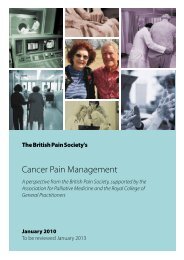
<strong>The</strong> pain department at City Hospital provides a one-day series of<br />
lectures and practical workshops for local GPs.<br />
49 GP’s attended the pain day and 35 returned completed the<br />
questionnaire. <strong>The</strong> response rate was 71%.<br />
nor can it establish ‘cause and<br />
effect’ relationships between<br />
psychological problems and<br />
pain (Doleys, 2000). <strong>The</strong> other<br />
purposes for which assessment<br />
is requested is to exclude<br />
patients with gross mental<br />
health problems, which is<br />
reasonable although we do not<br />
know that they would not<br />
benefit from neuromodulatory<br />
methods; and to improve<br />
outcomes in by identifying<br />
predictors of poor outcome (e.g.<br />
North et al, 1996, Nelson et al,<br />
1996). Suggested candidates for<br />
this include ‘somatisation<br />
disorder’, ‘major uncontrolled<br />
depression/anxiety’, ‘severe<br />
sleep disturbances’, ‘serious<br />
drug or alcohol problems’ and<br />
‘lack of social support’; other<br />
factors which the psychologist is<br />
advised to consider include ‘<br />
history of abuse or other<br />
dysfunction’, ‘unusual pain<br />
ratings’, ‘certain personality<br />
disorders’, ‘unresolved<br />
compensation’ and ‘lack of<br />
support from spouse’ (Olsen,<br />
1996). As you can see from this<br />
list, virtually every patient will<br />
present one or more of these<br />
‘warning’ factors.<br />
While the search for predictors<br />
of outcome seems at first a<br />
reasonable scientific pursuit, it<br />
does not stand up to scrutiny.<br />
<strong>The</strong> only way to discover such<br />
SUMMER 2003<br />
Glasgow ASM 2003 :<br />
Overview<br />
Breakdown of delegates<br />
<strong>The</strong>re were a total number of<br />
1,066 Delegates registered at<br />
the Meeting; an increase of 264<br />
from the 2002 Meeting in<br />
Bournemouth. 50 were<br />
Anaesthetic Research Delegates.<br />
Of the 1066, 70% were<br />
members of the <strong>Society</strong>.<br />
<strong>The</strong> specialty of the delegates<br />
continues to mirror the<br />
membership of the <strong>Society</strong>, with<br />
anaesthetists making up the<br />
largest group of delegates,<br />
followed by nurses,<br />
psychologists, physiotherapists,<br />
occupational therapists and<br />
general practitioners.<br />
Venue<br />
<strong>The</strong> Glasgow Scottish Exhibition<br />
+ Conference Centre was an<br />
excellent venue for this year’s<br />
ASM and perfectly suited the<br />
<strong>Society</strong>’s needs in terms of<br />
quality of plenary hall, number<br />
of break-out rooms and size of<br />
exhibition area. <strong>The</strong> support<br />
staff was excellent and the<br />
additional facilities at the<br />
Centre i.e. café bar, restaurant<br />
and business desk all added to<br />
the success of the meeting.<br />
Scientific Programme<br />
Overall, the view from the<br />
evaluation forms was that the<br />
scientific programme was varied<br />
and very well balanced, with<br />
excellent quality of speakers.<br />
predictors would be to assess<br />
all patients, to treat them all<br />
blind to the assessment process,<br />
and then to compare the<br />
outcome with those<br />
assessments. Instead, lists of<br />
problems such as those above<br />
are used to be very selective<br />
about candidates for<br />
neuromodulation, so that if any<br />
predictors are found<br />
retrospectively, they can only<br />
apply within the limits of those<br />
selection procedures, which of<br />
course vary from clinic to clinic.<br />
<strong>The</strong>se exclusion criteria easily<br />
become proxies for refusing<br />
patients who are already<br />
underserved and disadvantaged.<br />
A close look at the literature on<br />
psychological screening for<br />
neuromodulation shows<br />
generally poor methodologies<br />
and a strong influence from<br />
insurance based health funding<br />
which characteristically focuses<br />
on shortcomings in the<br />
patient/claimant.<br />
Given the unpredictable success<br />
of neuromodulation and the<br />
distress caused by pain and<br />
unsuccessful treatment, what<br />
should psychological screening<br />
aim to achieve? <strong>The</strong>re is<br />
certainly benefit in eliciting<br />
patients’ understanding (or<br />
misunderstanding) both of their<br />
pain problem and of<br />
neuromodulation procedures<br />
Which one of the following statements best describes the<br />
way that you would like the pain clinic to be organised?<br />
(Tick one option)<br />
1- More new patient appointments with a short follow up period<br />
and discharge back to GP care.<br />
2- More new patient appointments with a treatment plan that is<br />
carried out and maintained by the GP. No routine follow up in the<br />
pain clinic.<br />
3- Fewer new patient appointments with long term follow up by the<br />
pain clinic.<br />
regulars<br />
Demographic data<br />
Mean Range<br />
Number of partners 5 1-14<br />
list size 8000 1800-34000<br />
12 training practices and 22 non-training practices were represented.<br />
Organisational issues<br />
A number of participants were from outside Nottingham so gave<br />
responses related to experience with their local provider of pain<br />
services.<br />
How long do<br />
your patients<br />
have to wait<br />
for a routine<br />
pain clinic<br />
appointment?<br />
Option 1 70%<br />
Communication<br />
Do you expect<br />
to receive a<br />
letter after<br />
each<br />
outpatient<br />
episode in the<br />
pain clinic?<br />
How often<br />
does this<br />
happen?<br />
12 Letters to the Editor<br />
16 Special Interest Groups<br />
22 Reflections from the<br />
coalface<br />
What do you<br />
think is an<br />
acceptable<br />
waiting time<br />
for a routine<br />
pain clinic<br />
appointment?<br />
In order to reduce the waiting time for a new patient<br />
routine appointment at the pain clinic it would be<br />
necessary to reduce the number of follow up appointments.<br />
How would<br />
you rate this<br />
change?<br />
How long does it take for a letter to arrive at your practice<br />
after the<br />
patients’ pain<br />
clinic<br />
consultation?<br />
Comments<br />
“A brief letter with a treatment plan is all that is needed.”<br />
“<strong>The</strong> letters are very important because chronic pain patients are<br />
very demanding and frequent attendees who always want<br />
information from the hospital.”<br />
CONTENTS THE PAIN SOCIETY NEWSLETTER SUMMER 2003 3
President’s<br />
message<br />
DR.BEVERLY COLLETT<br />
Welcome to the summer<br />
Newsletter and my opportunity<br />
to share some thoughts with<br />
you.<br />
Glasgow hosted a spectacular<br />
Annual Scientific Meeting. A<br />
marvellous venue and a superb<br />
scientific programme<br />
contributed to this success. We<br />
were educated and challenged<br />
by lecturers from North America<br />
and Europe as well as by<br />
distinguished colleagues from<br />
our own shores. We owe a debt<br />
of thanks to David Rowbotham,<br />
Chairman of the Courses and<br />
Meetings Committee and to his<br />
team for compiling this<br />
excellent programme. David is<br />
now stepping down from this<br />
role and we thank him for his<br />
most valued contribution to the<br />
ongoing improvement of the<br />
standard of our ASM. Paul<br />
Watson has taken on this<br />
important task and plans are<br />
well underway for 31st March-<br />
2nd April 2003 in Manchester.<br />
Please let him know of any<br />
articulate, interesting and<br />
amusing speakers so that we<br />
can continue to present a varied<br />
multidisciplinary high quality<br />
programme.<br />
Congratulations to Kate Grady,<br />
Andrew Rice, Pat Schofield and<br />
Cathy Stannard, our new<br />
Council members. <strong>The</strong>y were<br />
elected from a very strong field<br />
and it is to the <strong>Society</strong>’s great<br />
benefit that we do have<br />
members who are willing to put<br />
in the extra time needed to<br />
work on your behalf.<br />
Commiserations if you were not<br />
successful on this occasion.<br />
However, I do hope that you<br />
will consider standing again.<br />
Cathy Stannard will be no<br />
stranger to you having recently<br />
passed on the Editor’s role of<br />
the Newsletter to Stephen<br />
Ward. Cathy’s thoughtprovoking<br />
observations on the<br />
state of pain management will<br />
be familiar to you from her<br />
Editorials and we look forward<br />
to much lively debate in our<br />
future Council meetings. Andy<br />
Vickers and Cathy Stannard<br />
have been appointed joint<br />
chairs of a new Committee<br />
tasked with looking at Clinical<br />
Governance issues for the <strong>Pain</strong><br />
<strong>Society</strong>. Pat Schofield and<br />
Andrew Rice are highly<br />
regarded for their academic<br />
credentials and we welcome<br />
their input into Council. Kate<br />
Grady will be involved in the<br />
Courses and Meetings<br />
Committee and will also be<br />
attending the Association of<br />
Palliative Medicine on our<br />
behalf.<br />
George Harrison has taken over<br />
from William Campbell as<br />
Honorary Treasurer. I should like<br />
to thank William for<br />
maintaining robust control of<br />
the <strong>Society</strong>’s finances,which<br />
continue to be soundly based.<br />
<strong>The</strong> <strong>Pain</strong> <strong>Society</strong> is in the<br />
fortunate position of being the<br />
beneficiary of two recent<br />
legacies. We have been notified<br />
that Mrs Irene Bainbridge of<br />
Stanhope, Co Durham has<br />
bequeathed a third of her<br />
residuary estate to the <strong>Pain</strong><br />
<strong>Society</strong> for its general purposes.<br />
We do not yet know the exact<br />
amount, but it is estimated that<br />
we will receive approximately<br />
£400,000.00. I have contacted<br />
her family to thank them for<br />
this most generous legacy, but<br />
do please let me know if you<br />
knew this lady. We have also<br />
been advised that Elaine<br />
Elizabeth Clulow, who died in<br />
April 2003, has left a legacy to<br />
the <strong>Pain</strong> <strong>Society</strong> for basic<br />
research into the causes and<br />
cure of pain. Council will be<br />
discussing how both these<br />
monies should properly be<br />
spent and will let you know<br />
what is agreed.<br />
I should like to convey my<br />
thanks to Dr. Douglas Justins<br />
our Immediate Past-President,<br />
who has skillfully crafted the<br />
<strong>Pain</strong> <strong>Society</strong> through the last<br />
two years. Douglas has<br />
considerable knowledge and<br />
perception in matters pertaining<br />
to the Royal College of<br />
Anaesthetists. It is essential that<br />
this important link is maintained<br />
and I am extremely pleased that<br />
he will continue to give us the<br />
benefit of this expertise by<br />
further work on <strong>Pain</strong> <strong>Society</strong><br />
Council as Immediate Past-<br />
President and as the<br />
representative of the Royal<br />
College of Anaesthetists.<br />
Congratulations to Professor<br />
Mike Harmer on his election as<br />
the next President of the<br />
Association of Anaesthetists of<br />
Great Britain and Ireland. We<br />
are delighted that an<br />
anaesthetist with an interest in<br />
pain management is<br />
undertaking this important role.<br />
We look forward to greater<br />
collaboration between our two<br />
organisations in the future.<br />
You should all have received a<br />
copy of the Provisional<br />
Recommendations for the<br />
Appropriate Use of Opioids in<br />
Patients with Chronic Noncancer<br />
Related <strong>Pain</strong>. Please<br />
feedback comments to Dr Karen<br />
Simpson, Honorary Secretary<br />
and Chair of the<br />
Communications Committee as<br />
soon as possible. <strong>The</strong> joint<br />
Working Group will be meeting<br />
during the summer to finalise<br />
this document. Council are<br />
pleased to announce that Dr<br />
Simpson will also be convening<br />
a Working Group to develop<br />
guidelines for Neuromodulation<br />
in conjunction with the<br />
Neuromodulation SIG. Draft<br />
proposals should be completed<br />
for the ASM next year. I think<br />
that you will appreciate that<br />
wide consultation and<br />
collaboration amongst various<br />
interested specialities is<br />
essential if <strong>Pain</strong> <strong>Society</strong><br />
recommendations are to have<br />
any credibility.<br />
I thank those of you who<br />
completed the Dr Foster<br />
questionnaire. <strong>The</strong> full Report is<br />
included with this mailing- so<br />
please do read it. It had been<br />
hoped a Sunday newspaper<br />
would publish it. But, even the<br />
likes of Dr Foster was unable to<br />
excite the interest of the written<br />
media in the current state of<br />
<strong>Pain</strong> Management Services.<br />
<strong>The</strong>re was some TV and radio<br />
coverage for those of you with<br />
‘early morning wakening’ and<br />
an article in the Independent.<br />
Unfortunately, the media’s<br />
perception of patients with pain<br />
and of NHS services available<br />
for them is that it does not sell<br />
newspapers.<br />
<strong>The</strong> results mirrored those of<br />
the CSAG Report in that <strong>Pain</strong><br />
Management Services continue<br />
to be ‘Cinderella’ services.<br />
Availability is variable, as are<br />
the treatments offered to<br />
patients. Only 58% of services<br />
4<br />
THE PAIN SOCIETY NEWSLETTER<br />
SUMMER 2003<br />
PRESIDENT’S MESSAGE
offer <strong>Pain</strong> Management<br />
Programmes despite the<br />
evidence of efficacy. What<br />
happens to patients in the other<br />
42% of services? Do these<br />
patient get offered PMPs<br />
outside of their locality, is this<br />
funded, is it practical or is it not<br />
a treatment option? I think that<br />
Dr. Foster behoves us all to look<br />
critically at how we organise<br />
our services. Given the recent<br />
emphasis on meeting<br />
Government waiting-list targets,<br />
it is not surprising that the<br />
waiting time for most services<br />
was within 21 weeks. Some<br />
services still have extremely<br />
long waiting times (up to 110<br />
weeks) and four services are not<br />
currently accepting GP referrals.<br />
Importantly, we must ask<br />
whether pain services are<br />
suffering as resources are<br />
diverted to those specialities<br />
made national priorities as<br />
defined by a National Service<br />
Framework or to fund additional<br />
anaesthetic sessions to reduce<br />
waiting times for surgery.<br />
Moreover, we must not confuse<br />
quantity with quality. <strong>The</strong><br />
average length of a new patient<br />
consultation was 34 minutesalthough<br />
some of us at times<br />
have to see a new patient in 10<br />
minutes, perhaps due to<br />
waiting-list pressures. All of us<br />
have a responsibility to<br />
highlight the deficiencies in<br />
service provision both locally<br />
and where possible nationally.<br />
More positively, on June11th,<br />
the Associate Parliamentary<br />
Health Group held a seminar on<br />
‘ Chronic <strong>Pain</strong>- A Silent<br />
Epidemic?’ <strong>The</strong> <strong>Pain</strong> <strong>Society</strong> and<br />
the Royal College of General<br />
Practitioners <strong>Pain</strong> Management<br />
Committee were key players in<br />
this meeting for MPs. Jointly, we<br />
launched ‘5 pledges to help<br />
people living with persistent<br />
pain.’ <strong>The</strong>se five pledges have<br />
been endorsed with an Action<br />
Plan that Parliamentarians, NHS<br />
services commissioners,<br />
healthcare professionals,<br />
patients and educators can<br />
follow. <strong>The</strong> possibility of a<br />
National Service Framework for<br />
<strong>Pain</strong> in Wales was raised. Will<br />
our Welsh compatriots steal a<br />
march over the rest of us<br />
again? It is vital that the<br />
initiative gathered at this<br />
meeting is further progressed.<br />
<strong>The</strong> Chairman, Barry Sheerman<br />
MP, has given an assurance to<br />
raise the profile of chronic pain<br />
with David Hinchcliffe,<br />
Chairman of the Parliamentary<br />
Health Select Committee. We<br />
are meeting again in six months<br />
to ascertain what progress has<br />
been made.<br />
<strong>The</strong> Patient Liaison Committee<br />
will be holding “An interactive<br />
workshop- Barriers to effective<br />
care” for people living with<br />
chronic pain on 13th October<br />
2003 at the Royal College of<br />
Nursing to mark European<br />
Week against <strong>Pain</strong>. This will<br />
build on the great success of<br />
last year’s inaugural event.<br />
Again, it will give an<br />
opportunity for health<br />
professionals, patients and<br />
carers to discuss experiences<br />
and challenges within pain<br />
management. This committee<br />
works exceptionally hard for the<br />
<strong>Pain</strong> <strong>Society</strong>. It is an example of<br />
how professional and lay<br />
members can work together to<br />
improve patient care in the<br />
broadest sense. I must thank<br />
Jean Gaffin, Chair of this<br />
committee for her expertise and<br />
insight in this pivotal role.<br />
Congratulations to Dr. Clare<br />
Daniel and Dr. Lesley Colvin<br />
who gained the Pfizer<br />
Neuropathic <strong>Pain</strong> awards. A<br />
large number of high quality<br />
applications were received<br />
despite very tight timelines. It<br />
does show that members are<br />
keen to do research- but that<br />
money is needed. We look<br />
forward to receiving the results<br />
of this research at next years<br />
ASM. Our thanks go to Pfizer<br />
whose financial support made<br />
these awards possible.<br />
Plans continue to progress with<br />
regard to incorporation of the<br />
<strong>Pain</strong> <strong>Society</strong>. At the AGM, a<br />
decision was taken for the<br />
<strong>Society</strong> to be renamed the<br />
<strong>British</strong> <strong>Pain</strong> <strong>Society</strong> after<br />
incorporation. A meeting of<br />
Officers and SIG chairman is<br />
planned for 11th July to discuss<br />
the changes that incorporation<br />
will necessitate and we do hope<br />
to have a good turnout for this<br />
important meeting.<br />
<strong>The</strong> Royal College of<br />
Anaesthetists and the <strong>Pain</strong><br />
<strong>Society</strong> will soon be publishing<br />
<strong>Pain</strong> Management Services:<br />
Good Practice. This document<br />
clearly highlights the<br />
importance of the management<br />
of pain and that the<br />
multidisciplinary approach fits<br />
well with the modern day skill<br />
mix and patient-centred<br />
approach of the NHS. It states<br />
very clearly that working<br />
arrangement for the pain<br />
specialist should resemble that<br />
of a consultant physician in<br />
terms of sessional allocation,<br />
accommodation and<br />
administration services. This<br />
document raises many clinical<br />
governance issues for<br />
anaesthetic members of the<br />
<strong>Pain</strong> <strong>Society</strong>. Translating this<br />
document into clinical practice<br />
is the next step.<br />
<strong>The</strong> <strong>British</strong> Medical Journal<br />
recently devoted a whole issue<br />
to the vexed question of the<br />
relationships between drug<br />
companies and doctors.<br />
Pharmaceutical companies<br />
impact upon us both<br />
individually and as a whole. <strong>The</strong><br />
NHS, as a large organisation, is<br />
almost unique in not financing<br />
education and ongoing<br />
professional development and<br />
expecting its employees to<br />
mostly fund these themselves.<br />
As a multidisciplinary society,<br />
this impacts significantly on<br />
many of our members and does<br />
expose potential vulnerabilities<br />
and leads to inequalities. <strong>The</strong><br />
challenge is to facilitate the<br />
best of the relationships with<br />
pharmaceutical companies<br />
without letting the resulting<br />
flows of goodwill, money and<br />
influence distort the caring,<br />
healing and teaching<br />
dimensions of medicine. Council<br />
and society members must be<br />
appropriate and open in<br />
dealings with the<br />
pharmaceutical industry. In<br />
September, Council will be<br />
debating this issue, which will<br />
undoubtedly continue as a topic<br />
of debate in practice.<br />
Dr Peter Nathan, Neurologist at<br />
the National Hospital for<br />
Neurology and Neurosurgery<br />
died peacefully at his home in<br />
London at the age of 88years.<br />
Peter was a founding member<br />
both of IASP and of the <strong>Pain</strong><br />
<strong>Society</strong>. A very moving obituary<br />
has already been written in <strong>Pain</strong><br />
to note his very great<br />
achievements, including those in<br />
the field of clinical pain<br />
research. I would concur with<br />
Geoff Schott that ‘it has been a<br />
privilege for so many of us, now<br />
and in the past, to have known<br />
and learnt from this most<br />
distinguished, cultured, and<br />
loveable man.’<br />
John Reid is now the new<br />
Minister for Health. Alan<br />
Milburn is off to spend more<br />
time with his family- so should<br />
you. Have a good summer<br />
break!<br />
PRESIDENT’S MESSAGE THE PAIN SOCIETY NEWSLETTER SUMMER 2003 5
PAIN MEETINGS FOR<br />
HEALTH PROFESSIONALS<br />
CELLULAR AND MOLECULAR MECHANISMS OF PAIN<br />
a satellite symposium to the International Brain<br />
Research Organization (IBRO)<br />
7-9 July Prague, Czech Republic<br />
Email:palecek@biomed.cas.cz / wdwillis@utmb.edu<br />
Web: http://www.biomed.cas.cz/IBRO-PAIN/<br />
BATH PAIN FORUM - CATASTROPHISING ABOUT<br />
CHRONIC PAIN<br />
29 July, Royal National Hospital for Rheumatic Diseases, Bath<br />
Contact: Dr. Chris Eccleston<br />
Director, <strong>Pain</strong> Management Unit,<br />
University of Bath<br />
Email: pain@bath.ac.uk<br />
PAIN IN EUROPE IV - 4TH CONGRESS OF THE EUROPEAN<br />
FEDERATION OF IASP CHAPTERS (EFIC)<br />
2-6 September, Prague, Czech Republic<br />
Contact: Congress Business Travel<br />
Email: pain2003@cbttravel.cz<br />
Web: www.pain2003.cz<br />
9TH NATIONAL CONFERENCE ON PAIN MANAGEMENT<br />
PROGRAMMES<br />
Organised by the <strong>Pain</strong> Management Special Interest<br />
Group of the <strong>Pain</strong> <strong>Society</strong><br />
11-12 September, John Innes Centre and University of East Anglia<br />
Contact: Elaine Wellingham<br />
Conference Secretariat, Field End House<br />
Bude Close, Nailsea<br />
Bristol BS48 2FQ<br />
Tel/Fax: 01275 853311<br />
Email: Confsec@blueyonder.co.uk<br />
THE FUTURE OF PAIN THERAPUTICS 2003<br />
15-16 September 2003, London<br />
Email: sara.peerun@visiongain.com<br />
http://www.visiongain.com/futurepaindrugs.html<br />
Glasgow ASM 2003 :<br />
Overview<br />
Breakdown of delegates<br />
<strong>The</strong>re were a total number of<br />
1,066 Delegates registered at<br />
the Meeting; an increase of 264<br />
from the 2002 Meeting in<br />
Bournemouth. 50 were<br />
Anaesthetic Research Delegates.<br />
Of the 1066, 70% were<br />
members of the <strong>Society</strong>.<br />
<strong>The</strong> specialty of the delegates<br />
continues to mirror the<br />
membership of the <strong>Society</strong>, with<br />
anaesthetists making up the<br />
largest group of delegates,<br />
followed by nurses,<br />
psychologists, physiotherapists,<br />
occupational therapists and<br />
general practitioners.<br />
Venue<br />
<strong>The</strong> Glasgow Scottish Exhibition<br />
+ Conference Centre was an<br />
excellent venue for this year’s<br />
ASM and perfectly suited the<br />
<strong>Society</strong>’s needs in terms of<br />
quality of plenary hall, number<br />
of break-out rooms and size of<br />
exhibition area. <strong>The</strong> support<br />
staff was excellent and the<br />
additional facilities at the<br />
Centre i.e. café bar, restaurant<br />
and business desk all added to<br />
the success of the meeting.<br />
Scientific Programme<br />
Overall, the view from the<br />
evaluation forms was that the<br />
scientific programme was varied<br />
and very well balanced, with<br />
excellent quality of speakers.<br />
PROVING OUR WORTH!<br />
Specialist Nurses & Nurse Consultants Conference<br />
25 September<br />
Post Graduate Medical Centre, Worthing Hospital, West Sussex<br />
THE PAIN RELIEF FOUNDATION 4TH ANNUAL LECTURE<br />
2003<br />
<strong>Pain</strong> & Central Nervous System Reorganisation”<br />
Friday,17th October at 7:00 pm<br />
<strong>The</strong> <strong>Pain</strong> Research Institute, Clinical Sciences Centre, University<br />
Hospital Aintree, Liverpool<br />
Professor Troels Jensen<br />
Danish <strong>Pain</strong> Research Centre, University of Åarhus, Denmark<br />
AN UNRECOGNISED PAIN CHALLENGE<br />
a one-day conference on Joint Hypermobility<br />
Syndrome<br />
21 October 2003, 9.30 - 4.40<br />
Postgraduate Centre, Gassiot House, St Thomas' Hospital<br />
6<br />
THE PAIN SOCIETY NEWSLETTER<br />
SUMMER 2003<br />
NEWS FROM PORTLAND PLACE
<strong>The</strong> plenary lectures received<br />
particularly high praise, both<br />
with regards to the range of<br />
topics and choice of speakers.<br />
Both Prof Herta Flor’s and Prof.<br />
Howard Field’s plenary lectures<br />
received particularly high marks<br />
out of the 9 lectures. Once<br />
again, a number of delegates<br />
asked for there to be ‘questions<br />
and answers’ during the plenary<br />
sessions.<br />
A number of delegates felt<br />
there were too many workshop<br />
choices running at the same<br />
time and it was also felt that<br />
there was too much repetition<br />
in the workshop sessions, which<br />
involved the plenary speakers.<br />
Workshop sessions, which<br />
received a particularly excellent<br />
feedback were How to Get Your<br />
<strong>Pain</strong> Management Programme<br />
Funded and the Psychology SIG:<br />
Changing Self-identity in<br />
Chronic <strong>Pain</strong>. Feedback<br />
received from the<br />
Clerical/Managerial Staff was<br />
very positive indeed, and found<br />
the session on Principles of <strong>Pain</strong><br />
Management extremely<br />
interesting and useful and<br />
asked for it to be repeated next<br />
year.<br />
<strong>The</strong> list of workshop topic<br />
suggestions for the 2004 ASM,<br />
has been forwarded to the<br />
Courses & Meetings Committee.<br />
Prize Paper Presentation<br />
and Poster Exhibition<br />
<strong>The</strong> Prize Paper Presentation<br />
session, once again, proved to<br />
be a great success and<br />
following feedback from the<br />
2002 ASM, was allocated a<br />
main session in the plenary hall.<br />
<strong>The</strong> winners of the Prize Paper<br />
Presentations were as follows:<br />
1st Prize - Poster No. 94:<br />
“Future Possible Selves”<br />
conditionality and adjustment to<br />
chronic pain.<br />
Prof. Stephen Morley<br />
2nd Prize - Poster No. 100 :<br />
Efficacy of two cannabis based<br />
medicinal extracts for relief of<br />
central neuropathic pain from<br />
brachial plexus avulsion: results<br />
of a randomized controlled trial.<br />
Dr Jonathan Berman<br />
3rd Prize - Poster No. 68: <strong>The</strong><br />
WEST Study - a cost<br />
effectiveness study of epidural<br />
steroids in the management of<br />
sciatica: 12 month effectiveness<br />
data.<br />
Dr Cathy Price<br />
160 posters made up this year’s<br />
Exhibition and proved to be a<br />
very valuable and interesting<br />
part of the meeting, but a<br />
number of authors felt that<br />
allotted times should be given<br />
during the course of the<br />
meeting, when they are to<br />
stand by their poster to discuss<br />
their work; this will be reviewed<br />
for the 2004 meeting.<br />
Technical Exhibition<br />
<strong>The</strong> Technical Exhibition was<br />
perfectly situated giving the<br />
exhibitors maximum exposure -<br />
feedback received from the<br />
exhibitors was very positive<br />
indeed. 60 stands were sold,<br />
with a total of 64 stands in the<br />
Exhibition (<strong>Pain</strong> <strong>Society</strong>/IASP<br />
stand, Charity Literature stand,<br />
PACS stand and DIPEX stand<br />
making up the additional 4<br />
stands).<br />
Catering<br />
Although the majority of<br />
delegates felt that the lunchbox<br />
was a very good idea, as it<br />
avoided queuing, the poor<br />
quality of the food was perhaps<br />
the one thing people<br />
complained most about.<br />
Satellite Meetings<br />
<strong>The</strong>re were three satellite<br />
meetings in total this year,<br />
Merck Sharp & Dohme, Pfizer<br />
Ltd and Janssen-Cilag. <strong>The</strong><br />
attendance figures and the<br />
results from the evaluation<br />
forms showed that delegates<br />
are very interested in this aspect<br />
of the meeting, which proves to<br />
be more and more successful<br />
each year.<br />
MANAGING CANCER PAIN<br />
A half-day course for members of all Healthcare<br />
Professions with Professor Frank Keefe, in Bristol on<br />
the afternoon of Tuesday 21st October 2003.<br />
Application form from: Anne Hartley, administrator, <strong>Pain</strong><br />
Management Centre, Frenchay Hospital, Frenchay Park Road, Bristol<br />
BS16 1LE.<br />
Tel: 0117 975 3890<br />
E-Mail: anne.hartley@north-bristol.swest.nhs.uk<br />
Cheques for the sum of £40 made payable to “<strong>The</strong> North Bristol<br />
NHS Trust” to be sent with application form by 22nd September<br />
2003.<br />
MANAGING PAIN IN RHEUMATOLOGICAL DISEASE<br />
A half day course for members of all Healthcare<br />
Professions with Professor Frank Keefe in Bristol on<br />
Tuesday 21st October 2003<br />
Please register an early interest in attending with Heather Muncey<br />
on: Tel: 0117 975 3890<br />
Email: Heather.Muncey@north-bristol.swest.nhs.uk<br />
BATH PAIN FORUM - PHANTOM PAIN<br />
4 November, Royal National Hospital for Rheumatic Diseases, Bath<br />
Contact: Dr. Chris Eccleston<br />
Director, <strong>Pain</strong> Management Unit,University of Bath<br />
Email: pain@bath.ac.uk<br />
2004<br />
PAIN RELIEF FOUNDATION -<br />
20th ANNUAL CLINICAL MANAGEMENT OF CHRONIC<br />
PAIN COURSE<br />
10-14 November<br />
PAIN SOCIETY 37TH ANNUAL SCIENTIFIC MEETING<br />
30 March – 2 April, Manchester, UK<br />
Abstract Deadline: Friday 30 January 2004<br />
7th INTERNATIONAL CONFERENCE ON THE<br />
MECHANISMS AND TREATMENT OF NEUROPATHIC PAIN<br />
13-16 May 2004, Madrid, Spain<br />
Social Programme<br />
This year’s Drinks Reception was<br />
a huge success. <strong>The</strong> Science<br />
Park was of obvious interest to<br />
the majority of the delegates<br />
and added greatly to the<br />
success of the evening. <strong>The</strong><br />
venue for the Annual Dinner<br />
was most impressive, so too<br />
was the food, but the evening<br />
was let down a little by poor<br />
acoustics.<br />
Conclusion<br />
Overall, the Meeting was a<br />
great success in terms of the<br />
well-balanced scientific content,<br />
the high quality of speakers, the<br />
excellent organisation and the<br />
suitability of the venue. In<br />
addition, the Technical<br />
Exhibition, the satellite<br />
meetings and the social<br />
programme made the Meeting<br />
an all round positive,<br />
informative and enjoyable<br />
event.<br />
<strong>The</strong> Courses & Meetings<br />
Committee would like to thank<br />
the 141 delegates who<br />
completed and returned their<br />
Evaluation Forms and is pleased<br />
to announce that Dr D R<br />
Hughes from Addenbrookes<br />
Hospital in Cambridge has won<br />
£100 worth of Waterstones<br />
book vouchers!<br />
NEWS FROM PORTLAND PLACE THE PAIN SOCIETY NEWSLETTER SUMMER 2003 7
<strong>The</strong> <strong>Society</strong> wishes to congratulate both Claire Daniel (£25,000) and Leslie Colvin (£5,000) for their successful <strong>Pain</strong> <strong>Society</strong>/Pfizer grant award applications.<br />
We only have space to print the abstracts!<br />
A survey to define the<br />
characteristics of post<br />
thoracotomy pain<br />
DR LESLEY COLVIN<br />
Consultant/ Senior Lecturer<br />
Dept of Anaesthesia, Critical Care & <strong>Pain</strong> Medicine<br />
Western General Hospital<br />
Persistent pain after surgery is a<br />
significant problem, that is<br />
often not recognised or<br />
managed correctly. It is unclear<br />
whether this pain is<br />
predominantly neuropathic in<br />
nature, although peripheral<br />
nerve injury seems to be an<br />
important factor, with a high<br />
incidence being found after<br />
surgery involving nerve injury<br />
such as amputation (75%),<br />
thoracotomy (67%) and<br />
mastectomy (30%). In order to<br />
institute early and appropriate<br />
management, it is important to<br />
define the problem accurately.<br />
<strong>The</strong> primary aim of this study<br />
is to define and characterise<br />
post surgical pain in a patient<br />
group with a high incidence of<br />
this problem – patients<br />
undergoing thoracotomy. We<br />
aim to carry out a prospective<br />
survey of consecutive patients<br />
undergoing thoracotomy, in<br />
order to characterise the<br />
prevalence, severity and type of<br />
pain found in this population. In<br />
the clinical setting, in addition<br />
to sensory changes, many other<br />
emotional and cognitive factors<br />
may contribute to the<br />
experience of pain. Thus a<br />
detailed assessment of sensory<br />
changes using Quantitative<br />
Sensory Testing (QST) will be<br />
used in combination with use of<br />
structured validated<br />
questionnaires to examine<br />
psychological factors.<br />
Assessments will commence<br />
immediately pre-operatively to 3<br />
months post-operatively to<br />
determine changes that may<br />
indicate progression from acute<br />
to chronic.<br />
<strong>The</strong> main objective is to develop<br />
an evidence-based description<br />
of post thoracotomy pain. This<br />
can then serve as a tool to<br />
improve pain management in a<br />
clinical setting as well as<br />
providing valuable information<br />
for future research into<br />
mechanisms of neuropathic pain<br />
in a clinical setting.<br />
‘<strong>The</strong> Impact of<br />
Neuropathic <strong>Pain</strong> on<br />
the Psychological and<br />
Physical Quality of<br />
Life’<br />
DR H. CLARE DANIEL<br />
Clinical Psychologist & Research Associate<br />
Department of Anaesthesia & Intensive Care<br />
Imperial College London<br />
Chelsea and Westminster Campus<br />
It is widely acknowledged that<br />
differences exist between the<br />
models of neuropathic and<br />
musculoskeletal pain and also<br />
the quality of pain experienced<br />
(Melzack & Katz, 1999).<br />
However, differences in the<br />
impact of neuropathic and<br />
musculoskeletal pain have not<br />
been specifically addressed.<br />
Although the impact of<br />
musculoskeletal pain on quality<br />
of life is well documented<br />
(Eccleston, 2001; Vlaeyen et al.,<br />
2002), there is a paucity of data<br />
for the same in neuropathic<br />
pain.<br />
<strong>The</strong> studies that report<br />
psychological distress in the<br />
neuropathic pain population do<br />
so in the context of pain relief<br />
outcomes (Meyer-Rosenberg et<br />
al., 2001) rather than<br />
elucidating the specific impact<br />
of neuropathic pain<br />
(Haythornthwaite & Benrud-<br />
Larson, 2001; Schmader, 2002).<br />
It is suspected that this<br />
situation is a contributing factor<br />
to the minimal focus that that<br />
has been placed on cognitive<br />
behavioural interventions and<br />
neuropathic pain.<br />
<strong>The</strong>refore, the small percentage<br />
of people with neuropathic pain<br />
who do receive cognitive<br />
behavioural pain management<br />
generally receive an intervention<br />
that is validated by research on<br />
musculoskeletal pain (Evans &<br />
Fishman, 1997).<br />
Although these interventions<br />
are effective in musculoskeletal<br />
pain (Morley, Eccleston &<br />
Williams, 1999), ‘there are no<br />
noteworthy, evidence based<br />
studies specifically evaluating<br />
these techniques in neuropathic<br />
pain’ (Harden & Cohen, 2003).<br />
This two-cohort postal<br />
questionnaire survey will aim:<br />
1. To identify the impact of<br />
neuropathic pain on<br />
psychological and physical<br />
quality of life and on<br />
everyday functioning<br />
2. To identify key beliefs about<br />
causation and mechanisms<br />
of neuropathic pain held by<br />
people with postherpetic<br />
neuralgia<br />
3. To identify key problems in<br />
the psychological and<br />
physical functioning of<br />
patients with postherpetic<br />
neuralgia<br />
4. To identify similarities and<br />
differences in 1-3 above<br />
between a postherpetic<br />
neuralgia population and<br />
those with musculoskeletal<br />
pain<br />
8<br />
THE PAIN SOCIETY NEWSLETTER<br />
SUMMER 2003<br />
NEWS FROM PORTLAND PLACE
Obituary<br />
MARK SWERDLOW<br />
Mark Swerdlow created the<br />
specialty of pain medicine in Great<br />
Britain. Although others may claim<br />
to have started pain clinics before<br />
Mark, it was he who called<br />
together those who had an<br />
interest in the relief of pain, and<br />
he who held the meeting that led<br />
to the formation of the Intractable<br />
<strong>Pain</strong> <strong>Society</strong> (IPS) in 1967. <strong>The</strong> IPS<br />
later merged with the <strong>British</strong> and<br />
Irish Chapter of the International<br />
Association for the Study of <strong>Pain</strong>,<br />
to form the large and active body<br />
that it is today. Mark was the first<br />
Chairman of the IPS, but it is<br />
typical of the man that he<br />
arranged for another to hold the<br />
post of President while he got on<br />
with organising the running and<br />
development of the new society.<br />
Mark Swerdlow was born in 1920<br />
and graduated MB ChB from<br />
Manchester and held both M.Sc<br />
and MD degrees from that<br />
university. He served with<br />
distinction in the Royal Army<br />
Medical Corps from 1943 to 1948<br />
and saw service in France,<br />
Belgium, Holland and Germany.<br />
On his return he specialised in<br />
anaesthesia and held the Diploma<br />
in Anaesthesia and was a Fellow<br />
of the Faculty of Anaesthetists of<br />
the Royal College of Surgeons of<br />
England. He spent time as an<br />
Exchange Fellow at the University<br />
of Pittsburgh in 1954 before<br />
being appointed as Consultant<br />
Anaesthetist to the Salford<br />
Hospital Group, University of<br />
Manchester School of Medicine.<br />
In 1955 he founded the pain clinic<br />
which became the North West<br />
Regional <strong>Pain</strong> Relief Centre<br />
twenty four years later and which<br />
remains to this day one of the<br />
finest pain management centres<br />
in the world. Throughout his<br />
career Mark was incredibly<br />
productive as an administrator,<br />
but it is his role as an educator<br />
that made a permanent and<br />
beneficial impact upon the<br />
management of pain. Mark wrote<br />
or co-wrote seven textbooks and<br />
numerous book chapters and<br />
articles about the clinical<br />
treatment of pain. Over a thirty<br />
year period his academic<br />
production was consistent, prolific<br />
and wide-ranging.<br />
He was in great demand as a<br />
lecturer and had a fund of<br />
practical knowledge that was<br />
simply unsurpassable. He had an<br />
ability to recognise when<br />
techniques of pain relief were<br />
becoming outmoded and he never<br />
dwelt in the past, but encouraged<br />
all he came into contact with to<br />
change and improve their practice<br />
where possible. His worldwide<br />
contributions were recognised by<br />
over a dozen visiting<br />
professorships, membership of<br />
editorial boards and honorary<br />
memberships of national and<br />
international societies. He was<br />
Adviser to the World Health<br />
Organization Cancer <strong>Pain</strong> Relief<br />
Programme from 1981 to 1987.<br />
<strong>The</strong> formal recognition and<br />
honours tell nothing of the<br />
gentleman who was Mark<br />
Swerdlow; a man who had perfect<br />
manners and who always listened<br />
to and considered the views of<br />
others. Mark was generous with<br />
his wisdom and practical<br />
knowledge and rarely critical<br />
without good reason. Retirement<br />
permitted him to enjoy his wide<br />
range of interests and his music<br />
and painting were a source of<br />
pleasure. He read a paper at the<br />
Welcome Institute only two<br />
months before his sudden death<br />
from complications of a brain<br />
tumour. He was 84 years of age.<br />
He is survived by his wife<br />
Elizabeth and three children: a<br />
son, currently Professor of<br />
Epidemiology at the Royal<br />
Marsden Hospital, and two<br />
daughters. Our sympathy is<br />
extended to them all.<br />
Mark Swerdlow, pioneer pain<br />
clinician, died 26 February, 2003.<br />
J. E. CHARLTON.T.P.NASH<br />
June 2003<br />
10<br />
THE PAIN SOCIETY NEWSLETTER<br />
SUMMER 2003<br />
NEWS FROM PORTLAND PLACE
New Membership Applicants<br />
Mrs J Barrett<br />
Mr Stephen Bliss<br />
Miss Jane Bott<br />
Dr Eric Brodie<br />
Mrs Pauline Chinn<br />
Miss Ursula Collignon<br />
Mrs Jill Compton<br />
Dr Jon Cort<br />
Dr Christina Cox<br />
Dr Natasha Curran<br />
Dr Mark Dale<br />
Dr H Clare Daniel<br />
Dr Chris Davies<br />
Dr Paul Dawson<br />
Dr Lorraine de Gray<br />
Dr Johannes Van der<br />
Merwe<br />
Mr Graeme Dickson<br />
Mr B Drysdale<br />
Miss Ruth Edgecumbe<br />
Miss Louise Evans<br />
Dr Ronald Feathers<br />
Dr Jo Fitz-Henry<br />
Mrs Marion Francis<br />
Dr Aidan Gill<br />
Mrs Sara Goulder<br />
Miss Gillian Gourlay<br />
Dr Gary Gutteridge<br />
Dr Sarah Halliday<br />
Mr Alan Hassard<br />
Mrs Jacqui Hawkins<br />
Dr Melanie Hearn<br />
Mrs Suzanne Henderson<br />
Miss Stella Howden<br />
Dr Martin Johnson<br />
Mrs Hilary Jones<br />
Ms Judith Kappesser<br />
Mrs Jane Knight<br />
Ms Kate Mackie<br />
Dr Ivan Marples<br />
Mrs Lesley Marshall<br />
Dr Dennis Marshall-<br />
Hasdell<br />
Miss Sophia<br />
Mavrommatis<br />
Nurse Specialist<br />
Senior Physiotherapist<br />
Physiotherapist<br />
Reader in Psychology<br />
Acute <strong>Pain</strong> Nurse<br />
Acute <strong>Pain</strong> Pharmacist<br />
<strong>Pain</strong> Clinic Sister<br />
Consultant Anaesthetist<br />
Consultant Anaesthetist<br />
SpR Anaesthesia<br />
SpR Anaesthesia<br />
Clinical Psychologist<br />
Clinical Psychologist<br />
Consultant Anaesthetist<br />
SpR Anaesthesia<br />
Consultant Clinical<br />
Psychologist<br />
Charge Nurse<br />
Clinical Psychologist<br />
Acute <strong>Pain</strong> Management<br />
Sister<br />
Assistant Scientist<br />
Clinical Assistant<br />
Consultant Anaesthetist<br />
Staff Nurse<br />
Medical Director<br />
Staff Nurse<br />
Assistant Scientist<br />
Consultant Anaesthetist<br />
Clinical Psychologist<br />
Clinical Psychologist<br />
Clinical Specialist<br />
Physiotherapist<br />
Consultant Anaesthetist<br />
Acute <strong>Pain</strong> Sister<br />
Post Graduate Researcher<br />
General Practitioner<br />
Staff Nurse<br />
PhD Student<br />
Occupational <strong>The</strong>rapist<br />
<strong>Pain</strong> Directorate Pharmacist<br />
Consultant in <strong>Pain</strong><br />
Medicine<br />
Senior Physiotherapist<br />
Manager<br />
Senior Physiotherapist<br />
Dorset County Hopsital<br />
Kings Mill Hospital<br />
Royal National Hospital<br />
Glasgow Caledonian<br />
University<br />
Peterborough Hospitals<br />
NHS Trust<br />
Guys & St Thomas’s NHS<br />
trust<br />
Addenbrookes Hospital<br />
Chesterfield Royal Hopsital<br />
Salisbury District Hospital<br />
North Middlesex Hospital<br />
Leicester University<br />
Hospital<br />
Chelsea & Westminster<br />
Hospital<br />
Wansbeck General Hospital<br />
Southampton General<br />
Hopsital<br />
Addenbrookes Hospital<br />
St Thomas’s Hospital<br />
St James University<br />
Hospital<br />
Psychology Dept North<br />
Place<br />
Birmingham Heartlands<br />
NHS Trust<br />
Organon Laboratories<br />
Kent & Canterbury<br />
Hospital<br />
Nottingham City Hospital<br />
BUPA Hospital, Leeds<br />
Scirex Ltd<br />
Addenbrookes Hospital<br />
Organon Laboratories<br />
Bristol Royal Infirmary<br />
University Hospital<br />
Birmingham<br />
Derriford Hospital<br />
Worthing Hospital<br />
Torbay Hospital<br />
University Hospital of<br />
Hartlepool<br />
Queen Margaret University<br />
College<br />
Ashville Medical Centre<br />
St Marys Hospital<br />
St Thomas’s Hospital<br />
Royal Bolton Hospital<br />
Middlesex Hospital<br />
Western General Hospital<br />
Astley Ainslie Hospital<br />
Vocational <strong>Pain</strong> Service<br />
Royal National<br />
Orthopaedic Hospital<br />
Ms Jean McCallum<br />
Mrs Lorraine McMain<br />
Miss Katie Mullins<br />
Dr Susan Nimmo<br />
Mrs Suzanne Nimmo<br />
Dr Jonathan Norman<br />
Mrs Moira O’Gorman<br />
Mrs Lynne Owen<br />
Ms E Phipps<br />
Ms Cliona Purecell<br />
Mrs Elizabeth Quinn<br />
Dr Joanne Regan<br />
Mrs Mary Ricketts<br />
Dr Mark Rockett<br />
Mrs Claire Ross<br />
Dr Satinder Sanghera<br />
Dr Ram Seereekissoon<br />
Mrs Brenda Slater<br />
Dr James Smart<br />
Mrs Karen Smith<br />
Dr Shona Smith<br />
Dr Ian Stevens<br />
Dr Ajit Sukumaran<br />
Dr Jonathan Tring<br />
Mrs Jacqueline Vasey<br />
Mrs Eva von Mantripp<br />
Dr Heather Wells<br />
Ms Felicity White<br />
Mrs Marcella Williams<br />
<strong>Pain</strong> Management Sister<br />
Nurse Specialist<br />
<strong>Pain</strong> Management Sister<br />
Consultant Anaesthetist<br />
Senior Clinical Nurse<br />
SpR Anaesthesia<br />
Acute <strong>Pain</strong> Sister<br />
Psychotherapist<br />
Sister – <strong>Pain</strong> Management<br />
Clinical Specialist<br />
Physiotherapist<br />
Clinical Nurse Specialist<br />
Clinical Psychologist<br />
Clinical Nurse Specialist<br />
Clinical Research Fellow<br />
Staff Nurse<br />
Part Time OP Principal<br />
Acute <strong>Pain</strong> Nurse<br />
Chronic <strong>Pain</strong> Sister<br />
Clinical Research Fellow<br />
RGN Bank Nurse<br />
SpR Anaesthetics<br />
Consultant Anaesthetist<br />
SpR Anaesthesia<br />
Consultant Anaesthetist<br />
Staff Nurse<br />
CNS Acute <strong>Pain</strong><br />
Clinical Psychologist<br />
Clinical Nurse Specialist<br />
Senior Nurse<br />
Gartnavel General Hopsital<br />
Charing Cross Hospital<br />
Leeds General Infirmary<br />
Western General Hospital<br />
Stirling Royal Infirmary<br />
Royal Preston Hospital<br />
Glenfield General Hospital<br />
Montagu Hospital<br />
Princess Royal Hospital<br />
Springburn Health Centre<br />
Kent & Canterbury Hospital<br />
Royal Preston Hospital<br />
Bath <strong>Pain</strong> Management<br />
Unit<br />
Royal Infirmary of<br />
Edinburgh<br />
Addenbrookes Hospital<br />
Stanhope Health Centre<br />
West Middlesex University<br />
Hospital<br />
University Hospital of<br />
Hartlepool<br />
Middlesex Hospital<br />
Nuffield Hospital<br />
Edinburgh Royal Infirmary<br />
Ipswich Hospital<br />
Blackpool Victoria Hospital<br />
Leicester Royal Infirmary<br />
Pinderfields General<br />
Hospital<br />
Singleton Hospital<br />
<strong>The</strong> Hillingdon Hopsital<br />
Hammersmith Hospital<br />
<strong>The</strong> Horder<br />
NEWS FROM PORTLAND PLACE THE PAIN SOCIETY NEWSLETTER SUMMER 2003 11
Letters to<br />
the Editor<br />
drspward@yahoo.co.uk<br />
This is the question I put to<br />
Professor Dawkins<br />
Given that chronic pain is generally<br />
pain persisting despite tissue healing<br />
and no on-going stimulation,and<br />
therefore offers very little advantage<br />
in terms of survival, what would be<br />
the explanation for the continuation<br />
of such a phenomenon in humans ?<br />
Dear Dr Ward<br />
I think it is an interesting<br />
question you raise. I don't have<br />
an authoritative answer. <strong>The</strong><br />
nearest I can approach one is as<br />
follows, and I admit that it<br />
sounds a bit lame.<br />
1. As you say, we can<br />
understand the evolution of<br />
pain when it is a guide to<br />
survival (putting your hand in<br />
the fire is bad for survival, and<br />
the pain of doing it once, warns<br />
directly against doing it again).<br />
2. Given 1, we have to ask why<br />
natural selection should 'bother'<br />
to make a distinction between<br />
pain that we can do something<br />
about (like refrain from picking<br />
up hot coals in the future) and<br />
pain that we can do nothing<br />
about (the chronic pain you are<br />
dealing with).<br />
As far as natural selection is<br />
concerned, the rule of thumb is:<br />
"Build a nervous system which<br />
feels pain whenever the tissues<br />
are damaged." Now, if natural<br />
selection were of a benevolent<br />
disposition, it might amend the<br />
rule to: "Build a nervous system<br />
which feels pain whenever the<br />
tissues are damaged, EXCEPT<br />
when there is nothing the<br />
unfortunate subject can do<br />
about it." But natural selection<br />
is, of course, not benevolent. It<br />
is indifferent to everything<br />
except reproductive success. <strong>The</strong><br />
trick to understanding this, in<br />
my view, is to switch the<br />
question from "Why should<br />
natural selection make cancer<br />
painful?" to "Why should<br />
natural selection make an<br />
exception of cancer, given that<br />
the general rule -- tissue<br />
damage = pain -- works very<br />
well?"<br />
Having said all that, I can think<br />
of reasons, other than<br />
benevolence, why natural<br />
selection might have reduced<br />
the painfulness of things like<br />
cancer.<br />
We can imagine circumstances<br />
in which reducing chronic pain<br />
might increase reproductive<br />
success. A person who is still<br />
young enough to reproduce but<br />
is suffering from cancer, might<br />
be distracted from doing so by<br />
the pain.<br />
Natural selection might<br />
therefore modify the nervous<br />
system to reduce the pain,<br />
because this would increase the<br />
chance of a child being born<br />
who bears the genetic tendency<br />
to feel less of this kind of pain.<br />
Well, I did say my attempts to<br />
answer your question might<br />
sound a bit lame!<br />
All best wishes<br />
Richard Dawkins<br />
Dear Editor<br />
I am rather surprised by the<br />
total lack of response from the<br />
<strong>Pain</strong> <strong>Society</strong> with regards to the<br />
attempt by BUPA Insurance to<br />
influence the practice of pain<br />
management by means of<br />
financial pressure. <strong>The</strong><br />
document they have recently<br />
issued with regards to<br />
management of back pain is<br />
described by them as being<br />
‘evidence based’ and if so<br />
would be highly laudable.<br />
However, of their three main<br />
advisors, one is Professor<br />
Gordon Wadell, Professor of<br />
Orthopaedic Surgery, whose<br />
antipathy towards any form of<br />
intervention with regards to<br />
back pain is well known and<br />
another is Professor Chris Main,<br />
Professor of Clinical Psychology<br />
who is one of the main<br />
proponents in this country of<br />
behavioural pain management<br />
programmes. If there were<br />
contributions from actively<br />
practising spinal orthopaedic<br />
surgeons and the <strong>Pain</strong><br />
Intervention Group of our own<br />
<strong>Society</strong> then I would have felt<br />
that their document was more<br />
balanced.<br />
I am now retiring from pain<br />
practice and therefore have no<br />
personal axe to grind but feel<br />
that this document is financially<br />
rather than scientifically based<br />
and their main ‘experts’ have<br />
produced the sort of result that<br />
is in the financial interests of<br />
the insurance societies. <strong>The</strong><br />
effects of their new policy are<br />
already being felt. I have<br />
patients whom I am able to<br />
keep mobile and at work with<br />
the occasional epidural, facet<br />
block or nerve root injection<br />
and who have already been told<br />
that cover will not be given for<br />
any further injections. Another<br />
patient was referred to me by<br />
an orthopaedic spinal surgeon<br />
with extremely severe pain<br />
which seeded to be discogenic<br />
in origin and in whom I was<br />
asked to give temporary respite<br />
with an indwelling epidural<br />
catheter for several days whilst<br />
a decision was made with<br />
regards to surgery. Cover was<br />
refused for this procedure on<br />
the grounds that ‘there was no<br />
evidence to show that it was an<br />
effective procedure’ as I was<br />
told by a non-medical member<br />
of the back pain team at BUPA.<br />
This same patient, after two<br />
spinal surgeons had agreed that<br />
spinal fusion was indicated ,<br />
was then contacted by a<br />
nursing member of the back<br />
pain team and asked whether<br />
she would consider a spinal<br />
rehabilitation programme rather<br />
than surgery. She declined this<br />
and subsequently underwent a<br />
totally successful spinal fusion.<br />
I am all in favour of the<br />
rationalisation of medical<br />
treatment but this must be<br />
through a proper peer review<br />
process and not by an insurance<br />
company with a vested interest<br />
producing a document with<br />
their main experts being people<br />
with their own particular vested<br />
interest.<br />
Yours sincerely<br />
Dr S M Berger MBBS FFARACS<br />
FANZA FRCA<br />
Manchester<br />
Dear Editor<br />
<strong>The</strong> London RCN and <strong>Pain</strong><br />
Network Forum is comprised of<br />
<strong>Pain</strong> Management Clinical<br />
Nurse Specialists, <strong>Pain</strong> Research<br />
Nurses and Senior Nurses<br />
practicing in <strong>Pain</strong> Management<br />
within the London area. We<br />
would like to register our views<br />
regarding the <strong>Pain</strong> <strong>Society</strong>'s<br />
recent publication,<br />
"Recommendations for Nursing<br />
Practice in <strong>Pain</strong> Management"<br />
As a Forum we read with<br />
interest the recommendations.<br />
This document is very<br />
comprehensive and the authors<br />
should be commended for this<br />
publication which will<br />
undoubtedly contribute to the<br />
debate on higher level practice.<br />
We would however like to share<br />
some concerns.<br />
From reading the document we<br />
feel that the working party has<br />
extended some of the standards<br />
originally intended by the NMC.<br />
Our main concern is that if<br />
12<br />
THE PAIN SOCIETY NEWSLETTER<br />
SUMMER 2003
employers interpret this<br />
document literally and assess<br />
nurses against the standards<br />
laid out in the document this<br />
could make it very difficult for<br />
nurses working in pain<br />
management to attain specialist<br />
posts or higher level practice<br />
posts.<br />
This is highlighted by the two<br />
following examples.<br />
With respect to Standard 4:<br />
Leading and Developing<br />
practice 4:2, the working party<br />
interprets this standard as;<br />
"educates own and other<br />
professionals on a local,<br />
national and/or possible<br />
international basis.... arranges<br />
local, national and possibly<br />
international study days and<br />
short courses". We would<br />
question how realistic it is for a<br />
Clinical Nurse Specialist to set<br />
up and run international study<br />
days and advise professionals<br />
on an international basis? We<br />
note from the results of the<br />
survey that 42% of acute pain<br />
teams and 31% of chronic pain<br />
teams have only one nurse. For<br />
nurses working alone it would<br />
be impossible to expect them to<br />
organise international study<br />
days and short courses. Whilst<br />
we would endorse the fact that<br />
CNS' should be involved in<br />
work at a local and even a<br />
national level, the inclusion of<br />
"International" implies nurses<br />
should also be meeting this<br />
objective in order to fulfil the<br />
Results of Glasgow ASM :<br />
sessions evaluation<br />
Average Mark<br />
Content Present’n Overall<br />
Repeat?<br />
PLENARY SESSION I: 5 4 4 128/141 (90%)<br />
Prof Herta Flor<br />
<strong>Pain</strong>, Learning & Plasticity: Results from Imaging<br />
PLENARY SESSION II: 4 4 4 121/141 (85%)<br />
Dr Lars Arendt-Nielsen<br />
Models of Muscle <strong>Pain</strong>: Experimental & Clinical…<br />
PLENARY SESSION III: 3 4 4 125/141 (88%)<br />
Dr Maureen Simmonds<br />
Assessment of Function<br />
PLENARY SESSION IV: 4 4 4 110/141 (78%)<br />
Kate Seers<br />
Implementing Evidence: Possibilities & Pitfalls….<br />
PLENARY SESSION V: 4 4 4 109/141 (77%)<br />
Dr Kenneth Craig<br />
<strong>The</strong> Faces of <strong>Pain</strong>: An Interpersonal Core<br />
PLENARY SESSION VI: 4 4 4 122/141 (86%)<br />
Dr Bill Macrae<br />
Postoperative <strong>Pain</strong>. Why Can It Become Chronic?<br />
PLENARY SESSION VII: 4 3 4 118/141 (60%)<br />
Prof. Mansel Aylward<br />
Social Policy and the Welfare System: <strong>The</strong> Challenge.<br />
PLENARY SESSION VIII: 3 3 3 85/141 (60%)<br />
Prof. Peter Reeh<br />
Inflammatory <strong>Pain</strong> Mechanisms<br />
PLENARY SESSION IX: 5 4 4 86/141 (60%)<br />
Prof. Howard L Fields<br />
Setting the Stage for <strong>Pain</strong><br />
requirement for higher level<br />
registration. Would such<br />
international ventures be<br />
expected of our medical<br />
colleagues who are practicing at<br />
Consultant level?<br />
Similarly with respect to<br />
Standard 3: Evaluation and<br />
Research 3:2, which states that,<br />
"higher level practitioners<br />
should critically appraise and<br />
synthesise the outcomes of<br />
relevant research, evaluations<br />
and audits and apply them to<br />
improve practice". <strong>The</strong> working<br />
party state that at a higher level<br />
of practice nurses working in<br />
pain management should<br />
be"....able to undertake metaanalysis<br />
and systematic reviews<br />
if warranted".<br />
Those of us who have been<br />
involved in undertaking<br />
research whilst trying to fulfill a<br />
CNS role are only too aware of<br />
the difficulties involved in this.<br />
To carry out meta-analyses or a<br />
systematic review would require<br />
considerable academic expertise<br />
and can often only be achieved<br />
if working as a full time<br />
researcher.<br />
We would very much appreciate<br />
any feedback from the working<br />
party, nursing and medical<br />
colleagues to find out whether<br />
the concerns we have noted<br />
here are shared by others.<br />
Members of the London RCN<br />
and <strong>Pain</strong> Network Forum<br />
14/11/02<br />
Content Present’n Overall Repeat?<br />
Session A – Wednesday 2 April, 14:00-15.30<br />
1. Muscle Physiology in <strong>Pain</strong> & Rehabilitation 4 4 4 10/16 (62%)<br />
2. Acute <strong>Pain</strong> Services – Can We Deliver? 4 4 4 17/24 (70%)<br />
3. <strong>Pain</strong>, War and Victims of Torture 4 4 4 12/15 (80%)<br />
4. Patient Involvement: from Leaflets to… 4 4 4 12/15 (80%)<br />
5. Chronic Abdominal <strong>Pain</strong>: Causes & Cures 4 4 4 19/25 (76%)<br />
6. Medico-legal Workshop 3 3 3 3/4 (75%)<br />
7. Psychology SIG: Changing Self-identity in… 5 5 5 10/13 (76%)<br />
8. <strong>Pain</strong> Intervention Interest SIG: Back <strong>Pain</strong>… 3 3 3 7/17 (41%)<br />
8a. <strong>Pain</strong> in Children SIG Workshop… 2 2 2 0/2 (0%)<br />
Session B – Wednesday 2 April, 16.10 – 17.40<br />
9. Neurophysiology of Phantom Limb <strong>Pain</strong> 4 5 4 16/22 (72.%)<br />
10. Patient-centred Assessment in Chronic <strong>Pain</strong> 4 4 4 10/12 (83%)<br />
11. Mechanisms of <strong>Pain</strong> 3 3 3 6/11 (54%)<br />
12. Dealing with Anger in Patients and Self… 4 5 4 6/7 (85%)<br />
13. Debate: This House Believes that Acute <strong>Pain</strong>.. 4 4 4 12/18 (66%)<br />
14. <strong>Pain</strong> and Palliative Care 4 4 4 14/20 (70%)<br />
15. <strong>Pain</strong> Management Programme SIG: Has the.. 4 4 4 14/24 (58%)<br />
16. Neuromodulation SIG: Evidence Base and… 4 4 4 2/6 (33%)<br />
Session C – Thursday 3 April 14.00 – 15.30<br />
17. <strong>The</strong> Expert Patients Programme<br />
18. Placebo in <strong>Pain</strong> 4 4 4 9/15 (60%)<br />
19. <strong>Pain</strong> in Burns 4 4 4 14/21 (66%)<br />
20. Governance in <strong>Pain</strong> Management 4 4 4 6/8 (75%)<br />
21. <strong>Pain</strong> in Children SIG Workshop: moved to 8a 4 3 3 9/16 (56%)<br />
22. Opioids for Non-cancer <strong>Pain</strong>: <strong>The</strong> New… 4 4 4 39/52 (75%)<br />
23. Clinical Information SIG: <strong>The</strong> Problems and… 3 3 3 8/13 (61%)<br />
24. DIPEx Chronic <strong>Pain</strong> – A Web-based Database. 5 5 5 2/3 (66%)<br />
25. Principles of <strong>Pain</strong> Management 5 5 5 3/3 (100%)<br />
Session D – Thursday 3 April 16.10 – 17.40<br />
26. A Revolution in Back <strong>Pain</strong> 4 4 4 22/33 (66%)<br />
27. Communicating <strong>Pain</strong> 3 3 3 7/11 63%)<br />
28. Integrating the Medical and Psychological… 4 4 4 10/12 (83%)<br />
29. How to Get Your <strong>Pain</strong> Management… 5 5 5 4/6 (66%)<br />
30. Debate: This House Believes that there is no.. 4 4 4 9/14 (64%)<br />
31. <strong>The</strong> Problem with Chronic <strong>Pain</strong> in Scotland… 4 4 4 3/3 (100%)<br />
32. Nursing Competencies in <strong>Pain</strong> Management.. 4 4 4 18/26 (69%)<br />
33. Angina SIG: Modern Management of… 4 4 4 6/7 (85%)<br />
THE PAIN SOCIETY NEWSLETTER SUMMER 2003 13
Psychological Assessment<br />
and Interventions<br />
SARAH BARKER &<br />
AMANDA C DE C WILLIAMS<br />
Having a converted cupboard<br />
for an office makes<br />
psychological consultation at<br />
our hospital a cosy affair.<br />
Despite this, a patient’s first<br />
appointment with the clinical<br />
psychologist can seem scary,<br />
associated with psychiatric<br />
labels and ‘all in the mind’<br />
statements, which mark the end<br />
of the pain being taken<br />
seriously by doctors.<br />
Psychological assessment is a<br />
real deterrent for some who<br />
don’t attend the initial meeting.<br />
But there is no avoiding this<br />
meeting for the patient wanting<br />
a spinal cord stimulator or a<br />
peripheral nerve stimulator:<br />
psychological assessment is<br />
mandatory. Many patients<br />
spend the first minutes<br />
emphasising their sanity, the<br />
reality of their pain, and their<br />
entitlement to neuromodulation<br />
to make life worth living again.<br />
<strong>The</strong> aversive and chronic nature<br />
of patients’ pain makes the<br />
hope of a cure alluring. So what<br />
does the assessment consist of,<br />
and is it really essential?<br />
Although it is widely<br />
acknowledged in the pain field<br />
that pain is a psychological<br />
experience as well as a physical<br />
one, the relationship between<br />
pain and psychological factors<br />
remains the subject of<br />
differences and debate. It would<br />
be encouraging to think that<br />
dualistic models are losing their<br />
hold, and that the attribution of<br />
pain in some patients to<br />
psychogenic factors is<br />
understood as a hypothesis not<br />
a finding, but this way of<br />
thinking still leads to<br />
stigmatisation and<br />
discrimination in many areas of<br />
health care. Although<br />
professionals working in the<br />
field of pain hopefully now have<br />
a broader perspective,<br />
misunderstandings can still<br />
occur about the role of<br />
psychology and how it can best<br />
be integrated with medical<br />
treatments.<br />
First: what requests can’t<br />
psychological assessment<br />
satisfy? It can’t establish the<br />
relative contributions of organic<br />
and psychological factors (nor<br />
can any other method, as the<br />
underlying model is erroneous),<br />
nor can it establish ‘cause and<br />
effect’ relationships between<br />
psychological problems and<br />
pain (Doleys, 2000). <strong>The</strong> other<br />
purposes for which assessment<br />
is requested is to exclude<br />
patients with gross mental<br />
health problems, which is<br />
reasonable although we do not<br />
know that they would not<br />
benefit from neuromodulatory<br />
methods; and to improve<br />
outcomes in by identifying<br />
predictors of poor outcome (e.g.<br />
North et al, 1996, Nelson et al,<br />
1996). Suggested candidates for<br />
this include ‘somatisation<br />
disorder’, ‘major uncontrolled<br />
depression/anxiety’, ‘severe<br />
sleep disturbances’, ‘serious<br />
drug or alcohol problems’ and<br />
‘lack of social support’; other<br />
factors which the psychologist is<br />
advised to consider include<br />
‘history of abuse or other<br />
dysfunction’, ‘unusual pain<br />
ratings’, ‘certain personality<br />
disorders’, ‘unresolved<br />
compensation’ and ‘lack of<br />
support from spouse’ (Olsen,<br />
1996). As you can see from this<br />
list, virtually every patient will<br />
present one or more of these<br />
‘warning’ factors.<br />
While the search for predictors<br />
of outcome seems at first a<br />
reasonable scientific pursuit, it<br />
does not stand up to scrutiny.<br />
<strong>The</strong> only way to discover such<br />
predictors would be to assess<br />
all patients, to treat them all<br />
blind to the assessment process,<br />
and then to compare the<br />
outcome with those<br />
assessments. Instead, lists of<br />
problems such as those above<br />
are used to be very selective<br />
about candidates for<br />
neuromodulation, so that if any<br />
predictors are found<br />
retrospectively, they can only<br />
apply within the limits of those<br />
selection procedures, which of<br />
course vary from clinic to clinic.<br />
<strong>The</strong>se exclusion criteria easily<br />
become proxies for refusing<br />
patients who are already<br />
underserved and disadvantaged.<br />
A close look at the literature on<br />
psychological screening for<br />
neuromodulation shows<br />
generally poor methodologies<br />
and a strong influence from<br />
insurance based health funding<br />
which characteristically focuses<br />
on shortcomings in the<br />
patient/claimant.<br />
Given the unpredictable success<br />
of neuromodulation and the<br />
distress caused by pain and<br />
unsuccessful treatment, what<br />
should psychological screening<br />
aim to achieve? <strong>The</strong>re is<br />
certainly benefit in eliciting<br />
patients’ understanding (or<br />
misunderstanding) both of their<br />
pain problem and of<br />
neuromodulation procedures<br />
14<br />
THE PAIN SOCIETY NEWSLETTER<br />
SUMMER 2003<br />
FEATURES
and effects, and various<br />
members of the team contribute<br />
to rectifying such<br />
misunderstandings. But<br />
arguably we could be following<br />
through the multidimensional<br />
model of pain with strategies in<br />
various dimensions, not only<br />
neuromodulation. <strong>The</strong><br />
psychological interview can be a<br />
chance to introduce the patient<br />
to pain management principles<br />
and practices which are<br />
compatible with invasive<br />
treatments. At present,<br />
organisation of services and<br />
referral patterns often<br />
instantiates the separation<br />
between physical and<br />
psychological which many pain<br />
clinicians try so hard to<br />
integrate.<br />
In areas such as psychiatric<br />
rehabilitation and cystic fibrosis,<br />
a multicomponent care plan is<br />
used to plan treatment over a<br />
particular time span. <strong>The</strong><br />
patient and those close to him<br />
or her take a major part in<br />
discussion and decisions while<br />
the various health professionals<br />
involved meet briefly with them<br />
to consider their various health<br />
needs, from physical treatments<br />
to social support. This produces<br />
a treatment plan with actions<br />
assigned to particular<br />
professionals, and a copy held<br />
by the patient. It then forms the<br />
basis of reviews and outcome<br />
assessment. Applied to<br />
persistent pain, this would<br />
enable physiotherapy,<br />
occupational therapy and<br />
psychology to be strategically<br />
planned alongside<br />
pharmacological and invasive<br />
treatments. For a psychologist it<br />
would offer the chance to work<br />
on a patient’s depression, fears<br />
about procedures, and problem<br />
solving in the context of other<br />
treatments, and for the patient<br />
is of far more value than a stack<br />
of questionnaires and possible<br />
refusal of neuromodulation on<br />
obscure psychological grounds.<br />
References<br />
Banks, SM and Kerns, RD (1996).<br />
Explaining high rates of depression in<br />
chronic pain: a diathesis-stress framework.<br />
Psychol. Bull. 199, 95-110.<br />
Doleys, D.M. (2000). Psychological<br />
assessment for implantable therapies.<br />
<strong>Pain</strong> Digest, 10, 16-23.<br />
Melzak, R. and Wall, P. (1988). <strong>The</strong><br />
Challenge of <strong>Pain</strong>. London: Penguin.<br />
Nelson, DV et al (1996).<br />
Psychological selection criteria for<br />
implantable spinal cord stimulations.<br />
<strong>Pain</strong> Forum 5(2), 93-103.<br />
North, RB; et al (1996). Prognostic<br />
value of psychological testing in<br />
patients undergoing spinal cord stimulation:<br />
a prospective study.<br />
Neurosurg 39 (2), 309-11<br />
Olsen (1996). <strong>The</strong> value of multiple<br />
sources of data in decision making.<br />
<strong>Pain</strong> Forum 5(2), 104-6.<br />
A Distress Motivation Axis<br />
A simple axis diagram was developed for the new patient<br />
assessment form in the pain clinic. <strong>The</strong> clinician ticks the quadrant<br />
they perceive best matches the patients mental state. Its aim is to<br />
serve as a reminder for the clinician at a subsequent consultation as<br />
to whether they elicited, or the patient expressed, distress relating to<br />
their pain and personal situation and how ready the patient<br />
appeared to be to adopt selfmanagement principles. It appears to be<br />
useful but is limited by the fact that the patients may have changed<br />
their attitudes and beliefs after the first consultation. It is also only a<br />
record of a clinical impression and is not patient centred. <strong>The</strong><br />
concepts behind the axis are not original; both 'psychological<br />
distress' (1) and 'readiness to change'(2) can be elicited by using<br />
patient self rating instruments in addition to patient interview.<br />
(1) Main C J, Wood P L R, Hollis S, Spanswick C C, Waddell G. <strong>The</strong><br />
distress and risk assessment method. A simple classification to<br />
identify distress and evaluate the risk of poor outcome. Spine, 1992;<br />
17(l):4252<br />
(2) Kems R D, Roseriher. R et al. Readiness to adopt a<br />
selfmanagement approach to chronic pain : the <strong>Pain</strong> Stages of<br />
Change Questionnaire. <strong>Pain</strong>, 1997 ; 72: 234 237<br />
Douglas Natusch - Consultant Anaesthetist<br />
<strong>Pain</strong> Management Offices, Torbay Hospital, Lawes Bridge, Torquay.<br />
TQ27AA<br />
FEATURES THE PAIN SOCIETY NEWSLETTER SUMMER 2003 15
SIGS<br />
Special Interest Groups<br />
Any group of 30 or more full members of the <strong>Pain</strong><br />
<strong>Society</strong> may form a Special Interest Group of the <strong>Society</strong>.<br />
Such a group must apply in writing to the Council for<br />
recognition.<br />
Such an application must provide:<br />
1. <strong>The</strong> name of the special interest group (SIG).<br />
2. A description of the proposed activities and scientific<br />
focus.<br />
3. <strong>The</strong> names, signatures and <strong>Pain</strong> <strong>Society</strong> membership<br />
numbers of the founding members.<br />
To be approved by the <strong>Society</strong> it is expected<br />
that:<br />
1. All members will be members of the <strong>Pain</strong> <strong>Society</strong>.<br />
2. <strong>The</strong> group will be multidisciplinary.<br />
3. <strong>The</strong> interest will be within one subject area.<br />
4. <strong>The</strong> membership will be open to all members of the<br />
<strong>Pain</strong> <strong>Society</strong>.<br />
<strong>The</strong> SIG will be expected to:<br />
1. Submit an annual report to the <strong>Society</strong> describing<br />
meetings held, financial affairs, list of members and<br />
other matters as deemed appropriate.<br />
2. May submit proposals to Council for subjects and<br />
speakers for <strong>Society</strong> meetings.<br />
3. May adopt bylaws and operating procedures for<br />
regulation of their affairs providing they do not conflict<br />
with the ordinances and constitution of the <strong>Pain</strong><br />
<strong>Society</strong>.<br />
4. May elect their own officers using the principle of one<br />
vote per member and may charge dues to their<br />
members.<br />
5. May hold scientific or professional meetings provided<br />
that these are organised and financed by the SIG. Such<br />
meetings must be open to all members of the <strong>Pain</strong><br />
<strong>Society</strong> on a space available basis and must not<br />
conflict with the three day Annual Meeting of the<br />
<strong>Society</strong>. However, it will be permissible to hold such a<br />
meeting immediately preceding or post the annual<br />
meeting.<br />
6. Details of the SIGs and their officers will be listed in<br />
the biannual handbook of the <strong>Society</strong>.<br />
7. SIGs will be permitted to use the <strong>Society</strong> mailing lists<br />
and facilities to publicise forthcoming meetings or<br />
events.<br />
SIGs meet annually with the Officers of the <strong>Pain</strong> <strong>Society</strong>.<br />
Special Interest Group:<br />
<strong>Pain</strong> in Children<br />
<strong>The</strong> Special Interest Group: <strong>Pain</strong><br />
in Children would like to extend<br />
sincere thanks to Dr. Martin<br />
Ward Platt and Ms. Zoe Sully, as<br />
outgoing Chair and Secretary of<br />
the group for all their time and<br />
enthusiasm expended over the<br />
last few years in leading the<br />
group.<br />
It is now accepted that pain<br />
should be anticipated, and<br />
safely and effectively controlled,<br />
in all children, whatever their<br />
age, maturity or severity of<br />
illness (Fisher & Morton 1998).<br />
<strong>The</strong> Audit Commission (1993)<br />
identifies pain prevention as<br />
one of ten indicators of quality<br />
of care in its report on children’s<br />
care in hospital.<br />
<strong>The</strong> SIG has the following aims:<br />
• To improve the<br />
identification, prevention<br />
and management of pain in<br />
children.<br />
• To promote multidisciplinary<br />
collaboration in paediatric<br />
pain management.<br />
• To encourage education and<br />
research in paediatric pain.<br />
• To provide a focus within<br />
the <strong>Pain</strong> <strong>Society</strong> for matters<br />
relating to pain in children.<br />
<strong>The</strong> management of acute,<br />
chronic and palliative paediatric<br />
pain remains complex. Within<br />
the diverse paediatric<br />
population the goal to deliver<br />
optimal pain management can<br />
often encompass all three<br />
components, whether in the<br />
postoperative period, the<br />
chronic trajectory or at the end<br />
stages of a child’s life.<br />
Acute pain management for the<br />
majority of children is now<br />
widely recognised and delivered<br />
effectively and safely.<br />
Early identification and<br />
management of chronic<br />
paediatric pain has been less<br />
successful and there are only a<br />
16<br />
THE PAIN SOCIETY NEWSLETTER<br />
SUMMER 2003<br />
SIGS
handful of centres resourced to<br />
manage it. <strong>The</strong>re is a distinct<br />
lack of guidelines. <strong>The</strong>re can be<br />
difficulty in recognising nonopioid<br />
responsive pain and<br />
adolescent society appears to<br />
particularly suffer from problems<br />
in accessing appropriate and<br />
individually titrated treatments.<br />
<strong>The</strong> importance of palliative<br />
pain management in children<br />
also requires emphasis,<br />
paediatric pain specialists can<br />
often be based in acute Trusts<br />
and children at end stage of life<br />
may frequently be cared for in<br />
the community. All community<br />
staff should have the<br />
opportunity to easily access<br />
support, advice and education<br />
regarding the most effective<br />
methods of analgesia for these<br />
patients at what can potentially<br />
be an extremely distressing time<br />
for family and staff.<br />
<strong>The</strong> SIG would like to invite <strong>Pain</strong><br />
<strong>Society</strong> members to consider<br />
methods of raising the profile of<br />
all components of paediatric<br />
pain management. Perhaps your<br />
centre would like to propose a<br />
member as a named contact for<br />
children’s pain management?<br />
Requests have also been sent to<br />
all SIG members for suggestions<br />
to the group on taking this area<br />
forward. Current suggestions<br />
that have been submitted are:<br />
the development of a national<br />
guideline on paediatric pain<br />
management using SIGN or the<br />
Cochrane Methodology; the<br />
development and collation of<br />
educational material for the<br />
child and family regarding all<br />
aspects of pain assessment and<br />
management and the proposal<br />
of a model of service and<br />
standards of care for children<br />
with complex persistent pain –<br />
with an observation by the<br />
group member that the Clinical<br />
Standards Advisory Group<br />
Report on <strong>Pain</strong> Services (1998)<br />
only briefly mentioned children<br />
with chronic pain.<br />
Any suggestions would be<br />
warmly welcomed. Thank you in<br />
anticipation.<br />
Mrs.Susan Aitkenhead<br />
Chair, SIG: <strong>Pain</strong> in Children.<br />
References:<br />
Audit Commission (1993)<br />
Children First: A Study of<br />
Hospital Services. London:<br />
HMSO.<br />
Clinical Standards Advisory Group<br />
(1998) Services for Patients with<br />
<strong>Pain</strong>. London: Stationary Office<br />
Books.<br />
Fisher S & Morton NS (1998) <strong>Pain</strong><br />
Prevention and Management in<br />
Children. In: Morton NS (Ed)<br />
Acute Paediatric <strong>Pain</strong><br />
Management: A Practical Guide.<br />
WB Saunders.<br />
Contact:<br />
Mrs. Susan Aitkenhead<br />
Consultant Nurse in Paediatric<br />
<strong>Pain</strong> Management<br />
<strong>The</strong> <strong>Pain</strong> Management Service<br />
<strong>The</strong> Royal Hospital for Sick<br />
Children<br />
Glasgow G3 8SJ<br />
Tel: 0141 201 0186<br />
E-mail:<br />
susan.aitkenhead@yorkhill.scot.nh<br />
s.uk<br />
SIGs and their Chairmen :<br />
Acute <strong>Pain</strong> Special Interest Group<br />
(APSIG)<br />
Dr D Counsell<br />
Tel: 01978 291 100<br />
Angina Special Interest Group<br />
Dr M Chester<br />
Tel: 0151 228 1616<br />
SIGS<br />
Special Interest Groups<br />
Clinical Information Special Interest<br />
Group (CISIG)<br />
Dr C Price<br />
Tel: 02380 796135<br />
<strong>Pain</strong> Intervention Interest Group (PIIG)<br />
Dr A Lawson<br />
Tel: 020 8746 8026<br />
<strong>Pain</strong> Management Programmes Group<br />
Dr G Cavill<br />
Tel: 01670 529 540<br />
Psychology and <strong>Pain</strong> Special Interest<br />
Group<br />
Dr C Eccleston<br />
Tel: 01225 826439<br />
<strong>Pain</strong> in Children Special Interest Group<br />
Mrs S Aitkenhead<br />
Tel: 0141 201 0186<br />
Neuromodulation Special Interest Group<br />
Dr D Dickson<br />
Tel: 0113 392 4682<br />
Neuropathic Special Interest Group<br />
Dr D Bowsher<br />
Tel: 0151 523 1486<br />
<strong>The</strong> University of Sydney <strong>Pain</strong> Management Research Institute offers a Graduate Certificate,Graduate Diploma and Masters in Science or Medicine (<strong>Pain</strong> Management) for students seeking to further their knowledge and<br />
skills in pain medicine.Students may also elect to study single non-award subjects.<strong>The</strong> Program is multidisciplinary and available to medical,dental and allied health professionals with an interest in pain management.<strong>The</strong><br />
curriculum includes modules on pain concepts,pain neurobiology,pharmacology and clinical aspects such as pain in children,pain in older people,musculoskeletal pain,cancer pain and psychological approaches to pain<br />
management.<strong>The</strong> Program has now been running for 7 years and over 150 students have enrolled,including 28 international students from 14 different countries.<strong>The</strong> Program has two student intakes,one commencing in<br />
March and one in July.All components of the Program including study guides,materials and discussion groups are accessed on-line and are therefore available worldwide.<strong>The</strong> Program has a two week face to face component<br />
but this is optional and the requirements for the degrees can all be completed by distance.<br />
For further details of the Program including curriculum,admission requirements,course fees and scholarships,please visit the Program website at:www.painmgmt.usyd.edu.au/html/domdip6.html.<br />
Information can also be obtained from the administrative assistant Ros Wyllie,Tel:+61 2 9926 7386;Fax:+ 61 2 9926 6780,or email:rwyllie@med.usyd.edu.au.<br />
SIGS THE PAIN SOCIETY NEWSLETTER SUMMER 2003 17
Angina<br />
Pectoris :<br />
A Historical<br />
Perspective<br />
AUSTIN LEACH<br />
Since the beginning of recorded<br />
history mankind has<br />
differentiated between visceral<br />
and superficial (somatic) pain.<br />
From examination of<br />
archaeological relics and<br />
modern day primitive cultures, it<br />
seems clear that pain was<br />
regarded as being due to<br />
external forces. For superficial<br />
pain, these external forces were<br />
usually obvious, such as an<br />
accidental injury, but deep or<br />
internal, pains, which had no<br />
readily identifiable source, were<br />
attributed to metaphysical<br />
causes such as evil spirits or<br />
curses.<br />
<strong>The</strong> traditional medicine<br />
practiced by the Chinese for<br />
4500 years describes how the<br />
balance of vital energy or ch'i is<br />
maintained by its flow through<br />
a network of conduits or<br />
meridians which are connected<br />
to visceral structures or organ<br />
function. If there develops an<br />
imbalance between the two<br />
opposing forces of Yin and<br />
Yang, disease and pain result.<br />
This is due to an obstruction<br />
(deficiency) or outpouring<br />
(excess) in the circulation of<br />
ch'i. Thus the Chinese were able<br />
to link pathology in visceral<br />
structures with pathology in<br />
somatic structures, and also link<br />
abnormal sensation in one site<br />
with abnormal sensation in<br />
another.<br />
Western thinking is linked<br />
strongly to the ancient Greek<br />
philosophies. Plato felt that<br />
sensation in humans was<br />
processed by the heart and the<br />
liver, which communicated with<br />
the rest of the body by the<br />
movement of atoms through<br />
communicating veins. (Not that<br />
different, if slightly less<br />
sophisticated, from the Chinese<br />
notions). In De Anima Aristotle<br />
wrote that the centre of<br />
perception was in the heart.<br />
<strong>Pain</strong> was felt in the heart as a<br />
"quale", a passion of the soul,<br />
and a sensation or experience<br />
opposite to pleasure, the<br />
epitome of unpleasantness. This,<br />
in essence, is how we describe<br />
the affective quality of pain<br />
today. Aristotle also described<br />
pain as being an excess in any<br />
of the five sensations. All five<br />
senses, vision, taste, smell,<br />
hearing and touch arose in the<br />
end organs of the flesh and<br />
were conveyed by blood to the<br />
heart. <strong>Pain</strong> was thus regarded<br />
as an intensityrelated<br />
phenomenon.<br />
Nearly 2000 years passed<br />
before this concept was<br />
seriously challenged. In 1628<br />
William Harvey examined the<br />
exposed heart of the young<br />
Viscount Montgomery, who had<br />
earlier suffered a chest injury<br />
following a riding accident and<br />
had a well healed defect<br />
opening into his pericardium.<br />
Harvey touched, pinched and<br />
pricked the surface of the heart,<br />
after which he concluded that<br />
the heart was insensate. In<br />
1664 Descartes published his<br />
book L'homme, in which he<br />
suggested that sensation was<br />
transmitted centrally along<br />
nerves, which caused an<br />
opening of pores in the brain<br />
resulting in sensation. This<br />
concept is an early suggestion<br />
of specificity theory.<br />
A century later Heberden is<br />
credited with adopting the term<br />
angina pectoris ("strangling of<br />
the chest") in an address to the<br />
Royal College of Physicians in<br />
1768, although his descriptions<br />
of angina, angor animi (anguish<br />
and mortal fear associated with<br />
angina) and its relation to<br />
physical exertion were not<br />
published until 1772.<br />
Between 1890 and 1925<br />
intense interest surged around<br />
the functionings of the nervous<br />
system, the perception of pain<br />
and the differences between<br />
visceral and somatic pain. It<br />
seems that the experiences of<br />
the workers a century ago were<br />
little different to the frustrations<br />
encountered today:"...I had<br />
become so deeply interested in<br />
the line of research I had<br />
pursued for years that I fancied<br />
I had been making a<br />
considerable advance. But ..<br />
doubts began to arise in my<br />
mind as to the sufficiencies of<br />
the researches that had been<br />
made ... by myself and others ...<br />
It became evident that,<br />
notwithstanding the new<br />
phenomena that were being<br />
brought to light .. no progress<br />
was being made towards<br />
attaining the great object of all<br />
our undertakings."<br />
Sir James Mackenzie "Diseases<br />
of the Heart" 1925 Preface to<br />
4th edn.<br />
Two schools of thought<br />
prevailed during this period, and<br />
intense debate sprang up<br />
between the protagonists of<br />
each body of opinion. <strong>The</strong> link<br />
between coronary vessel<br />
atheroma and cardiac pain had<br />
been well established by this<br />
time, but the mechanisms<br />
linking ischaemia and pain<br />
generation were more tenuous.<br />
Most interest centred on the<br />
observations of exercise induced<br />
intermittent claudication and,<br />
having established that muscle<br />
could be a primary source of<br />
pain, attempted to extrapolate<br />
these findings to events in the<br />
ischaemic myocardium.<br />
<strong>The</strong> observation that viscera are<br />
insensate led to an alternative<br />
hypothesis, namely that cardiac<br />
pain was generated primarily by<br />
an abnormal excitability in the<br />
nervous system. This was<br />
supported by the appearance of<br />
cutaneous and subcutaneous<br />
hyperalgesia in association with<br />
angina pectoris. This led to the<br />
adoption of the term 'cardiac<br />
neurasthenia', a vague term<br />
encapsulating the concept of<br />
the CNS becoming<br />
hypersensitive so that a<br />
previously trivial sensory input<br />
from the organ in question,<br />
which would hitherto be below<br />
a perceptual threshold,<br />
somehow gets translated into a<br />
painful stimulus. Extremely<br />
elaborate charts of the nervous<br />
connections of the heart were<br />
produced following meticulous<br />
anatomical dissections in an<br />
attempt to define macroscopic<br />
links between the various parts<br />
of the sympathetic chain and<br />
spinal cord. <strong>The</strong> reporting of<br />
cutaneous hyperalgesia and<br />
subcutaneous tenderness is a<br />
commonly recurring theme. In<br />
the days before sophisticated<br />
monitoring detailed<br />
examination formed the basis<br />
for much medical theory and it<br />
is difficult to believe that so<br />
many distinguished clinicians<br />
were making a truly spurious<br />
observation. It seems more<br />
likely that this potentially<br />
important clinical finding has<br />
been forgotten.<br />
Against the neurasthenia<br />
hypothesis were ranged such<br />
worthy opinions as Colbeck's,<br />
who stated in the Lancet in<br />
1903: "the rarity of its<br />
occurrence among women are<br />
features opposed to the purely<br />
nervous theory of its mode of<br />
production. "<br />
<strong>The</strong> inability to match pathology<br />
with symptoms, which persists<br />
to this day, led to Mackenzie<br />
postulating "...two forms of<br />
cardiac pain ... produced in<br />
different ways which have a<br />
significance of a widely different<br />
kind. One form is associated<br />
with actual disease of the heart.<br />
This should be called 'primary<br />
angina pectoris'. In the other<br />
18<br />
THE PAIN SOCIETY NEWSLETTER<br />
SUMMER 2003<br />
FEATURES
form there is no disease of the<br />
heart, the symptoms being<br />
referable to a hypersensitive<br />
central nervous system. This<br />
form I call 'secondary angina<br />
pectoris'."<br />
It seems that in certain aspects<br />
of medicine nothing changes.<br />
One of the most widely<br />
discussed themes in the old<br />
textbooks is whether or not<br />
angina pectoris is a disease<br />
entity in its own right, or a<br />
symptom; in other words a<br />
manifestation common to<br />
several distinctly separate<br />
disease processes. If modern<br />
medical writing is often accused<br />
of being dry, I would refer<br />
interested parties to the<br />
relevant chapter in Albutt's<br />
book Diseases of the Arteries<br />
including Angina Pectoris<br />
published in 1915. <strong>The</strong>se nine<br />
turgid pages (pp211-220),<br />
densely printed in eight point,<br />
debate the differences between<br />
the definitions of symptoms,<br />
syndromes and diseases and<br />
conclude: "... if the title of<br />
angina pectoris be used to<br />
include a variety of symptom<br />
groups which, although they<br />
may present a superficial clinical<br />
resemblance, yet in their<br />
aetiological and pathological<br />
relations differ widely and<br />
fundamentally, all definite use<br />
of names comes to an end "<br />
Relying on case reports and<br />
clinical observational<br />
associations clearly had its<br />
drawbacks, and contributed to<br />
the frustrations and inaccuracies<br />
of the day. Albutt continues<br />
(describing his trawl through<br />
the literature): "...surely it is<br />
levity to confuse the squalls of<br />
unstable neurotics, mostly<br />
women, with the assault of one<br />
of the fiercest and most<br />
searching afflictions which can<br />
fall upon steadfast and resolute<br />
men ... Could professorial<br />
pedantry be more extravagant!<br />
unless, indeed, it be surpassed<br />
by a comparison of the pain of<br />
angina with that of colic, of<br />
hysteralgia or of heartburn! But<br />
the most egregious example of<br />
this eccentricity which I have<br />
noted is the description, by a<br />
well known modern physician,<br />
of a case of angina pectoris<br />
originating in the clitoris.<br />
"However, some workers had<br />
useful insight: "Sir James Barr<br />
thinks that in angina the heart<br />
has too much (sic) calcium<br />
ions... " which could be taken<br />
to predict the value of calcium<br />
channel blocking drugs in<br />
angina.<br />
In the late 1920's the debate<br />
regarding angina's aetiology<br />
appears to come to an abrupt<br />
halt, and, for no clear reason,<br />
comes down on the side of the<br />
"primary angina" side of the<br />
fence. Since then, it has become<br />
enshrined as a piece of medical<br />
dogma that the pain of angina<br />
pectoris is a warning that<br />
myocardium threatening<br />
ischaemia looms. This has been<br />
the understanding for several<br />
generations of doctors, and<br />
therefore patients, but the<br />
evidence to support this<br />
hypothesis remains as patchy as<br />
it was seventy five years ago.<br />
<strong>The</strong> available treatments of that<br />
time are still part of the<br />
therapeutic framework of today.<br />
Atropine, amyl nitrite,<br />
nitroglycerine and morphine<br />
were popular and widely used<br />
drugs; one Dr Dieulafoy<br />
recommended aspirin, in a dose<br />
of 500 mg every two hours.<br />
Remedies used less often today<br />
are such preparations as sodium<br />
and potassium iodide, strontium<br />
bromide, peppermint ("Once<br />
break the wind, they say, and<br />
the attack is relieved'), arsenic<br />
(syphilitic aortitis was a<br />
common cause of coronary<br />
disease) and high frequency<br />
electrical current, delivered via a<br />
sulphur bath. In terms of<br />
prevention the importance of<br />
diet and rest was stressed.<br />
Vigorous exercise was regarded<br />
as dangerous.<br />
Surgical treatments at this time<br />
were confined to extracardiac<br />
procedures carried out by a<br />
minority of enthusiasts. In 1880<br />
Langer noted that numerous<br />
minute vascular connections<br />
existed between coronary<br />
vessels and surrounding<br />
structures such as diaphragm,<br />
bronchi and pericardium. This<br />
paved the way for attempts at<br />
indirect revascularisation.<br />
Procedures such as pericardial<br />
poudrage (direct surgical<br />
irritation by abrasion and<br />
instillation of talc into the<br />
pericardium) achieved some<br />
popularity. In anticipation of the<br />
increasingly discredited modern<br />
day transmyocardial laser<br />
"revascularisation" (TMLR)<br />
there are descriptions of<br />
myocardial perforation with<br />
acupuncture needles in an<br />
attempt to stimulate<br />
neovascularisation. However,<br />
until the 1930's, most surgical<br />
procedures centred on the<br />
cardiac nerve supply. <strong>The</strong> first<br />
human cardiac sympathectomy<br />
was carried out by Jonnesco in<br />
1916. This was reasonably<br />
effective in relieving the<br />
sensation of angina, but was<br />
also believed to produce<br />
coronary vasodilation.<br />
Sympathectomy was achieved<br />
by surgical extirpation or<br />
injection of neurotoxic<br />
substances such as ethanol.<br />
Success for this procedure was<br />
reasonably good, though there<br />
was a significant complication<br />
rate. Neuropathic pain or even<br />
paralysis could occur, although<br />
the mortality rate of 510%<br />
probably reflects the belief that<br />
removing “Nature's warning”<br />
was dangerous, and palliative<br />
surgical sympathectomy was<br />
reserved for the most extreme<br />
of circumstances. Only patients<br />
with apparent end stage<br />
coronary disease and impending<br />
heart failure would be offered<br />
this treatment and techniques<br />
of anaesthesia and<br />
understanding of cardiovascular<br />
physiology were less well<br />
developed than nowadays.<br />
Enthusiasts continued<br />
denervation until the 1960's but<br />
the development of<br />
extracorporeal oxygenation and<br />
direct revascularisation of the<br />
myocardium led to<br />
sympathectomy's fall from<br />
grace.<br />
Since then, all efforts have<br />
concentrated on developing<br />
more sophisticated (for which<br />
read expensive!) and less<br />
dangerous methods of<br />
increasing the calibre of the first<br />
ten inches or so of the<br />
epicardial arteries. This appears<br />
to have resulted in a serious<br />
neglect of the other part of the<br />
equation: namely, how cardiac<br />
signalling is translated into the<br />
perception of pain, and how<br />
those signals are handled by<br />
the central nervous system once<br />
they arrive. It is well known that<br />
there is no correlation between<br />
stimulus intensity (degree of<br />
ischaemia) and stimulus<br />
perception (what the sufferer<br />
feels). Approximately one third<br />
of myocardial infarctions are<br />
silent, i.e. painless. <strong>The</strong><br />
speculations and debates of the<br />
early twentieth century<br />
regarding the nature of angina,<br />
and other visceral pain<br />
syndromes, deserve to be<br />
resurrected. With new expertise<br />
available to us using<br />
sophisticated imaging<br />
techniques, improved<br />
understanding of such matters<br />
as genetic expression and<br />
neural biochemistry, we may yet<br />
get much closer to truly<br />
understanding one of Nature's<br />
remaining conundrums.<br />
Austin Leach<br />
National Refractory Angina<br />
Centre, Liverpool UK<br />
May 2003<br />
FEATURES<br />
THE PAIN SOCIETY NEWSLETTER SUMMER 2003 19
Nottingham <strong>Pain</strong> Clinic survey<br />
What do GPs’ want from the pain<br />
clinic and do we provide it?<br />
<strong>The</strong> pain department at City Hospital provides a one-day series of<br />
lectures and practical workshops for local GPs.<br />
49 GP’s attended the pain day and 35 returned completed the<br />
questionnaire. <strong>The</strong> response rate was 71%.<br />
Demographic data<br />
Mean Range<br />
Number of partners 5 1-14<br />
List size 8000 1800-34000<br />
Which one of the following statements best describes the<br />
way that you would like the pain clinic to be organised?<br />
(Tick one option)<br />
1- More new patient appointments with a short follow up period<br />
and discharge back to GP care.<br />
2- More new patient appointments with a treatment plan that is<br />
carried out and maintained by the GP. No routine follow up in the<br />
pain clinic.<br />
3- Fewer new patient appointments with long term follow up by the<br />
pain clinic.<br />
Option 1 70%<br />
Communication<br />
12 training practices and 22 non-training practices were represented.<br />
Organisational issues<br />
A number of participants were from outside Nottingham so gave<br />
responses related to experience with their local provider of pain<br />
services.<br />
How long do<br />
your patients<br />
have to wait<br />
for a routine<br />
pain clinic<br />
appointment?<br />
0-4 Weeks - 23%<br />
Do you expect<br />
to receive a<br />
letter after<br />
each<br />
outpatient<br />
episode in the<br />
pain clinic?<br />
How often<br />
does this<br />
happen?<br />
No - 20%<br />
Always - 6%<br />
Yes - 80%<br />
Mostly - 51%<br />
1-3 Months - 54%<br />
Rarely - 11%<br />
0-4 Weeks - 17%<br />
What do you<br />
think is an<br />
acceptable<br />
waiting time<br />
for a routine<br />
pain clinic<br />
appointment?<br />
1-3 Months - 74%<br />
Sometimes - 11%<br />
How long does it take for a letter to arrive at your practice<br />
after the<br />
4-6 weeks - 11%<br />
patients’ pain<br />
0-2 weeks - 14%<br />
clinic<br />
consultation?<br />
In order to reduce the waiting time for a new patient<br />
routine appointment at the pain clinic it would be<br />
necessary to reduce the number of follow up appointments.<br />
How would<br />
Acceptable - 46%<br />
you rate this<br />
Excellent - 17%<br />
change?<br />
2-4 weeks - 54%<br />
Comments<br />
“A brief letter with a treatment plan is all that is needed.”<br />
“<strong>The</strong> letters are very important because chronic pain patients are<br />
very demanding and frequent attendees who always want<br />
information from the hospital.”<br />
Good - 31%<br />
20<br />
THE PAIN SOCIETY NEWSLETTER<br />
SUMMER 2003<br />
FEATURES
Have you ever<br />
tried to phone<br />
a pain<br />
Consultant for<br />
telephone<br />
advice?<br />
No - 71%<br />
Yes - 26%<br />
A 30-year-old<br />
male with a 12-<br />
week history of<br />
acute back pain<br />
following a<br />
lifting injury who<br />
has had 2 weeks<br />
off work.<br />
<strong>The</strong> 50 year old - 63%<br />
Both - 23%<br />
Why did you<br />
not phone?<br />
You did not want to be kept on hold<br />
for ages by switchboard - 24%<br />
You did not need<br />
advice - 28%<br />
A 50-year-old<br />
male with a 20-<br />
<strong>The</strong> 30 year old - 9% Neither - 6%<br />
year history of progressively increasing back pain that has caused<br />
him to take early retirement.<br />
Comments<br />
“It would be helpful to have a direct line number and a time period<br />
when GP’s could telephone a Consultant for advice about a patient,<br />
especially to prevent a referral.”<br />
How satisfied<br />
are you with<br />
the advice that<br />
you receive<br />
from the<br />
Consultants at<br />
the pain clinic?<br />
You didn’t think that advice would be forthcoming<br />
because the Consultant was busy or unobtainable - 32%<br />
Fair - 34%<br />
Poor - 6%<br />
<strong>The</strong> role of<br />
the pain clinic<br />
Rank the following in order of importance for a pain<br />
service: (where 1 is the most important and 8 is the least<br />
important)<br />
1st Multidisciplinary approach by a large margin<br />
2nd Psychological assessment<br />
3rd <strong>Pain</strong> management program<br />
4th Nerve blocks<br />
5th TENS service<br />
6th Acupuncture service<br />
7th Highly specialised techniques<br />
8th Massage and relaxation therapy<br />
<strong>The</strong> 2nd and 3rd choices were almost equally popular and then there<br />
was a gap before 4th, 5th and 6th choices, which were almost<br />
equally popular. <strong>The</strong> 7th and 8th choices were a lot less popular<br />
compared with other options.<br />
Comments<br />
“TENS and Acupuncture direct GP access”<br />
“TENS and Acupuncture provided by the PCT”<br />
Very good - 6%<br />
Good - 46%<br />
Which of these patients would be appropriate to refer to a<br />
chronic pain clinic?<br />
A 40-year-old,<br />
otherwise fit<br />
gentleman, is<br />
started on<br />
MST to relieve<br />
back pain. He<br />
is discharged<br />
from clinic<br />
because he<br />
has exhausted<br />
all other<br />
Yes<br />
for a short time<br />
- 37%<br />
Yes<br />
indefinitely<br />
- 60%<br />
No - 3%<br />
treatment modalities. Would you be happy to continue his<br />
care whilst on MST for non-malignant pain?<br />
Conclusions<br />
Over 75% of patients referred to clinic were seen within 3 months<br />
and this was deemed acceptable by 75% of GPs’ who responded.<br />
Many GPs would accept fewer follow-up appointments if this<br />
resulted in more new appointments with a shorter waiting time.<br />
It was a surprise that 20% of GPs did not consider a letter to be<br />
desirable after an outpatient appointment. Those who did want a<br />
letter wanted it to include a treatment plan and be brief.<br />
<strong>The</strong> telephone advice line did not appear to be a popular option<br />
although more than 50% of GPs considered advice from the pain<br />
clinic to be of good quality.<br />
<strong>The</strong> multidisciplinary approach was considered to be the most<br />
important feature of the pain clinic although access to a pain<br />
management program was highly sought after.<br />
A number of GPs would like direct access to TENS and acupuncture<br />
clinics and would like their PCTs to provide these services<br />
independently of the acute trusts.<br />
A good proportion of GPs seemed happy to prescribe opioids for<br />
non-malignant pain although this question requires further<br />
examination.<br />
Reference:<br />
Clarke Leo. What does a GP want from a pain clinic? <strong>The</strong> Exeter Audit.<br />
<strong>The</strong> <strong>Pain</strong> <strong>Society</strong> newsletter. Winter 199/2000; Volume 1: 8-9.<br />
Authors : Dr. Richard J Faleiro - <strong>Pain</strong> Fellow and SpR<br />
Anaesthetics City Hospital Nottingham. Dr Andrew Ravenscroft<br />
Consultant <strong>Pain</strong> Anaesthetist City Hospital Nottingham.<br />
FEATURES THE PAIN SOCIETY NEWSLETTER SUMMER 2003 21
Reflections<br />
from the<br />
coalface<br />
DR AL O’DYNIA<br />
Department of <strong>Pain</strong><br />
and Snake Oil Medicine<br />
One of our anaesthetic trainees,<br />
who is about to start her pain<br />
module, announced that she<br />
wasn’t sure in which camp she<br />
was going to find herself; that is<br />
whether to be a pain<br />
interventionalist or not. It is a<br />
curious perception of somebody<br />
coming new into the field that<br />
there should be such polarised<br />
positions. How did this<br />
situation come about? In the<br />
past decade we have seen the<br />
rise of evidence-based medicine.<br />
We have of course had some of<br />
the most vocal proponents of<br />
this approach within the field of<br />
pain medicine and perhaps we<br />
are closer to it than some<br />
specialties. What does<br />
evidence-based medicine<br />
actually tell us that is useful in<br />
the field of pain management?<br />
In the field of pain<br />
pharmacology with a number of<br />
good quality studies we are<br />
presented with data in the<br />
forms of numbers-needed-totreat;<br />
this gives a comparison of<br />
effectiveness between drugs,<br />
but may not give us a huge<br />
amount of help when it comes<br />
to treating individual patients.<br />
Patients’ response to analgesics<br />
is often unpredictable and for<br />
reasons that are not at all<br />
apparent some drugs seem to<br />
be highly effective in some<br />
patients and not in others. <strong>The</strong><br />
use of analgesic drugs is often<br />
limited by side-effects, especially<br />
in the elderly, and we often use<br />
drugs in combination as well.<br />
Numbers-needed-to-treat seem<br />
to offer us little help in<br />
choosing a drug therapy beyond<br />
telling us that these drugs have<br />
analgesic properties.<br />
When we move on to chronic<br />
pain interventional therapies the<br />
information provided by<br />
evidence-based medicine<br />
becomes even more difficult to<br />
interpret. To look at the<br />
technique of intravenous<br />
regional sympathetic block, for<br />
example, as evaluated by Drs<br />
McQuay and Moore, there have<br />
been 8 randomised controlled<br />
trials on a total of only 96<br />
patients, each trial used a<br />
different combination of drugs.<br />
It was concluded from this that<br />
intravenous regional<br />
sympathetic blocks were not<br />
supported by the systematic<br />
review. This had led to many<br />
people now not using this<br />
technique; however many <strong>Pain</strong><br />
Clinics around the country<br />
continue to use the technique,<br />
and in combination with a good<br />
hand therapist, find that the<br />
technique gives excellent service<br />
year after year to many<br />
thousands of patients. <strong>The</strong><br />
fundamental problem here is<br />
that what the evidence-based<br />
experts should say to us is that<br />
while there is not enough<br />
evidence to support the use of<br />
intravenous regional blocks,<br />
there is not enough evidence<br />
not to support it either. <strong>The</strong><br />
trials are simply too small and<br />
too disparate to tell us very<br />
much at all. If the authors were<br />
intellectually honest they would<br />
say that there is simply not<br />
enough evidence to comment<br />
on this technique and they<br />
should keep their own counsel<br />
until such time that there is<br />
enough information for them to<br />
provide a useful comment either<br />
way.<br />
However evidence-based<br />
medicine has a strong whiff of<br />
political correctness about it,<br />
which is somewhat inherent in<br />
the title. If you call a form of<br />
medicine evidence-based and<br />
make somewhat dogmatic<br />
statements about what can and<br />
can’t be supported, then<br />
anyone who is practicing<br />
outside that dogma must by<br />
definition be practicing non<br />
evidence-based medicine, akin<br />
to the use of snake oil or similar<br />
preparations. Evidence-based<br />
medicine runs the risk of<br />
becoming mantric and dogmatic<br />
and I detect from speaking to<br />
many colleagues around the<br />
country a definite swing against<br />
the positions and stances<br />
adopted by the proponents of<br />
evidence-based medicine.<br />
In reality in the <strong>Pain</strong> Clinic we<br />
are presented with patients<br />
with difficult clinical problems;<br />
we often have to mix and<br />
match and there is often not a<br />
very clear way or right way<br />
forward in treating patients.<br />
Sometimes we end up using<br />
treatments that we may<br />
normally be uncomfortable<br />
with, such as referring<br />
occasional back pain patients to<br />
spinal surgeons for spinal fusion<br />
(another non-evidence based<br />
pain relieving treatment). <strong>The</strong><br />
correct treatment of course is<br />
the one that works in the<br />
individual patient; from that<br />
point of view, perhaps in the<br />
<strong>Pain</strong> Clinic more than in other<br />
area of medicine, n-of-one trial<br />
is the correct way to treat the<br />
patient and that simply means<br />
in effect trying different<br />
treatments until you find the<br />
one or ones that works. This is<br />
all very well, but what about<br />
the risk? Procedures done in<br />
the <strong>Pain</strong> Clinic are generally of<br />
very low risk, especially when<br />
compared to what many of our<br />
surgical colleagues do. For<br />
example after intravenous<br />
regional sympathetic blocks<br />
some of the patients may suffer<br />
feelings of light-headedness or<br />
perhaps even low blood<br />
pressure, which are transient<br />
and no threat to the patient.<br />
This compares with hip<br />
replacement surgery (another<br />
non-evidence based pain<br />
relieving therapy), where there<br />
is one to two percent mortality<br />
in the pre-operative period and<br />
up to twenty percent serious<br />
morbidity. It is fair to say that<br />
‘no permanent damage’ is a<br />
reliable motto within the <strong>Pain</strong><br />
Clinic. In the past ten years a<br />
series of systematic reviews that<br />
have not supported, or largely<br />
ignored (University of York<br />
review of back pain)<br />
interventional pain relieving<br />
treatments, have led to a period<br />
of intense navel-gazing,<br />
particularly in the pain world,<br />
which has perhaps not served<br />
us well and I suspect has not<br />
served the patients very well<br />
either. I am unaware of my<br />
orthopaedic colleagues being<br />
filled with self doubt about the<br />
value of their procedures,<br />
although their evidence base is<br />
likely to be even thinner than<br />
ours. Evidence-based medicine<br />
in its true form is of course to<br />
be applauded; it may however<br />
be best viewed as an ideal to<br />
which we should aspire, as<br />
when we look at the evidence<br />
base available now it looks very<br />
much like a case of the<br />
Emperor’s new clothes.<br />
I shall say to our new trainee<br />
that there isn’t a right way or a<br />
wrong way to treat patients<br />
with chronic pain, but we<br />
should use all our efforts and as<br />
many techniques, be they<br />
interventional, pharmacological<br />
or psychological, as we have<br />
available to attempt to alleviate<br />
patients’ pain and suffering. It is<br />
the patients after all that we<br />
are here to serve, and not<br />
academic purists in ivory<br />
towers, who have the luxury of<br />
not having to treat patients on<br />
a day-to-day basis.<br />
REFLECTIONS FROM THE COALFACE THE PAIN SOCIETY NEWSLETTER SUMMER 2003 23